0842
High-resolution whole brain ASL perfusion imaging using variably undersampled Cartesian Fast-Spin-Echo and Compressed Sensing reconstruction1Division of MRI research, Radiology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, United States, 2Diagnostic Imaging and Radiology, Children’s National Medical Center, Washington DC, DC, United States
Synopsis
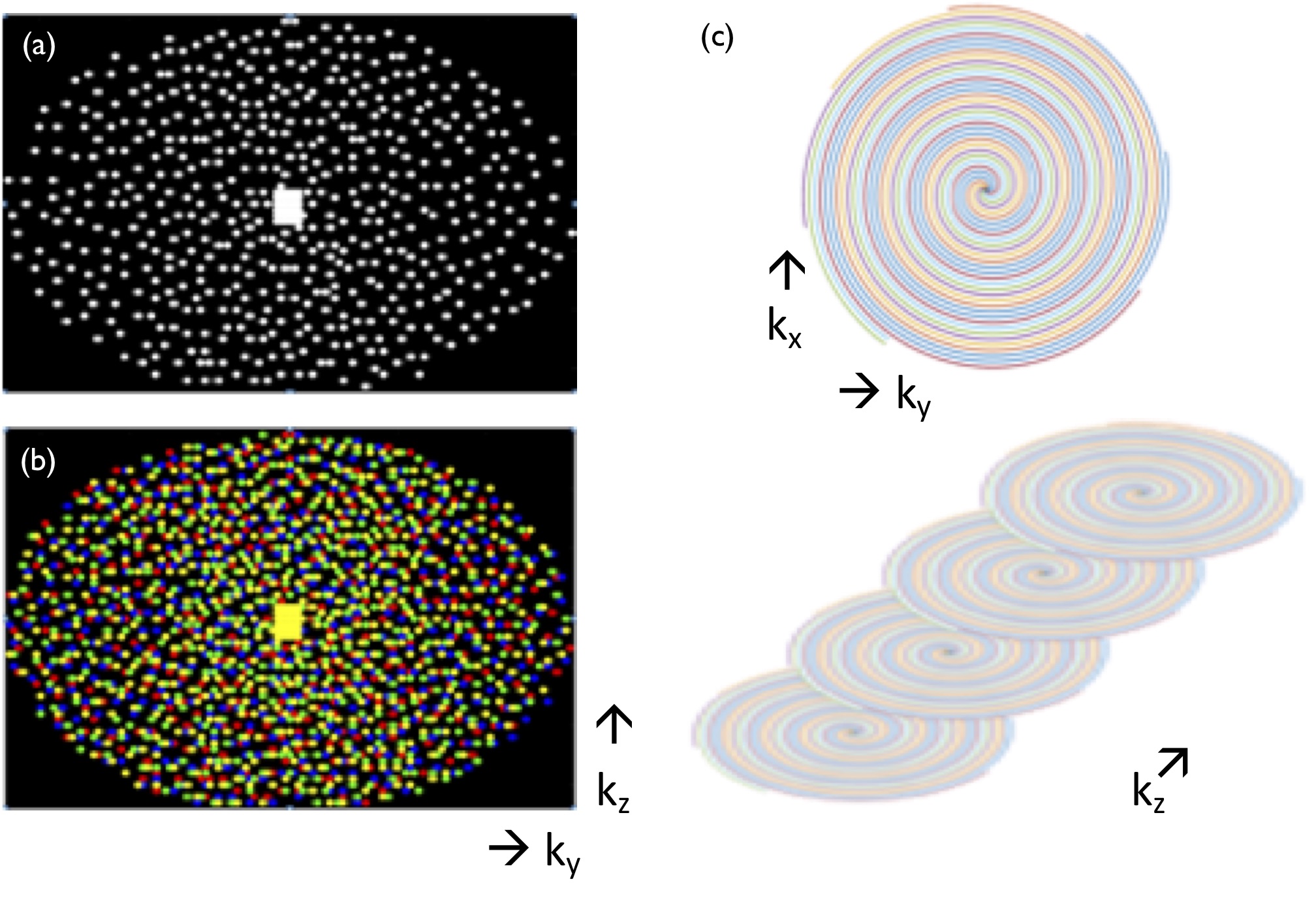
3D whole-brain ASL is typically performed using either Stack-of-Spirals FSE or GRASE. However, those readouts suffer from significant image blurring and off-resonance sensitivity. Hence, Cartesian encoding would be highly desirable because of its robustness and high image quality, but acquisition times remain prohibiting. We therefore report the implementation of an accelerated 3D-FSE sequence using variable-density Poisson-disk undersampling to provide redundant k-space center sampling while varying the outer pseudo-random sampling and Parallel-Imaging Compressed-Sensing reconstruction to provide high quality high-resolution whole brain ASL perfusion images.
Introduction
Though early ASL studies were limited to one or a few slices, continued development has made whole brain perfusion measurement with ASL routinely feasible. As stated by the ASL consensus paper for clinical neuroradiologic applications1, 3D encoding using Stack-of-Spirals Fast-Spin-Echo (SoS-FSE) or Gradient-Spin-Echo (GRASE) readouts is recommended to get whole brain coverage with optimal SNR and compatibility with background suppression. But both SoS-FSE and GRASE are vulnerable to off-resonance, degraded image quality due to through-plane blurring and non-trivial reconstruction for spirals. As a robust workhorse of volumetric imaging, Cartesian 3D-FSE would be a good candidate, but its slowness prevents its use for volumetric ASL. Hence, we report in the current work the implementation of an accelerated 3D-FSE sequence using variable-density Poisson-disk (VD-C-FSE) undersampling and Parallel-Imaging Compressed-Sensing (PI-CS) reconstruction2 to provide high quality high-resolution whole brain ASL perfusion images. We implemented a strategy providing redundant center and variable outer k-space sampling to further enhance CS capabilities.Material and Methods
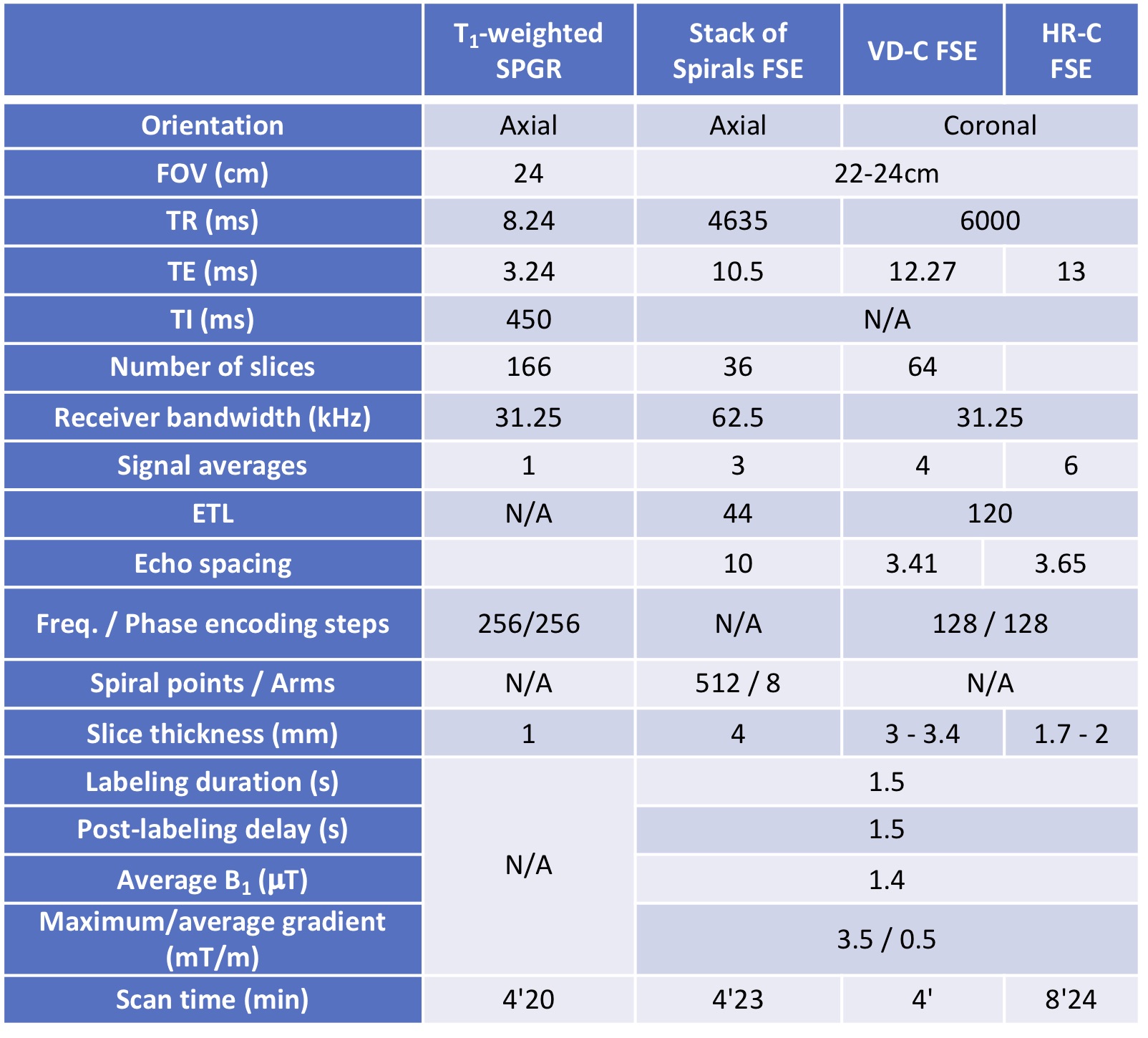
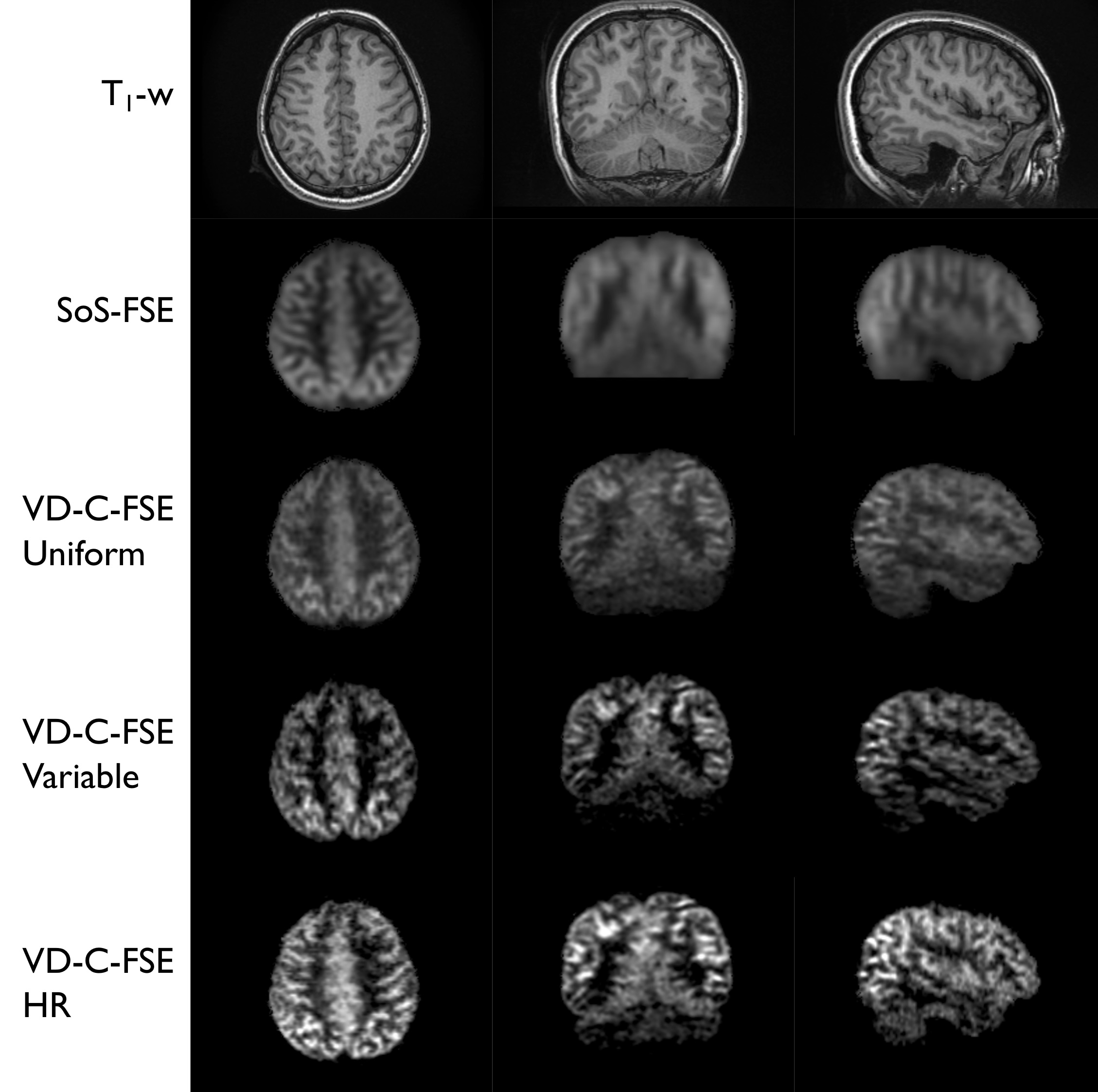
4 healthy volunteers (33±17yo,3F/1M) were scanned at 3T (GE Discovery MR750) with a 32-ch head coil. An axial 3D-T1-w-FSPGR volume was acquired for anatomical reference. All ASL acquisitions used 1.5s pCASL labeling (1.5s PLD, B1_av=1.4$$$\mu$$$T, Gmax/Gav=3.5/0.5mT/m3,4) background-suppression and inferior in-flow saturation. The following ASL sequences were acquired (Fig.1):
- SoS-FSE commercially available (nominal in-plane resolution 3.6x3.6mm2, 440ms echo-train)
- VD-C-FSE with the same undersampling pattern repeated across averages
- VD-U-FSE with a varying pseudo-random undersampling across averages (408ms echo-train)
- HR-C-FSE a high isotropic spatial resolution acquisition (1.7 to 2mm3 isotropic resolution, 432ms echo-train).
All Cartesian-FSE acquisitions use a flip-angle modulation of the refocusing echo-train while the SoS does not. Additionally, a proton-density pre-saturated reference volume was acquired matching resolution for both SoS and C-FSE. All acquisition details are provided in Fig.2.
The SoS-FSE were reconstructed using the standard product online reconstruction pipeline. For the C-FSE acquisitions, raw k-space data were saved for offline reconstruction under MATLAB using the BART toolbox5. After coil-sensitivity estimation using ESPIRiT6 on the M0 volume (calibration region 323, cluster size k=63, $$$\sigma$$$=0.01 and threshold=0.8), a PI-CS reconstruction7 of the volume m was performed with k-t sparsity enforcement of the data y by minimizing the L1-norm of spatial wavelets ($$$\psi$$$) and L1-TV ($$$\lambda$$$1=0.001, $$$\lambda$$$2=0.05) using the ADMM algorithm (max. 100 iterations):
$$$ m(x,y,z,t)=argmin\parallel DFSm(x,y,z,t)-y(x,y,z,t) \parallel_{2}+\lambda_{1}\parallel\psi m(x,y,z)\parallel_{1}+\lambda_{2}\parallel TV m(t)\parallel_{1} $$$(1)
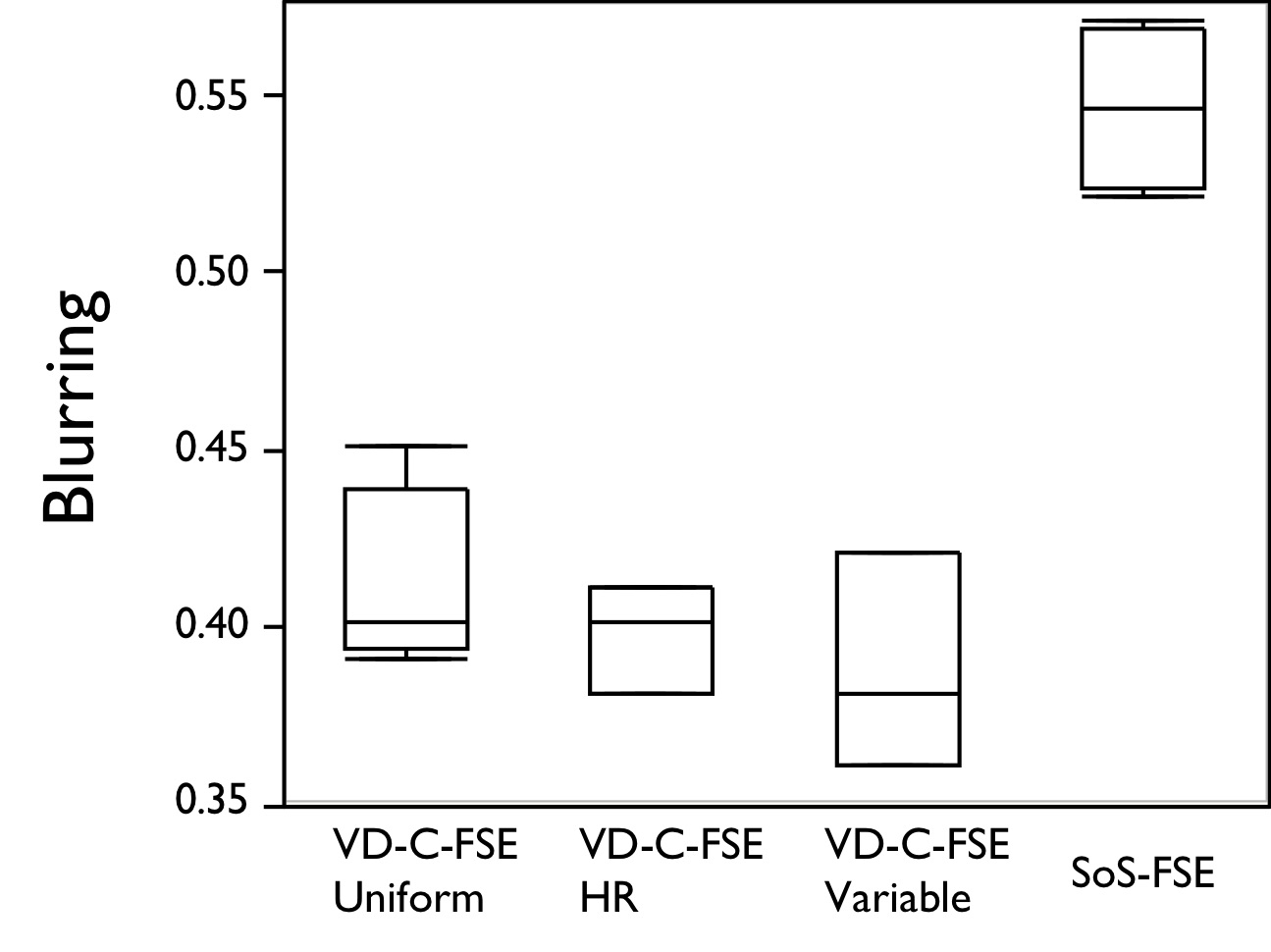
With D a sampling, F Fourier-transform and S ESPIRiT operators. Spatial normalization, segmentation and cortical surface estimation was performed using FreeSurfer on the T1-w volume. Then, all ASL volumes were normalized to a smoothed GM-segmentation (2mm3 Gaussian kernel) of the T1-w volume using FSL (12-DOF affine registration, CC metric), allowing projection of the cortical surfaces on the ASL data. After qualitative assessment, a non-reference blurring metric as used in previous work8,9 was calculated on whole brain perfusion-weighted images for each encoding/reconstruction and compared using a multiple-pairs HSD Tukey-Kramer test.
Results
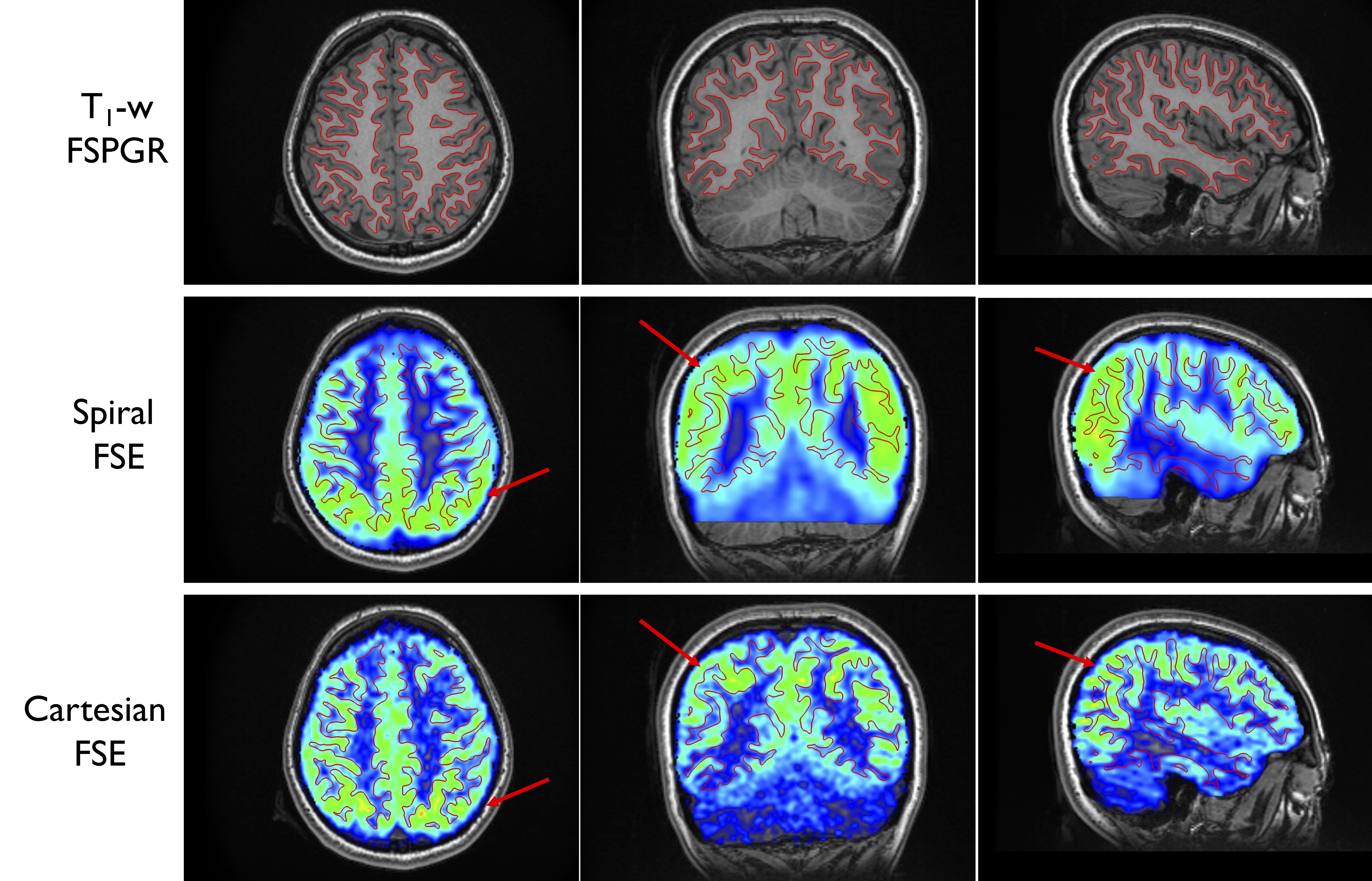
As seen on Fig.3, for similar echo-train duration, all Cartesian-FSE images present less blurring in any orientation, while the SoS-FSE presents higher blurring both in and through-plane that degrades image quality especially in coronal/sagittal reformats, although acquired at close to isotropic nominal resolution partially because of the C-FSE flip-angle modulation. However, the Cartesian data appear to have lower SNR, although no quantitative SNR measure was performed because of the CS reconstruction. Quantitative non-reference blurring supports the qualitative assessment, with a significantly higher blurring with the SoS-FSE readout (p<0.0001, Fig.4). Although a lower mean value is observed for the variable temporal sampling, no significant difference was seen between the different Cartesian-FSE acquisitions, probably because of small sample size. Finally, looking at the projection of the estimated cortical boundary on ASL images (Fig.5) confirms previous qualitative and quantitative observations, especially in the parietal/occipital regions. The high perfusion from cortical gray matter appears to follow more precisely the actual cortex as defined by the surfaces from the T1-w volume.Discussion and Conclusions
While Stack-of-Spiral-FSE readouts provide faster k-space sampling without requiring further acceleration, they suffer from loss of image quality mostly due to increased blurring and higher off-resonance sensitivity compared to Cartesian encoding. However, recent strategies combining tailored echo-train modulation and k-space filtering8 showed reduced blurring and should warrant further investigations. Although the still slower acquisition time of Cartesian encoding wouldn’t be suitable for functional fluctuation studies (e.g. resting-state) using ASL10, it does represent a promising and valuable alternative to GRASE (although not explored in the current study) or SoS-FSE for high-resolution, high-quality whole-brain average perfusion measurement using ASL. Furthermore, additional dimensions could be considered for undersampling to provide for example multi-PLD based Arterial-Transit-Time and CBF quantification using an undersampled Hadamard encoding scheme11.Acknowledgements
No acknowledgement found.References
1. Alsop, D. C. et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn. Reson. Med. 73, 102–116 (2015).
2. Lustig, M., Donoho, D. & Pauly, J. M. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn. Reson. Med. 58, 1182–1195 (2007).
3. Dai, W., Garcia, D., de Bazelaire, C. & Alsop, D. C. Continuous flow-driven inversion for arterial spin labeling using pulsed radio frequency and gradient fields. Magn. Reson. Med. 60, 1488–1497 (2008).
4. Zhao, L., Vidorreta, M., Soman, S., Detre, J. A. & Alsop, D. C. Improving the robustness of pseudo-continuous arterial spin labeling to off-resonance and pulsatile flow velocity. Magn. Reson. Med. (2016). doi:10.1002/mrm.26513
5. Uecker, M. et al. Berkeley Advanced Reconstruction Toolbox. in Proc. Intl. Soc. Mag. Reson. Med 2486 (2015).
6. Uecker, M. et al. ESPIRiT—an eigenvalue approach to autocalibrating parallel MRI: Where SENSE meets GRAPPA. Magn. Reson. Med. 71, 990–1001 (2014).
7. Cheng, J. Y. et al. Free-breathing pediatric MRI with nonrigid motion correction and acceleration. J. Magn. Reson. Imaging 42, 407–420 (2015).
8. Zhao, L., Chang, C.-D. & Alsop, D. C. Controlling T2 blurring in 3D RARE arterial spin labeling acquisition through optimal combination of variable flip angles and k-space filtering. Magn. Reson. Med. 80, 1391–1401 (2018).
9. Crete, F., Dolmiere, T., Ladret, P. & Nicolas, M. The blur effect: perception and estimation with a new no-reference perceptual blur metric. in Human Vision and Electronic Imaging XII 6492, 64920I (International Society for Optics and Photonics, 2007).
10. Dai, W., Varma, G., Scheidegger, R. & Alsop, D. C. Quantifying fluctuations of resting state networks using arterial spin labeling perfusion MRI. J. Cereb. Blood Flow Metab. 36, 463–473 (2016).
11. Dai, W., Shankaranarayanan, A. & Alsop, D. C. Volumetric measurement of perfusion and arterial transit delay using hadamard encoded continuous arterial spin labeling. Magn. Reson. Med. 69, 1014–1022 (2013).
Figures