0864
Gait retraining as a conservative treatment for medial knee OA: preliminary findings1Department of Radiology, Stanford University, Stanford, CA, United States, 2Musculoskeletal Research Laboratory, VA Palo Alto Healthcare System, Palo Alto, CA, United States, 3Department of Mechanical Engineering, Stanford University, Stanford, CA, United States, 4Department of Bioengineering, Stanford University, Stanford, CA, United States, 5Department of Orthopaedic Surgery, Stanford University, Stanford, CA, United States
Synopsis
Osteoarthritis is a major societal burden and is associated with pain and disability. To cope with the “osteoarthritis epidemic” and its high associated costs, there is a need for new conservative treatments. This study investigates the potential of gait retraining with altered foot progression angle as one inexpensive conservative treatment for medial knee osteoarthritis. Our results show that this treatment may be effective in reducing pain and improving the MRI outcomes in osteoarthritis patients. This suggests the potential of personalized gait retraining with altered foot progression angle as an inexpensive and effective conservative method for the management of osteoarthritis patients.
Introduction
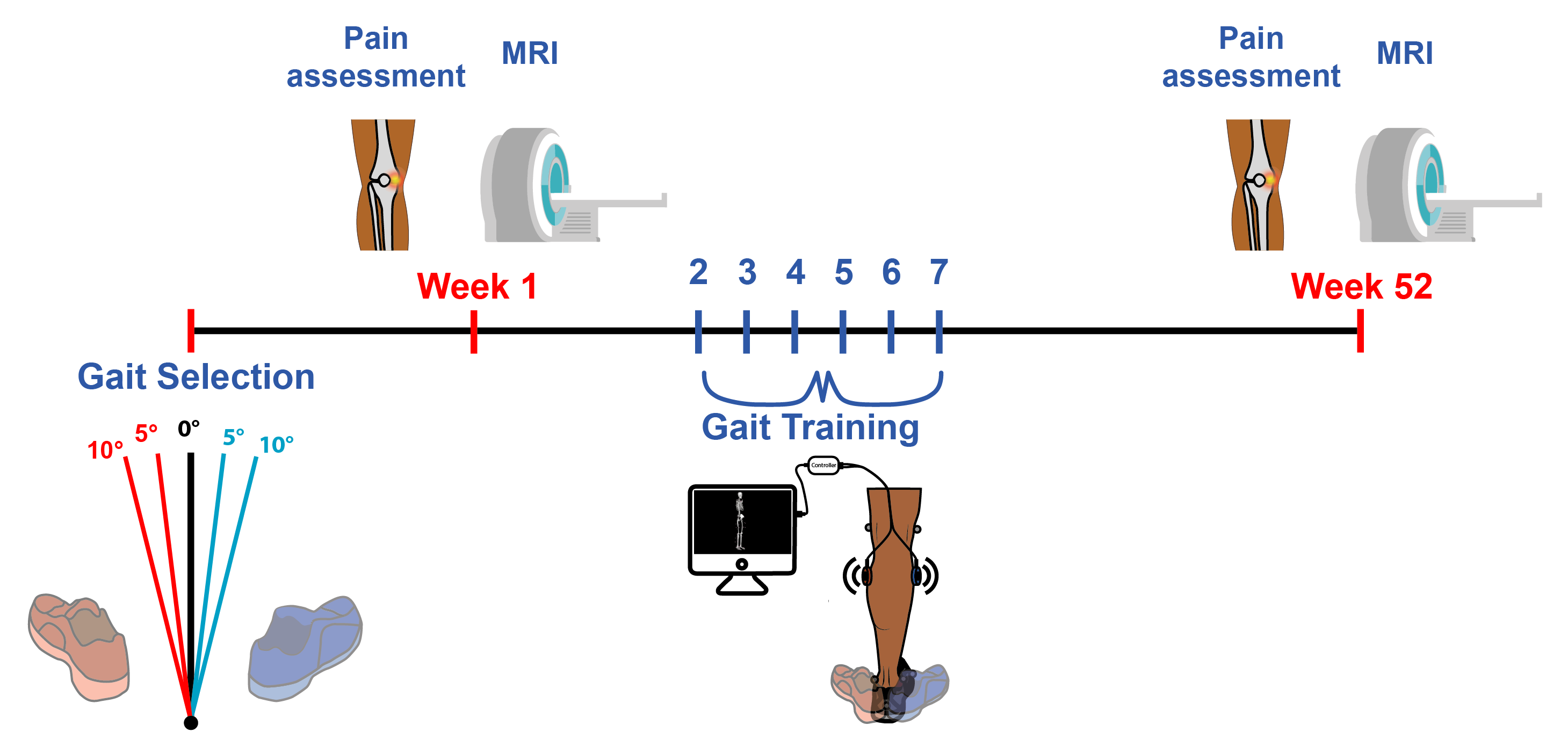
Osteoarthritis (OA) is a major societal burden and is associated with pain and disability. To cope with the “OA epidemic” and its high associated costs, there is a need for new conservative treatments. Current recommended conservative treatments include weight loss and exercise, such as walking. While a daily walking regimen is known to reduce pain from knee OA(1), gait modifications, combined with walking, have the potential to provide larger benefits as compared to walking alone. In particular, modification of foot progression angle (FPA, Figure 1) in a patient-specific fashion has been shown to reduce the knee adduction moment (KAM), a surrogate measure for medial-compartment loading, in healthy subjects(2). This reduction of excessive forces in the medial compartment achieved with personalized gait retraining strategies could be beneficial in reducing the symptoms of knee OA and slowing disease progression. The aim of this study is to determine whether a personalized gait retraining strategy, consisting of a modification of the FPA in a patient-specific fashion, can provide an additional long-term benefit to OA patients compared with walking alone.Methods
Twenty-one subjects were included in this longitudinal study (Figure 1). Inclusion criteria were medial compartment knee OA (KL grade = 1, 2, 3), age 18-80 years, able to walk without aids for at least 25 minutes, and ability to reduce the most prominent KAM peak by at least 5%. Subjects were excluded if they had history of joint replacement or BMI≥35.
The subjects were randomly assigned to either a KAM-reducing (altered FPA, n=12) or a control (consistent FPA, n=9) group. Both groups participated in weekly treadmill walking sessions for 6 weeks where they were given vibrotactile biofeedback to walk accurately with their personalized FPA(3); the altered FPA group was prescribed the angle that maximally reduced their peak KAM, and the control group was prescribed their natural FPA (Figure 1).
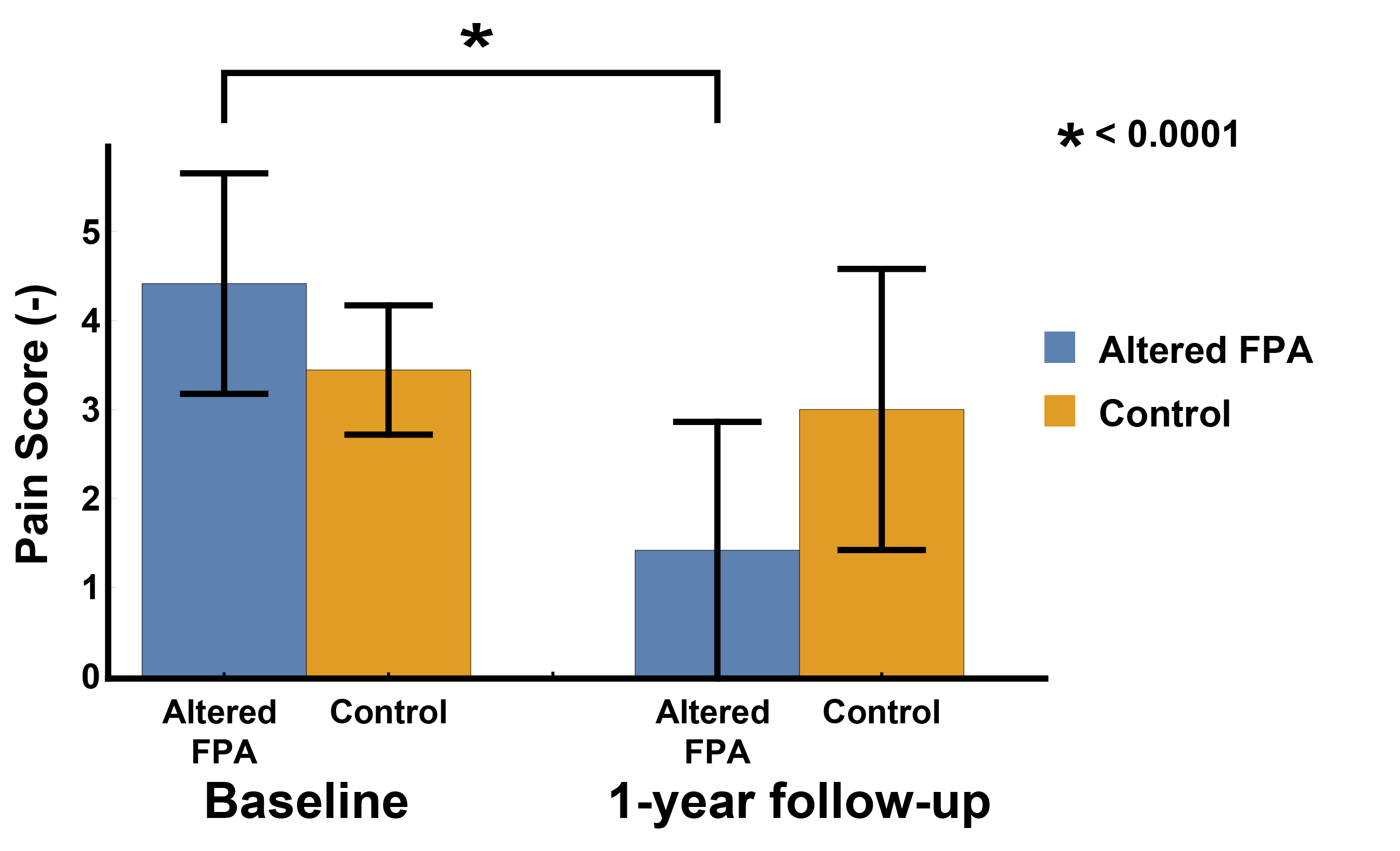
Medial knee pain was evaluated using a numeric rating scale (0 = no pain; 10 = worst pain imaginable) at baseline and at 1-year follow-up.
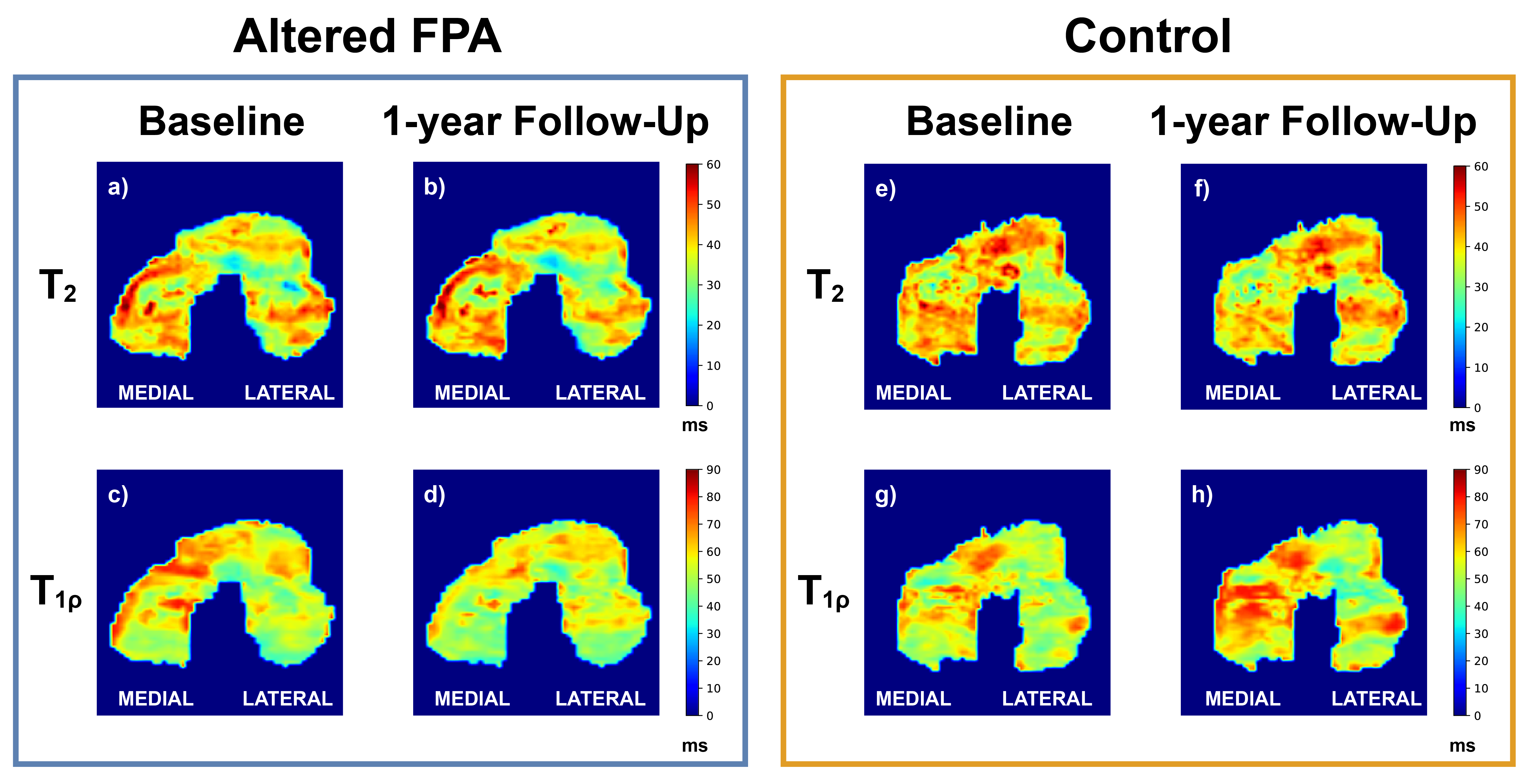
MRI examination was carried out at baseline and 1-year follow-up to measure T1ρ and T2. All scans were performed at 3T (GE DISCOVERY MR750) using a 16ch phased-array flexible coil. T1ρ relaxation times were estimated using a magnetization-prepared pseudo-steady-state 3D FSE sequence ( FSL= 500 Hz, TR/TE=1292/16 ms, FA=90°, FOV=160x160x120 mm3, voxel size = 0.5x0.625x3 mm3, TSL=1, 10, 30, 60 ms, total scan time=5min12s). T1ρ values were calculated pixelwise using a monoexponential decay model. T2 relaxation times were estimated using a 3D DESS sequence (TR=24.96 ms, TE1/ TE2=7.54/42.38 ms, FA=30°, FOV=160x160x120 mm3, voxel size = 0.3125x0.3125x1.5 mm3, scan time=5min32s).T2 was calculated from the two DESS echoes(4).
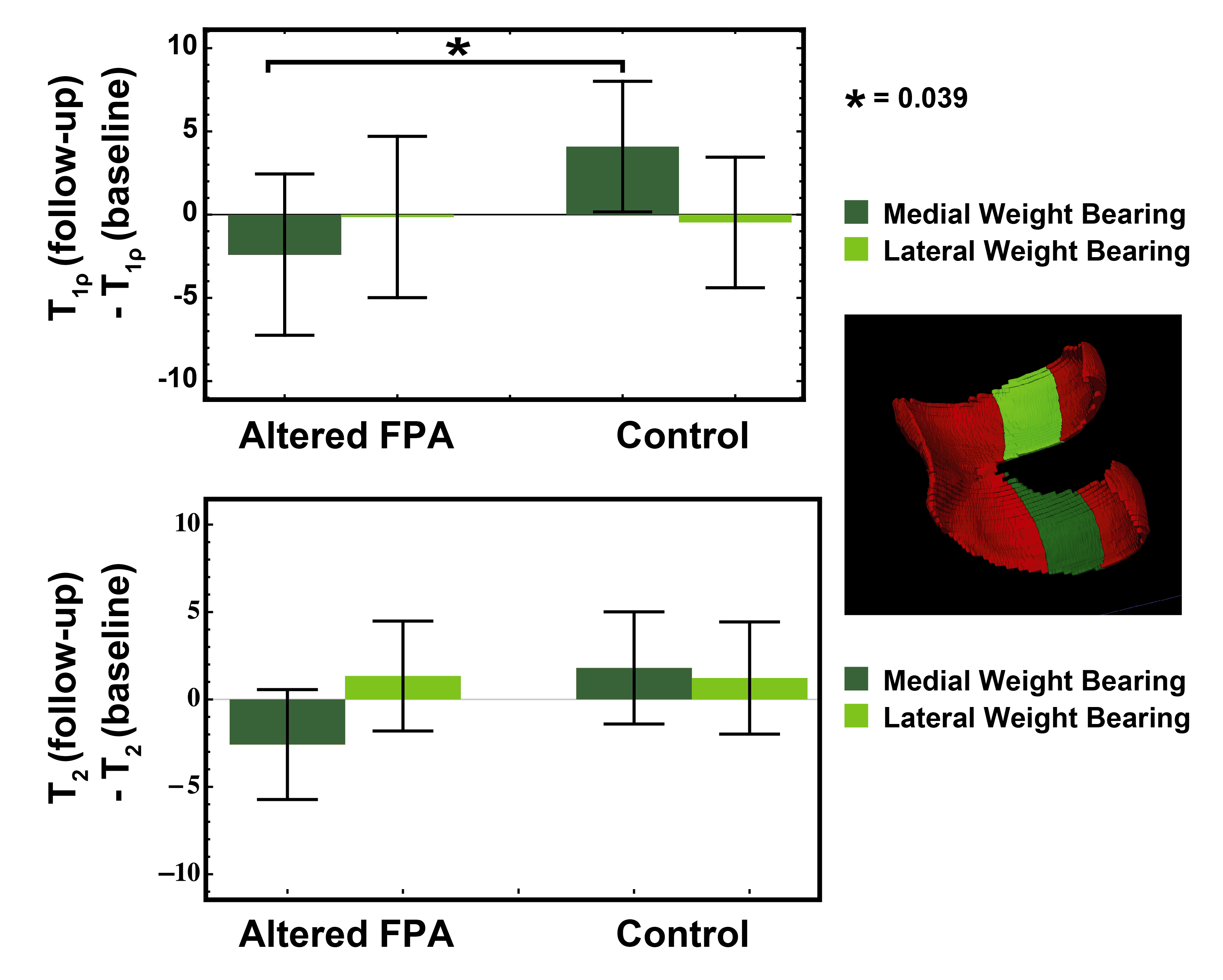
The medial and lateral weight-bearing regions were manually segmented on the DESS scan (see Figure 4) for each subject at baseline. Subsequently, T1ρ scans at baseline and the DESS and T1ρ scans at follow-up were non-rigidly registered to the DESS scan at baseline and average pixelwise difference was calculated for the two compartments. Differences in relaxation times and pain scores over time were assessed using a General Linear Model. A p-value of 0.05 was considered to be significant.
Results
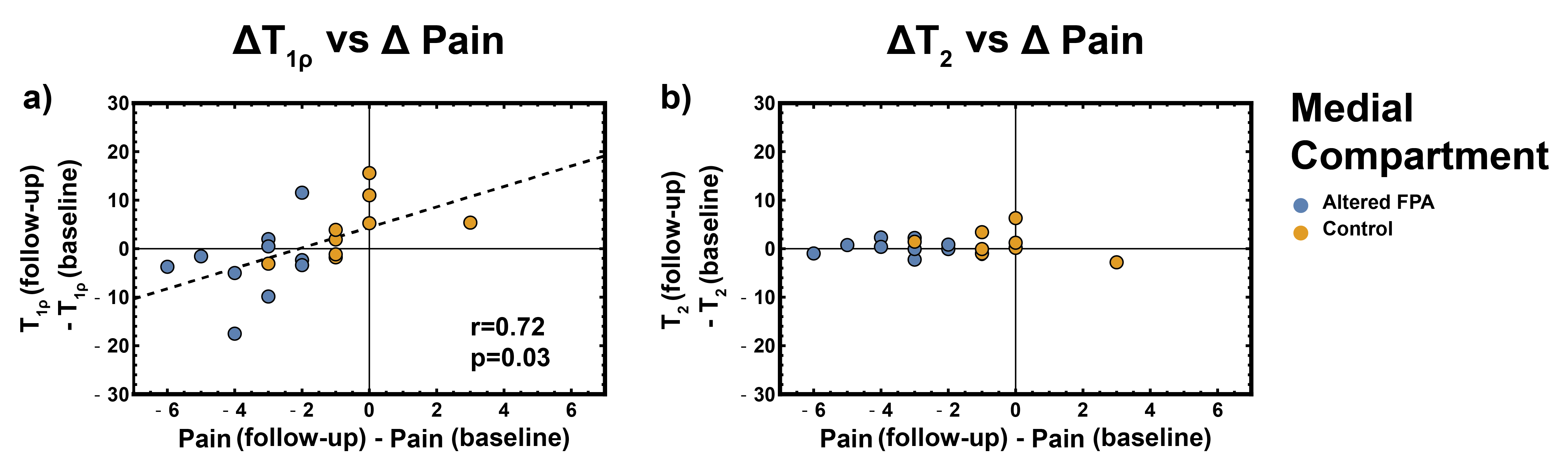
Subjects in the altered FPA group reported significantly lower pain (p<0.0001) at follow-up, as compared to controls (Figure 2). A small increase in T1ρ over time was observed in the control group, indicating disease progression. A significantly different behavior was observed in the altered FPA group (p=0.039), with a small reduction in T1ρ after treatment (Figure 3 and 4). A strong correlation (r=0.72, p=0.03) was observed with changes in pain and changes in T1ρ over time, with pain reduction associated with a reduction in T1ρ values in the medial compartment in the altered FPA group (Figure 5).Discussion and Conclusions
Our preliminary results indicate that adopting a modified FPA that reduces the KAM can decrease the pain in the medial compartment in knee OA more than walking alone. Furthermore, a personalized FPA modification appears to slow down the disease progression in the medial compartment, as indicated by the different time evolution of T1ρ in altered FPA and control groups. These modifications could be associated with proteoglycan regeneration with load reduction, but the causes of these changes warrant further investigation.
This study has a limited sample size. Nonetheless, our preliminary results suggest the potential of personalized gait retraining with altered FPA as an inexpensive and effective conservative method for the management of knee OA patients. Further, it demonstrates the potential of quantitative MRI to detect tissue-level cartilage changes associated with changes in joint mechanics to evaluate the potential of conservative disease-modifying therapies.
Acknowledgements
This work was supported in part by Merit Review Award Number I01 RX001811 from the United States Department of Veterans Affairs Rehabilitation R&D Service.References
1. Roddy E: Evidence-based recommendations for the role of exercise in the management of osteoarthritis of the hip or knee--the MOVE consensus. Rheumatology 2005; 44:67–73.
2. Uhlrich SD, Silder A, Beaupre GS, Shull PB, Delp SL: Subject-specific toe-in or toe-out gait modifications reduce the larger knee adduction moment peak more than a non-personalized approach. J Biomech 2017; 66:103–110.
3. Shull PB, Lurie KL, Cutkosky MR, Besier TF: Training multi-parameter gaits to reduce the knee adduction moment with data-driven models and haptic feedback. J Biomech 2011; 44:1605–1609.
4. Sveinsson B, Chaudhari AS, Gold GE, Hargreaves BA: A simple analytic method for estimating T2 in the knee from DESS. Magn Reson Imaging 2017; 38:63–70.
Figures