0854
Low extracellular acidification in 1p/19q co-deleted gliomas confirmed using pH-weighted amine CEST-EPI, T2 relaxometry, and amino acid PET1Brain Tumor Imaging Laboratory (BTIL), Center of Computer Vision and Imaging Biomarker, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 2Department of Bioengineering, Henry Samueli School of Engineering and Applied Science, University of California, Los Angeles, Los Angeles, CA, United States, 3Department of Radiological Sciences, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 4Department of Neurosurgery, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 5UCLA Brain Research Institute (BRI), David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 6Department of Neurology, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 7Physics and Biology in Medicine, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 8Department of Psychiatry and Biobehavioral Sciences, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
The 1p/19q co-deletion in gliomas is associated with better response to therapies and better patient prognosis. In this study, we demonstrate that 1p/19q co-deleted gliomas are less acidic than gliomas with intact 1p/19q using a combination of pH-sensitive amine CEST-EPI, T2 relaxometry, and 18F-FDOPA PET. Results suggest amine CEST-EPI may serve as a quick non-invasive imaging biomarker for identifying 1p/19q co-deleted tumors. Our results also support the hypothesis that the better prognosis and higher sensitivity to treatment of 1p/19q co-deleted gliomas may be related to less acidity in tumor microenvironment.
INTRODUCTION
The co-deletion of the short arm of chromosome 1 (1p) and the long arm of chromosome 19 (19q) is the molecular hallmark of oligodendroglioma, which is present in about 60-90% histopathologically diagnosed oligodendroglioma and 30-50% of mixed oligoastrocytoma1,2. In addition to its diagnosis value, the 1p/19q co-deletion is also associated with better response to radiotherapy and alkylating agent chemotherapy3,4,5, longer progression free survival, and prolonged overall survival6,7. However, the biological basis of these prognosis differences is not well understood. Blough et al. found that silencing of a pH regulator, NHE-1 is associated with DNA hypermethylation and 1p allelic loss, consequently impairs the ability of tumor cells to neutralize the acidosis generated by the Warburg glycolytic shift8. In terms of non-invasive imaging characteristics, 1p/19q co-deleted gliomas tend to have heterogeneous signal intensity, indistinct margin, and calcification on anatomic images9,10. Studies using advanced MRI and metabolic imaging show that 1p/19q co-deleted gliomas have higher relative cerebral blood volume (rCBV) and increased uptake of 18F-FDG (fluorine-18 fluorodeoxyglucose), 11C-MET (carbon-11 methionine), and 18F-FET (fluorine-18 fluoro-ethyl-tyrosine)11,12,13,14. However, no studies to date have examined potential differences in extracellular acidity arising between 1p/19q codeleted and intact gliomas due to differences in glycolysis non-invasively in human glioma patients.
Amine CEST EPI is a fast chemical exchange saturation transfer (CEST) imaging technique that is sensitive to decreased extracellular pH, transverse relaxation rate, and amino acid concentration15. Acidification of the tumor microenvironment has been shown to correspond with increased tumor aggressiveness, enhanced invasion, and resistance to various therapies16. In this study, we demonstrate that 1p/19q co-deleted gliomas are less acidic than gliomas with intact 1p/19q using a combination of pH-sensitive amine CEST-EPI, T2 relaxometry, and 18F-FDOPA (fluorine-18 fluoro-L-dopa) amino acid PET.
METHODS
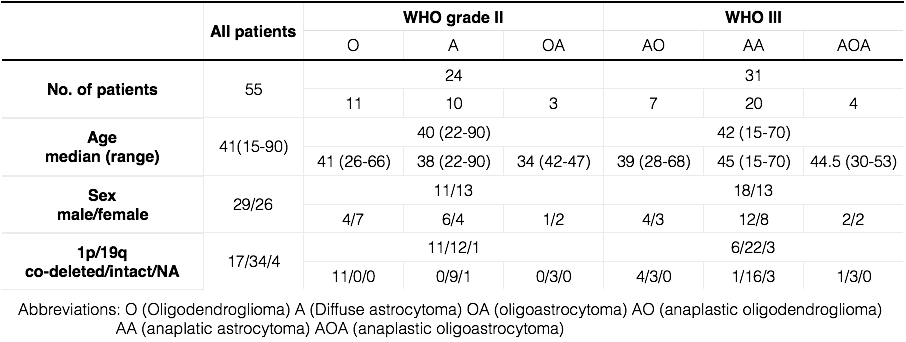
Patient: A total of 55 histologically confirmed glioma patients (World Health Organization WHO II, N=24; WHO III, N=31) were enrolled in this retrospective study. A detailed patient demographics is in Table 1. The 1p/19q status was determined with fluorescent in situ hybridization (FISH) on biopsy/surgical resection tissue. Amine CEST-EPI: pH-weighting amine CEST-EPI images were collected with single echo CEST-EPI sequence15 or CEST spin-and-gradient-echo (SAGE)-EPI sequence17. Off-resonance saturation was applied using a pulse train of 3x100ms Gaussian pulses with peak amplitude of 6µT. Post processing of CEST data consists of motion correction, z-spectra based B0 correction, followed by the calculation of magnetization transfer ratio asymmetry (MTRasym) at amine proton resonance frequency (3.0ppm) as the metric of CEST contrast. 18F-FDOPA: 15 out of the 55 patients received an 18F-FDOPA amino acid PET scan within three months of amine CEST-EPI. FDOPA images were registered to anatomic MRI and normalized to mean signal intensity in basal ganglia. T2 relaxometry: 28 out of the 55 patients received CEST-MRI scan with a multi-echo SAGE-EPI readout. The signal intensity from the various echoes were used to estimate T2. Data Analysis: Mann-Whitney u-test is performed to evaluate the difference in MTRasym, FDOPA, and T2 within T2 hyperintensity lesions, comparing 1p/19q co-deleted and intact gliomas.RESULTS
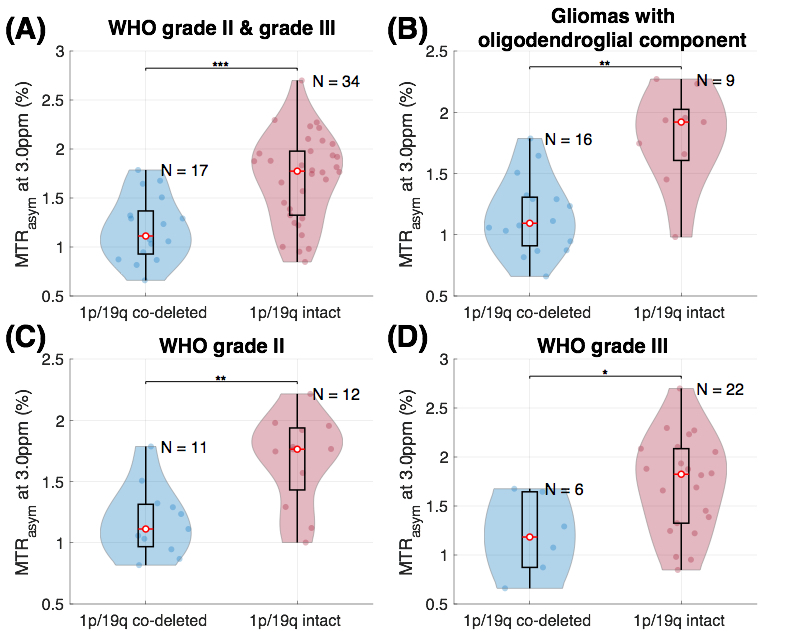
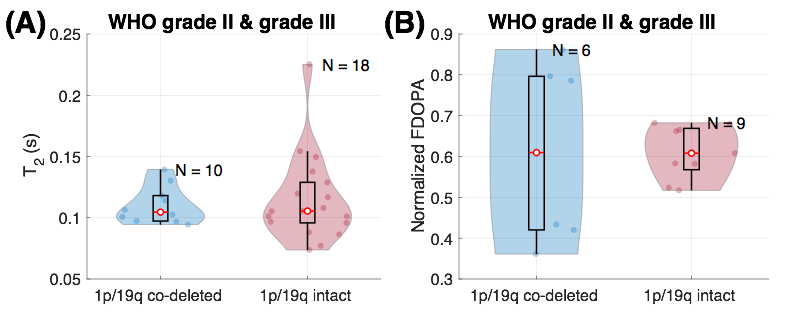
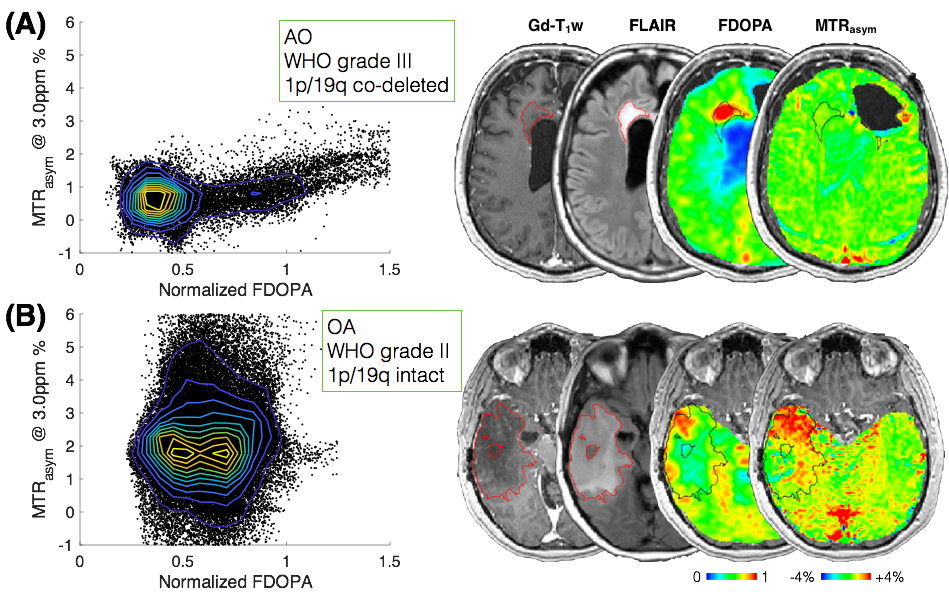
Median MTRasym at 3ppm within T2 hyperintense lesions were significantly lower in 1p/19q co-deleted gliomas compared to 1p/19q intact ones (co-deleted: 1.19±0.32%; intact: 1.70±0.45%; p = 0.00018, Figure 1 (A)). The significantly lower MTRasym persists when comparing within grade II (p = 0.0062, Figure 1 (C)) and grade III (p = 0.027, Figure 1 (D)). Within gliomas exhibiting classical oligodendroglial histological features (including olidodendroglioma, oligodendrocytoma, anaplastic olidodendroglioma, and anaplatic oligodendrocytoma), the MTRasym is significantly lower in 1p/19q co-deleted tumors compared to intact ones (p = 0.0017, Figure 1 (B)). The ROC analysis shows that prediction of 1p/19q status using median MTRasym within T2 hyperintensity lesion has sensitivity of 76.5%. specificity of 76.5%, and area under the curve (AUC) of 0.83. FDOPA and T2 in T2 hyperintense lesions were not different between1p/19q co-deleted and intact tumors (FDOPA: p = 0.94; T2: p = 1, Figure 2). Two examples of MTRasym vs. FDOPA are demonstrated in Figure 3, showing the characteristic difference between 1p/19q co-deleted and intact gliomas.DISCUSSION AND CONCLUSION
Results suggest that 1p/19q co-deleted gliomas have notably lower acidity compared with intact gliomas, as indicated by lower MTRasym at 3.0ppm and no differences in amino acid concentration or transverse relaxation rates. Results further suggest that amine CEST-EPI may serve as a quick non-invasive imaging biomarker for identifying 1p/19q co-deleted tumors. Interestingly, the difference in acidity is more specific to 1p/19q status than to the histological feature of glioma. Further, results suggest the better prognosis and higher sensitivity to treatment of 1p/19q co-deleted gliomas may be related to less acidity in tumor microenvironment.Acknowledgements
No acknowledgement found.References
1. van den Bent MJ. Anaplastic oligodendroglioma and oligoastrocytoma. Neurol Clin 2007; 25: 1089–109.
2. Koeller KK, Rushing EJ. From the archives of the AFIP: oligodendroglioma and its variants: radiologic-pathologic correlation. Radiographics 2005; 25: 1669–88.
3. Cairncross G, Berkey B, Shaw E, et al. Phase III trial of chemotherapy plus radiotherapy compared with radiotherapy alone for pure and mixed anaplastic oligodendroglioma: Intergroup Radiation Therapy Oncology Group Trial 9402. J Clin Oncol. 2006;24:2707–2714.
4. Van den Bent MJ, Carpentier AF, Brandes AA, et al. Adjuvant procarbazine, lomustine, and vincristine improves progression-free survival but not overall survival in newly diagnosed anaplastic oligodendrogliomas and oligoastrocytomas: a randomized European Organisation for Research and Treatment of Cancer phase III trial. J Clin Oncol. 2006;24:2715–2722.
5. WickW, Hartmann C, Engel C, et al. NOA-04 randomized phase III trial of sequential radiochemotherapy of anaplastic glioma with PCV or temozolomide. J Clin Oncol. 2009;27:5874–5880.
6. Engelhard HH, Stelea A, Cochran EJ. Oligodendroglioma: pathology and molecular biology. Surg Neurol 2002; 58: 111–7; discussion 117.
7. Engelhard HH, Stelea A, Mundt A. Oligodendroglioma and anaplastic oligodendroglioma: clinical features, treatment, and prognosis. Surg Neurol 2003; 60: 443–56.
8. Blough MD, Al-Najjar M, Chesnelong C, et al. DNA hypermethylation and 1p loss silence NHE-1 in oligodendroglioma. Ann Neurol. 2012;71:845–849.
9. Kim JW, Park CK, Park SH, Kim YH, Han JH, Kim CY, et al. Relationship between radiological characteristics and combined 1p and 19q deletion in World Health Organization grade III oligodendroglial tumours. J Neurol Neurosurg Psychiatry 2011; 82: 224–7.
10. Jenkinson MD, du Plessis DG, Smith TS, Joyce KA, Warnke PC, Walker C. Histological growth patterns and genotype in oligodendroglial tumours: correlation with MRI features. Brain Engl 2006; 129(Pt 7): 1884–91.
11. Kapoor GS, Gocke TA, Chawla S, Whitmore RG, Nabavizadeh A, Krejza J, et al. Magnetic resonance perfusion-weighted imaging defines angiogenic subtypes of oligodendroglioma according to 1p19q and EGFR status. J Neurooncol 2009; 92: 373–86.
12. Stockhammer F, Thomale UW, Plotkin M, Hartmann C, Von Deimling A. Association between fluorine-18-labeled fluorodeoxyglucose uptake and 1p and 19q loss of heterozygosity in World Health Organization Grade II gliomas. J Neurosurg 2007; 106: 633–7.
13. Jansen NL, Schwartz C, Graute V, Eigenbrod S, Lutz J, Egensperger R, et al. Prediction of oligodendroglial histology and LOH 1p/19q using dynamic [(18)F]FET-PET imaging in intracranial WHO grade II and III gliomas. Neuro Oncol 2012; 14: 1473–80.
14. Saito T, Maruyama T, Muragaki Y, Tanaka M, Nitta M, Shinoda J, et al. 11C-methionine uptake correlates with combined 1p and 19q loss of heterozygosity in oligodendroglial tumors. AJNR Am J Neuroradiol 2013; 34: 85–91.
15. Harris RJ, Cloughesy TF, Liau LM, et al. Simulation, phantom validation, and clinical evaluation of fast pH-weighted molecular imaging using amine chemical exchange saturation transfer echo planar imaging (CEST-EPI) in glioma at 3 T. NMR Biomed 2016;29:1563-1576
16. DeClerck K, Elble RC. The role of hypoxia and acidosis in promoting metastasis and resistance to chemotherapy. Front Biosci. 2010 Jan 1;15:213-25.
17. Harris RJ, Yao J, Chakhoyan A, Raymond C, Leu K, Liau LM, Nghiemphu PL, Lai A, Salamon N, Pope WB, Cloughesy TF. Simultaneous pH-sensitive and oxygen-sensitive MRI of human gliomas at 3T using multi-echo amine proton chemical exchange saturation transfer spin-and-gradient echo echo-planar imaging (CEST-SAGE-EPI). Magnetic resonance in medicine. 2018 Apr 6.
Figures