0846
Glomerular filtration rate estimation by motion-robust high spatiotemporal resolution DCE-MRI with radial VIBE and comparison with plasma clearance of 99mTc-DTPA1Radiology, Boston Children's Hospital and Harvard Medical School, Boston, MA, United States, 2Siemens Healthcare, Erlangen, Germany, 3Urology, Boston Children's Hospital and Harvard Medical School, Boston, MA, United States
Synopsis
The accuracy of MRI based glomerular filtration rate (GFR) measurements using the standard Cartesian VIBE DCE-MRI is limited by motion and temporal resolution. Instead, we use motion-robust high temporal resolution radial VIBE for DCE-MRI for accurate estimation of GFR. We optimize its temporal resolution and compressed sensing reconstruction temporal regularization parameters to obtain an accurate arterial input function peak while reconstructing good quality images. We also developed a fully automated segmentation and tracer kinetic model-fitting pipeline to compute MRI-GFR. We assessed the accuracy of proposed technique to measure GFR by comparing MRI-GFR to GFR from 99mTcDTPA nuclear medicine study (NMGFR).
Introduction
Dynamic Contrast Enhanced (DCE) MRI can be used to measure renal function, i.e. glomerular filtration rate (GFR). DCE-MRI using standard Cartesian-VIBE has several limitations including 1) respiratory motion in free-breathing scans which reduces image quality and significantly lowers the accuracy of MRI-GFR estimates; 2) insufficient temporal resolution, which results in a failure to measure the arterial input function (AIF) peak needed for accurate estimates of GFR because AIF changes rapidly after contrast injection; 3) a lack of specialized software for fully automated segmentation of kidney parenchyma, aorta and for performing tracer kinetic model fitting for robust GFR estimation. In this work, we use a motion-robust high spatiotemporal resolution DCE-MRI using dynamic radial VIBE (DRV) sequence, compressed-sensing offline-reconstruction using temporal regularization and a fully automated processing pipeline to measure MRI-GFR. We optimize the parameters (temporal resolution and regularization) to achieve accurate GFR estimation and good image quality at the same time. We then assess the accuracy of measuring GFR with this technique by comparison of MRI-GFR to gold standard GFR from 99mTcDTPA nuclear medicine study (NM-GFR).Methods
Children, between 0-20 years, undergoing both a clinically indicated contrast-enhanced MRI, and a nuclear medicine GFR study within 2 weeks of each other, underwent an IRB approved additional 6-minute DCE-MRI kidney scan using the motion-robust high spatiotemporal resolution dynamic radial VIBE sequence (3T Siemens Skyra/Trio, radial “stack-of-stars” 3D FLASH prototype Siemens sequence with TR/TE/FA 3.56/1.39ms/12o, 32 coronal slices, voxel size=1.25x1.25x3mm, 1326 radial spokes in 6 mins, golden angle radial ordering). Contrast was injected using bolus injection (0.2ml/s). 4D dynamic image series were reconstructed offline using compressed-sensing reconstruction1 (using the Matlab code provided by NYU that we modified) to improve image quality, effectively reducing the streaking artifacts. We analyzed the effect of regularization parameter and temporal resolution on the AIF peak and image quality and chose the optimal parameters that satisfied both criteria.
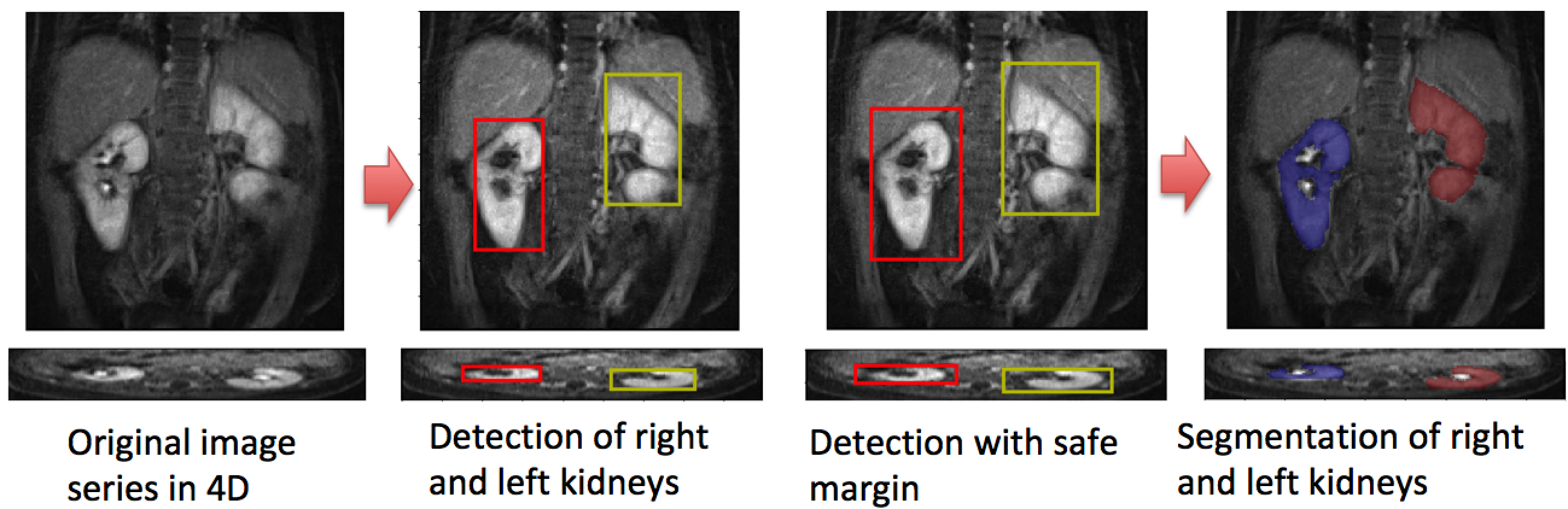
Images were automatically post-processed using in-house developed software. Post-processing steps included segmentation of kidney parenchyma2 and aorta using fully convolutional neural network (F-CNN) techniques. Figure 2 shows the cascaded detection and segmentation steps for segmentation of left and right kidneys using a F-CNN2. The steps included: 1) detection of left and right kidneys given a time series of 3D volumes (4D data); 2) generating a safer enlarged bounding box and 3) segmentation of each kidney. Before detection, we applied PCA to reduce the time dimension and downsampling in spatial dimensions for memory efficiency. After segmentation, we converted the tissue enhancement curves of aorta and kidneys to concentration curves, selected aorta voxels with largest peak and fitted Sourbron et al.’s3 separable two-compartment tracer kinetic model to compute the filtration rate parameter (FT). MRI-GFR is calculated by multiplying FT with renal parenchyma volume. The MRI-GFR results were compared to the GFR measured by 99mTcDTPA nuclear medicine study (NMGFR).
Results
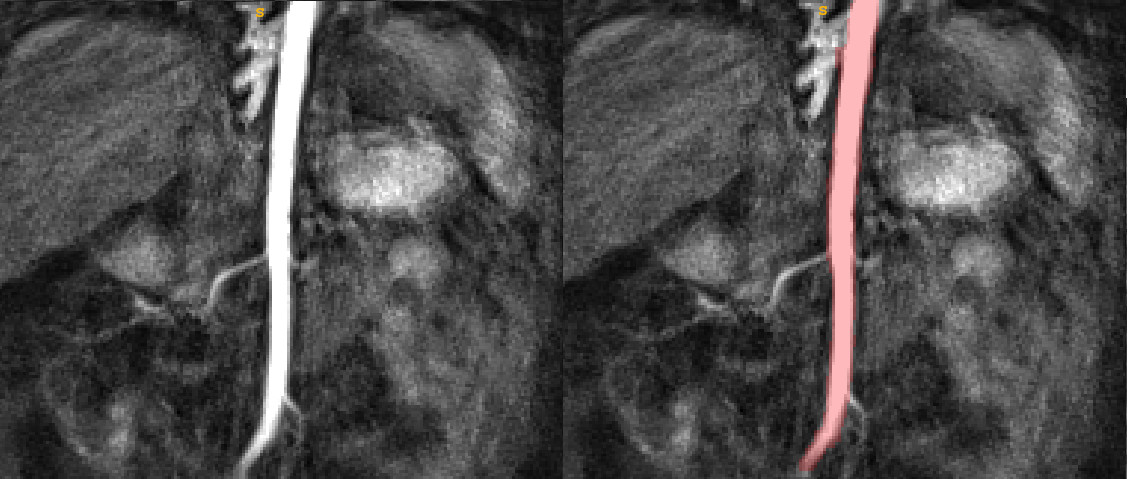
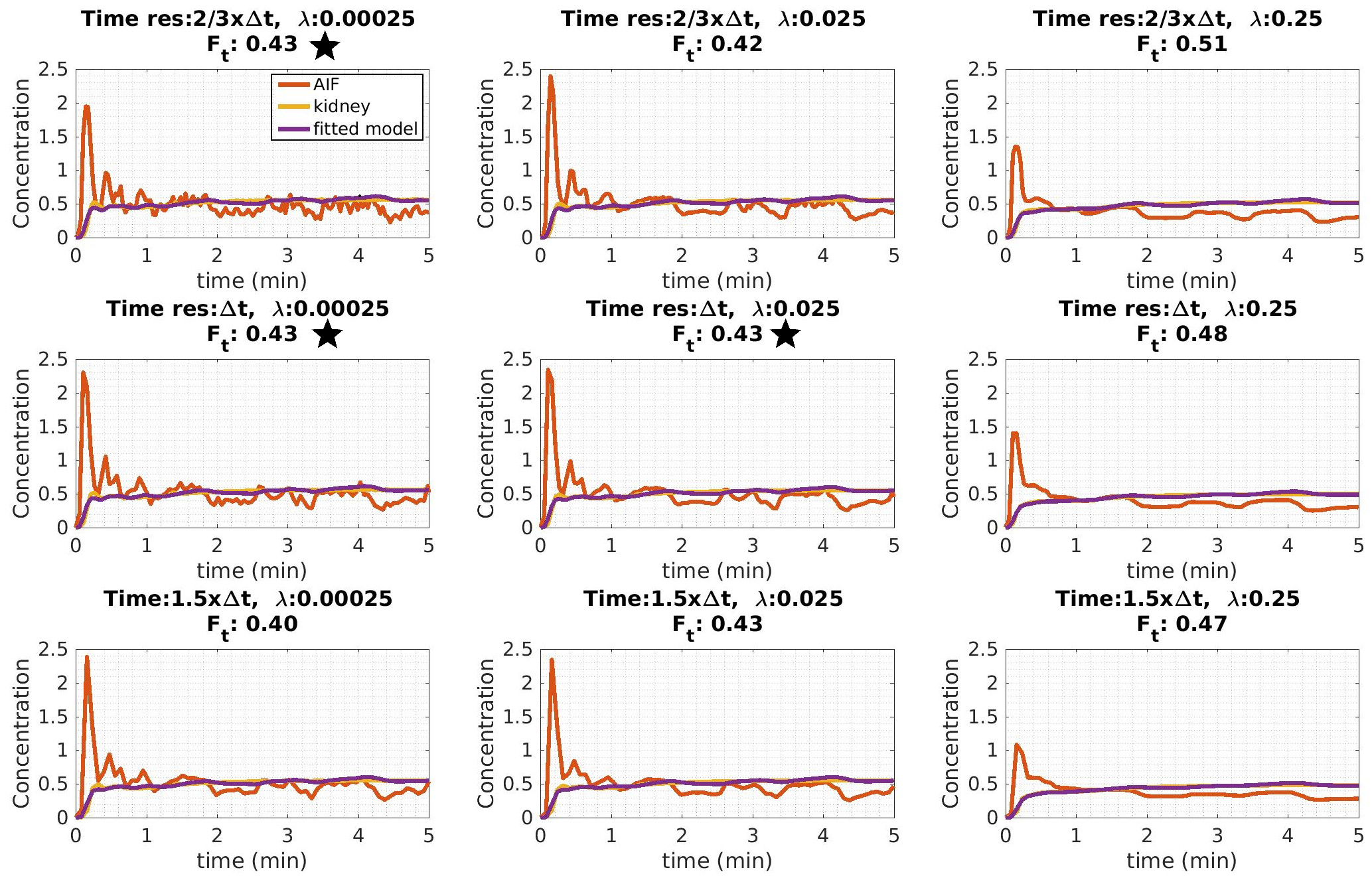
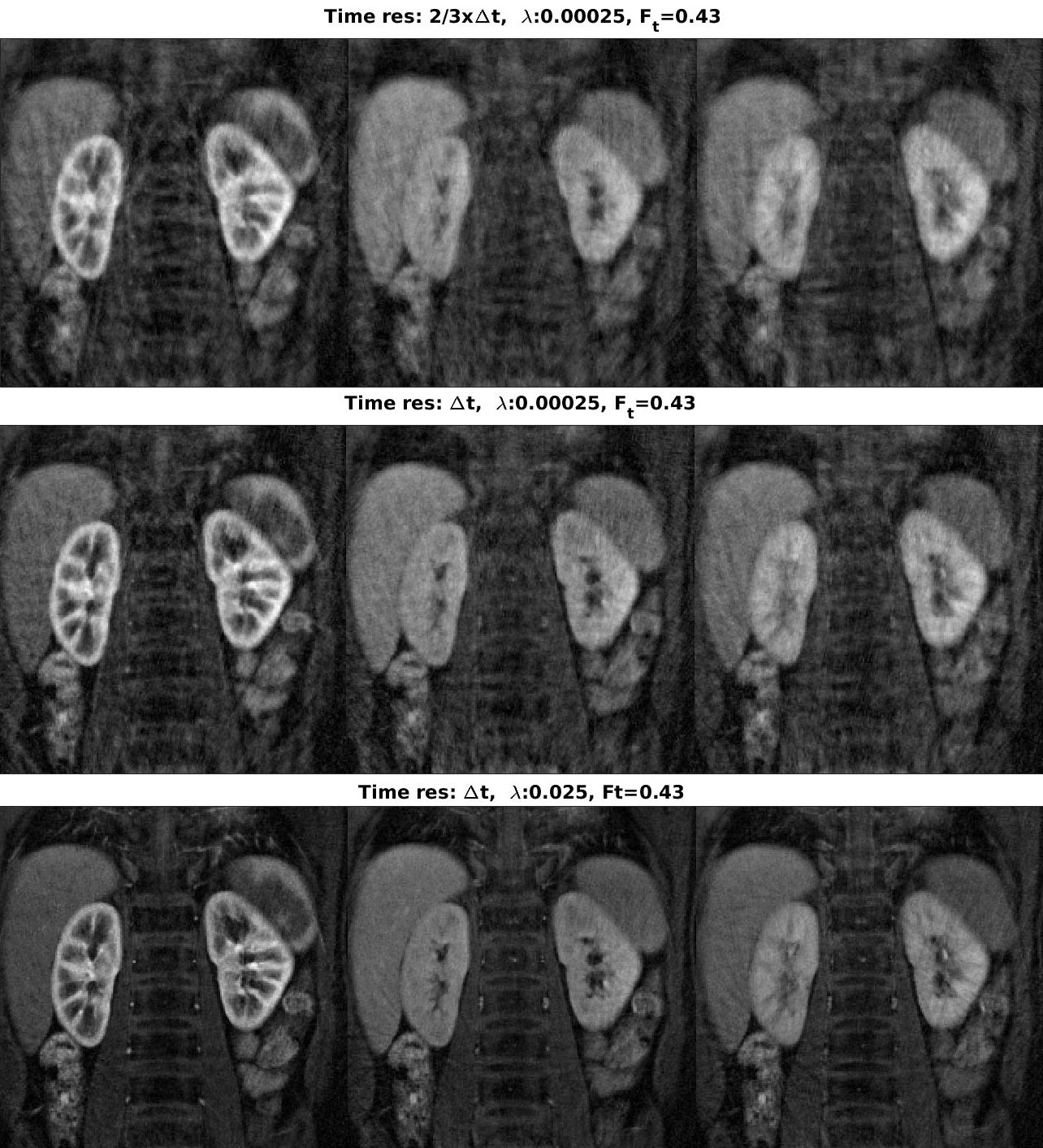
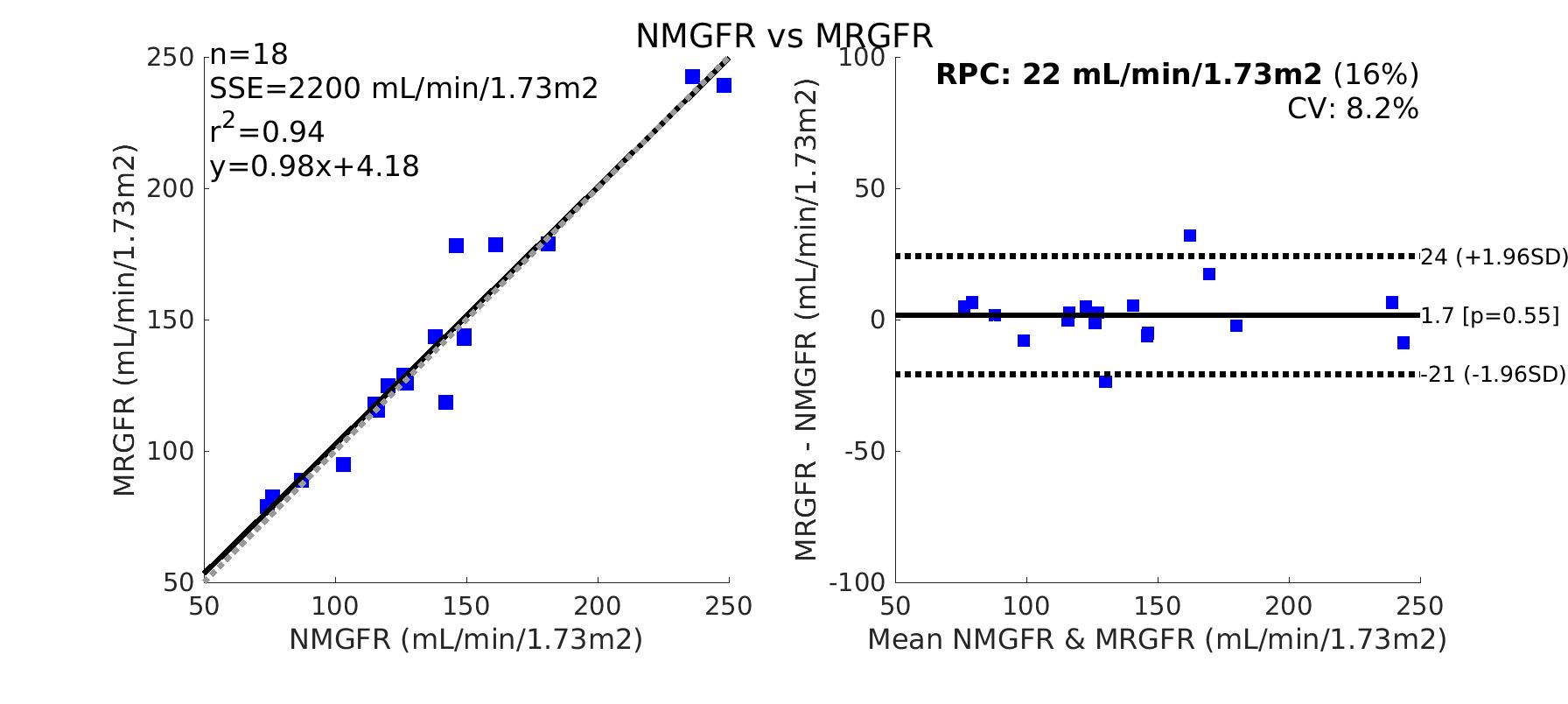
18 children (average age 5.9, 8 female/10 male) were enrolled between July 2017-present. The method was technically feasible in all patients. Figure 1 shows the results of aorta segmentation using densely connected F-CNN4-5 (Tiramisu) for a sample subject. The kidney segmentation results are shown in Figure 2 for the same subject. The algorithm successfully detected kidneys for all subjects with both single and double kidneys. Figure 3 shows the results of our analysis for optimal selection of temporal resolution (Δt) and regularization parameter (λ) of the temporal regularization term of the compressed sensing reconstruction. With increasing λ, the AIF peak was smoothed out, but also when λ was too small and temporal resolution was too high at the same time (1st row and column), the reconstructed images had low quality and were noisy, and the AIF peak was also compromised. Figure 4 compares the quality of the resultant reconstructed images for selected λ and Δt values that resulted in the same Ft. Parameters in row 3 resulted in the best image quality, while achieving an accurate AIF peak. These selected parameters, i.e. a small λ=0.025 and high temporal resolution (Δt=3.3secs) were used when reconstructing images of all subjects. MRI-GFR values computed by the proposed pipeline are compared with NMGFR values in Figure 5. MRI-GFR correlated with NMGFR with r-square value of 0.94. Bland Altman analysis (right panel) indicated a reproducibility coefficient (RPC) of 22 with 95% confidence interval, and coefficient of variation (CV) of 8.2%.Conclusions
The proposed radial VIBE DCE-MRI technique to compute MRI-GFR is a reliable and easy-to-use method of measuring GFR, when using optimized parameters and a fully automated segmentation and parameter estimation pipeline. MRI-GFR values were comparable with NMGFR using plasma clearance of 99mTcDTPA.Acknowledgements
This work was supported by Boston Children’s Hospital Translational Research Program Grant 2018 and Society of Pediatric Radiology Young Investigator Grant 2016 and by NVIDIA Corporation with the donation of the Titan Xp GPU used for this research.References
- Feng L, Grimm R, Block T, et al. Golden-angle radial sparse parallel MRI: Combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med. 2014;72: 707–717.
- Haghighi M, Warfield SK, and Kurugol S. Automatic renal segmentation in DCE-MRI using convolutional neural networks. In Biomedical Imaging (ISBI 2018), 2018 IEEE 15th International Symposium on. p.1534-1537. IEEE. April 2018.
- Sourbron SP, et al. MRI-measurement of perfusion and glomerular filtration in the human kidney with a separable compartment model. Investigative radiology, vol 43(1), 2008, p. 40-48.
- J´egou S, et al.,The One Hundred Layers Tiramisu: Fully Convolutional DenseNets for Semantic Segmentation. Computer Vision and Pattern Recognition Workshops (CVPRW) 2017, pp. 1175-1183.
- Huang G, et al., Densely Connected Convolutional Networks. Computer Vision and Pattern Recognition CVPR 2017, Vol. 1, p. 3.
Figures