0848
Quantification of cerebral perfusion fraction map using cardiac-triggered, off-resonance calibrated super-selective arterial spin labeling1Biomedical Engineering, University of Michigan, Ann Arbor, MI, United States, 2Surgery, University of Michigan, Ann Arbor, MI, United States, 3FMRI Laboratory, University of Michigan, Ann Arbor, MI, United States
Synopsis
The impact of off-resonance compensation and cardiac triggering on vessel- selective ASL labeling efficiency and image quality was investigated. A strategy to calculate individual vessel’s perfusion fraction maps based on measurements of vessel-selective labeling efficiency is also presented. This work serves as a practical guideline for acquiring high quality, quantitative perfusion fraction maps with super-selective pseudo-continuous arterial spin labeling.
Introduction
Perfusion measurements of vascular territories in the brain offer critical clinical information on cerebrovascular function. In the presence of steno-occlusive cerebrovascular disease, perfusion fraction maps can be used to identify and evaluate collateral flow pathways1,2. Recently, pseudo-continuous arterial spin labeling (PCASL) was extended to include vessel-selective labeling to map perfusion territories3,4. In super-selective PCASL (SS-PCASL), additional in-plane gradient blips create a circular labeling spot which can be placed on arteries. Clinical application of SS-PCASL has been limited5,6 due to challenges that can significantly decrease labeling efficiency, image quality, and overall accuracy perfusion maps. SS-PCASL generally suffers from low SNR due to an inherently lower labeling efficiency compared to standard PCASL3, particularly noticeable in low-flow vessels such as the vertebral arteries. Primary causes for reduced labeling efficiency are off-resonance, pulsatility, and vessel movement. Consequently, there is a need to maximize labeling efficiency and to assess efficiency differences between vessels in order to produce accurate, quantitative perfusion fractions, especially in voxels with mixed perfusion. In this work, the impact of off-resonance compensation and cardiac-triggering on SS-PCASL labeling efficiency and image quality is investigated and a strategy to calculate the perfusion fraction map based on label efficiency measurements is presented.Methods
Maximizing Labeling efficiency and image quality. The effects of off-resonance and pulsatility were investigated in 10 subjects.
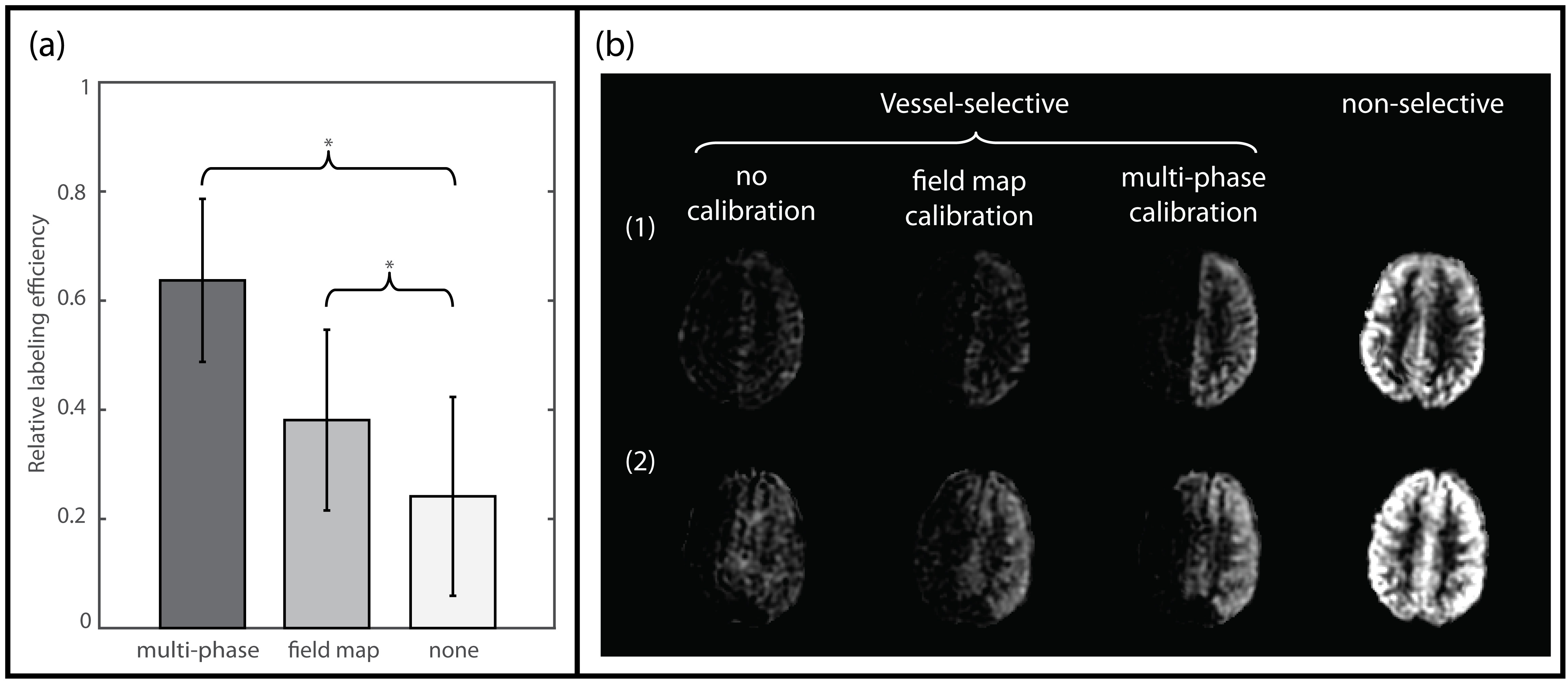
Two off-resonance compensation strategies, a multi-phase pre-scan and a field map, were compared by acquiring SS-PCASL images of the left carotid artery. The multi-phase pre-scan consisted of a non-selective PCASL with increasing RF-phase increments after each label/control pair (Fig. 1a). A field map was collected in the location of the PCASL label plane to measure the off-resonance directly (Fig. 1b). A comparison was performed by calculating a mean labeling efficiency relative to a non-selective PCASL image.
Two sets of SS-PCASL images of the dominant vertebral artery were collected with and without cardiac triggering. In the cardiac-triggered SS-PCASL scan, the start of the saturation pulse before the label train was triggered by a peripheral pulse oximeter7. A spatial and temporal SNR, as well as a CNR were calculated inside and outside the posterior perfusion territory. A qualitative comparison was conducted by 3 objective observers.
Calculating a perfusion fraction map. Cardiac-triggered SS-PCASL images of all neck arteries were acquired in two volunteers after a TOF and multi-phase calibration pre-scan. Labeling efficiency was directly measured 2 cm above the label plane. Vessel-averaged labeling efficiency was obtained by compensating for T1-decay during transit and calculating a velocity-weighted average across the vessel. Perfusion fraction maps were generated by scaling each vessel-selective subtraction image by its corresponding label efficiency and dividing it by the sum of all the vessel-selective subtraction images.
Results
Off-resonance: Multi-phase calibration and field map acquisition yielded statistically significant increases in labeling efficiency (p=0.0020 and p=0.0371, respectively) compared to the non-calibrated scan (Fig. 2a). The multi-phase calibrated scan resulted in higher labeling efficiency compared to the field map approach (p=0.0020). Fig. 2b illustrates the resulting left carotid perfusion territories for two subjects.
Cardiac triggering: A qualitative comparison resulted in equal or improved image quality with cardiac triggering in 6.7 out of 10 subjects. Fig. 3 illustrates the reduction of pulsatility artifacts with cardiac triggering in a subject. Cardiac triggering did not result in a significant improvement in spatial or temporal SNR. However, there was a significant change in CNR between the vascular territory and the surrounding regions.
Quantitative perfusion fraction map: Fig. 4 shows the perfusion fractions for a subject with a posterior circulation dominated by the left vertebral artery (a) and a subject with a missing basilar artery (b). These findings are consistent with the TOF images.
Discussion and conclusions
Both off-resonance calibration strategies showed a significant increase in labeling efficiency. While the field map method captured the off-resonance due to B0-field inhomogeneity, the multi-phase pre-scan method also captured additional imperfections in the magnetic field induced by the PCASL label train itself and resulted consistently in the highest labeling efficiency.
Pulsatility artifacts can significantly affect the image quality and the estimation of perfusion fraction maps. Qualitative inspection of the mean subtraction images showed a reduction in arterial artifacts and overall improved image quality with cardiac triggering. Changes in heart rate between label and control images can lead to imperfect subtractions and reduce the efficacy of cardiac triggering.
The scaled perfusion fraction maps based on our proposed strategy showed the perfusion territory of each vessel clearly. In mixed perfusion territories, such as the posterior circulation, perfusion fractions were in line with TOF images.
Acknowledgements
No acknowledgement found.References
[1] X. V Richter, X.M. Helle, X.M.J.P. Van Osch, X.T. Lindner, X.A.S. Gersing, X.P. Tsantilas, X.H. Eckstein, X.C. Preibisch, ADULT BRAIN MR Imaging of Individual Perfusion Reorganization Using Superselective Pseudocontinuous Arterial Spin-Labeling in Patients with Complex Extracranial Steno-Occlusive Disease, (2017) 1–9.
[2] P.J. Van Laar, J. Hendrikse, W.P.T.M. Mali, F.L. Moll, H.B. van der Worp, M.J.P. van Osch, J. van der Grond, Altered flow territories after carotid stenting and carotid endarterectomy, J. Vasc. Surg. 45 (2007) 1155–1161. doi:10.1016/j.jvs.2006.11.067.
[3] M. Helle, D.G. Norris, S. Rüfer, K. Alfke, O. Jansen, M.J.P. Van Osch, Superselective pseudocontinuous arterial spin labeling, Magn. Reson. Med. 64 (2010) 777–786. doi:10.1002/mrm.22451.
[4] E.C. Wong, Vessel-encoded arterial spin-labeling using pseudocontinuous tagging, Magn. Reson. Med. 58 (2007) 1086–1091. doi:10.1002/mrm.21293.
[5] M. Helle, S. Rüfer, M.J.P. Van Osch, A. Nabavi, K. Alfke, D.G. Norris, O. Jansen, Superselective arterial spin labeling applied for flow territory mapping in various cerebrovascular diseases, J. Magn. Reson. Imaging. 38 (2013) 496–503. doi:10.1002/jmri.24041.
[6] T. Lin, Z. Lai, Y. Lv, J. Qu, Z. Zuo, H. You, B. Wu, B. Hou, C. Liu, F. Feng, Effective collateral circulation may indicate improved perfusion territory restoration after carotid endarterectomy, Eur. Radiol. (2017) 1–9. doi:10.1007/s00330-017-5020-8.
[7] Y. Li, D. Mao, Z. Li, M. Schär, J.J. Pillai, J.G. Pipe, H. Lu, Cardiac-triggered pseudo-continuous arterial-spin-labeling: A cost-effective scheme to further enhance the reliability of arterial-spin-labeling MRI, Magn. Reson. Med. 00 (2018). doi:10.1002/mrm.27090.
Figures