0826
Choroid plexus perfusion MRI indicates cerebrospinal fluid production changes after surgically-manipulated vascular tone: implications for glymphatic flow1Radiology and Radiological Sciences, Vanderbilt University School of Medicine, Nashville, TN, United States, 2Neurology, Vanderbilt University School of Medicine, Nashville, TN, United States, 3Psychiatry, Vanderbilt University School of Medicine, Nashville, TN, United States
Synopsis
The objective of this study was to determine if a feedback circuit between CSF production and arterial health may exist in the human brain. Sequential measurements of CSF volume were obtained, as well as cortical and choroid plexus function measured from pseudo-continuous arterial spin labeling (pCASL) before and after clinically-indicated indirect surgical revascularization. Regression analyses were used to evaluate dependence of study parameters on time. Following surgically-induced angiogenesis, fronto-parietal perfusion increased, which paralleled a reduction in choroid plexus perfusion. This could reflect a homeostatic mechanism where improved perivascular flow and more robust waste clearance prompts decreased choroid plexus CSF production.
Introduction
Recent studies have provided evidence in support of a CNS lymphatic drainage system in vertebrate animals, in which communication exists between brain parenchyma, perivascular and interstitial spaces, and CSF.1 This glymphatic system is believed to operate to clear interstitial solutes along perivascular spaces and in coordination with meningeal lymphatic vessels to clear CSF and metabolic waste products toward draining lymph nodes. However, interrogating this system in vivo in humans has been difficult owing to a general inability to measure CSF production activity in the choroid plexus and perivascular flow with sufficient sensitivity. Here we apply quantitative hemodynamic and anatomical imaging to evaluate the effect of angiogenesis-inducing interventions, which increase perivascular flow, on choroid plexus function. The hypothesis to be investigated is that by improving perivascular flow via duro-arterio-synangiosis, less CSF production will be required for waste clearance, and choroid plexus activity will reduce if perivascular arterial health and CSF flow dynamics are related.Methods
Study procedure. A cross-sectional study was performed in which consenting patients (n=23) presenting with symptoms of moyamoya received multi-modal MRI (Philips, Best, The Netherlands) and catheter angiography (Fig. 1) before and after surgical revascularization (interval duration=275±28 days; Fig. 1). For comparison, patients (n=10) without any interval intervention were scanned twice with a similar interval scan duration (interval duration=360±75 days). MRI. Standard anatomical imaging (T1-weighted MPRAGE, T2-weighted FLAIR, DWI) and a novel pseudo-continuous arterial spin labeling (pCASL)2 approach covering the choroid plexus and cortical revascularization site were performed at both time points. Analysis. T1-weighted scans were used to calculate total intracranial and non-fluid tissue volume using FSL-FAST.3 For CBF determination, pCASL data were calculated4 in the choroid plexus located within the inferior horn of the lateral ventricles, as well as in the fronto-parietal parenchyma at the location of the resection site. Hypothesis testing. A Wilcoxon signed-rank test was applied to the total intracranial CSF normalized by intracranial volume for all participants with interval surgeries before vs. after the surgical revascularization, as well as to participants without interval surgeries. A logistic regression analysis was performed across all 33 participants using the patient category (interval surgery vs. no interval surgery) as the dependent variable and fronto-parietal CBF change, choroid plexus CBF change, and age as the independent variables. Two-sided p<0.05 was required in all cases for significance.Results
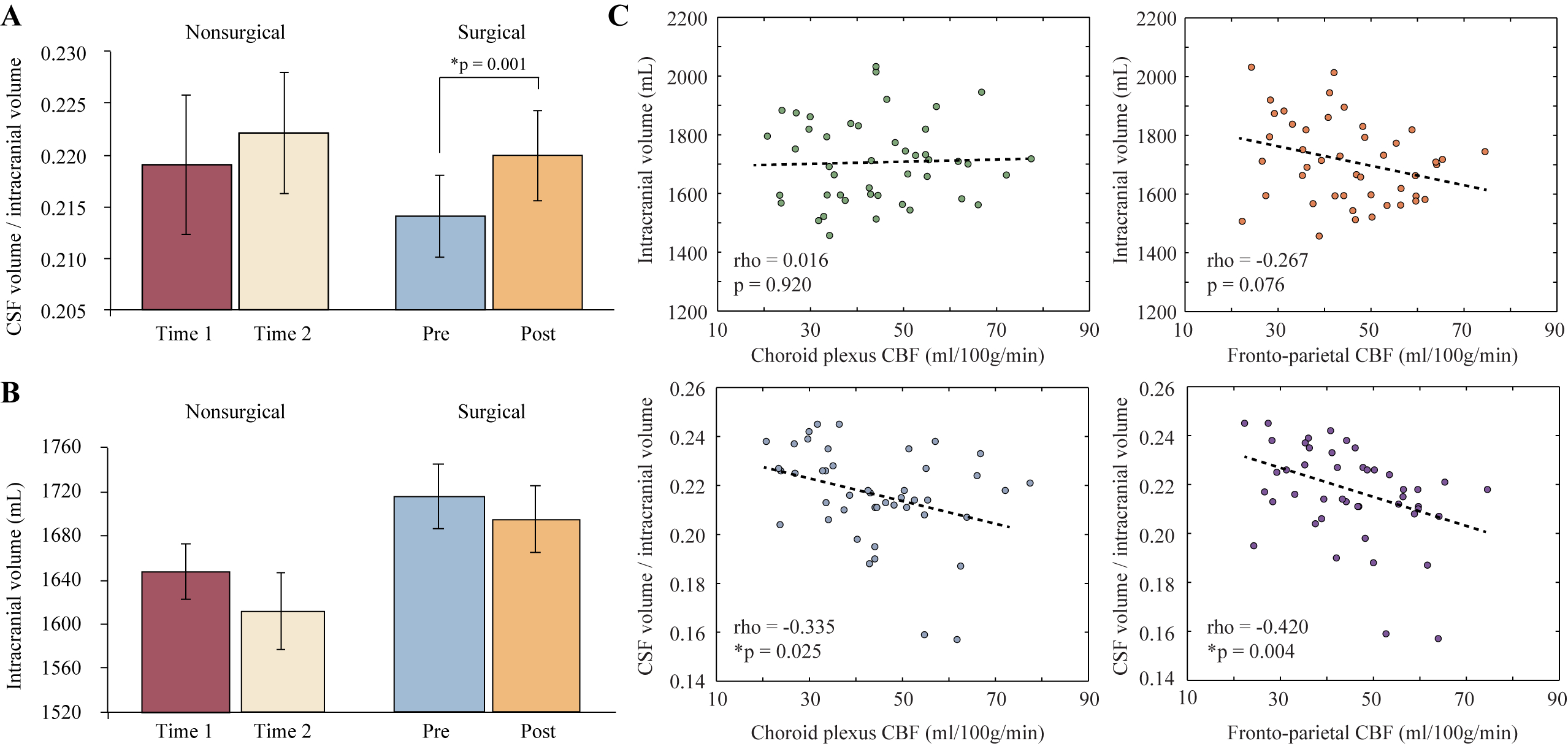
In patients without interval surgeries, the normalized intracranial CSF volume (0.219±0.089) and total intracranial volume (1648±38.2 mL) at the first time point were statistically unchanged from the normalized intracranial CSF volume (0.221±0.056) and total intracranial volume (1611±42.8 mL) at the second time point. In patients with interval surgeries, the total intracranial volume did not change significantly (p=0.16) from pre-surgery (1717±29 mL) to post-surgery (1696±30 mL), but the normalized intracranial CSF volume increased slightly to 0.220±0.004 (post-surgery) from 0.214±0.004 (pre-surgery) (Fig. 2).
On regression analysis, the fronto-parietal CBF reduced in patients without interval surgeries by 16.1±13.1% and the choroid plexus CBF increased by 8.6±10.4%. The opposite trend was observed in the patients with interval surgeries, in which the fronto-parietal CBF on the side of revascularization increased by 12.1±8.3% whereas the choroid plexus CBF reduced by 10.5±17.1% (Table 1; Fig. 3). These changes were all significant at a two-sided significance level of p<0.05.
Discussion
We performed consecutive measurements of choroid plexus perfusion, CSF volume, and fronto-parietal perfusion in patients with intracranial stenosis before and after surgical revascularization. Findings suggest that choroid plexus activity, which provides a surrogate marker of CSF production, is highest when arterial flow is lowest. Following revascularization and angiographically-confirmed improvement in arterial perivascular flow secondary to increased arterial density, choroid plexus activity reduces. As arterial health has been proposed to be central to CSF flow, this suggests the possibility that a feedback loop may be present that allows for upregulation of choroid plexus CSF production in the setting of poor perivascular arterial flow. Importantly, these data also suggest that emerging quantitative MRI methods should have relevance for interrogating function of the recently-proposed glymphatic pathway.Conclusion
Following surgically-induced angiogenesis, fronto-parietal perfusion increased as expected and this paralleled a reduction in choroid plexus perfusion, consistent with reduced CSF production. This could reflect a homeostatic mechanism where improved perivascular flow and more robust waste clearance prompts decreased choroid plexus CSF production.Acknowledgements
No acknowledgement found.References
1.Iliff JJ, Wang M, Liao Y, et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid β. Sci Transl Med. 2012;4(147):147ra111.
2. Dai W, Garcia D, de Bazelaire C, Alsop DC. Continuous flow-driven inversion for arterial spin labeling using pulsed radio frequency and gradient fields. Magnetic resonance in medicine 2008; 60(6): 1488-97.
3. Zhang Y, Brady M, Smith S. Segmentation of brain MR images through a hidden Markov random field model and the expectation-maximization algorithm. IEEE transactions on medical imaging 2001; 20(1): 45-57.
4. Alsop DC, Detre JA, Golay X, Gunther M, Hendrikse J, Hernandez-Garcia L, et al.Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magnetic resonance in medicine 2015; 73(1): 102-16.
Figures