0824
MEMRI Can Quantify Myocardial Infarct Size Earlier Than LGE-MRINur Hayati Jasmin1,2, May Zaw Thin1, Valerie Taylor1, Christopher S Pope1, Mark F Lythgoe1, Sean Davidson3, and Daniel J Stuckey1
1Division of Medicine, Centre for Advanced Biomedical Imaging, University College London, London, United Kingdom, 2School of Medical Imaging, Universiti Sultan Zainal Abidin, Terengganu Darul Iman, Malaysia, 3Hatter Cardiovascular Institute, University College London, London, United Kingdom
Synopsis
Late gadolinium enhanced MRI (LGE-MRI) is an established method for quantification of infarct size after myocardial infarction but is non-specific and reflects the increased membrane rupture and extracellular volume (ECV) that occurs several hours after myocardial infarction. Manganese (Mn2+) is an efficient intracellular MR contrast agent, which acts as an analogue of Calcium (Ca2+) and can provide information on cell viability. The present study shows that manganese-enhanced MRI (MEMRI) can quantify the final infarct size earlier than LGE-MRI.
Introduction
Cardiomyocytes in the area of perfusion defect will die if blood flow is not restored after myocardial infarction1. An in vivo tool able to measure final infarct size at an early time point after coronary occlusion would be beneficial. Late gadolinium enhanced MRI (LGE-MRI) can accurately delineate infarct size after myocardial infarction (MI) owing to non-specific accumulation of gadolinium contrast agent within the increased extracellular volume (ECV) on the damaged tissue2. However, in the first hours after injury these changes in ECV may not have occurred and infarct quantification could be inaccurate. Manganese-enhanced MRI can enhance viable myocardium as contracting myocytes accumulate Mn ions via voltage gated calcium channels3. This active process ceases under ischemia. Hence, we hypothesized that MEMRI would be able to quantify the final infarct size earlier than LGE-MRI and tested this by applying both methods to mice at 1 and 24 hours after myocardial infarction.Materials and Methods
All procedures complied with The UK Home Office and local animal care and welfare committees. 7 adult male C57BL/6 mice were included after left coronary artery (LAD) ligation. MEMRI was performed in 4 mice and LGE-MRI was performed in 3 mice at 1 hour after LAD ligation. All animals then underwent both MEMRI and LGE-MRI at 24 hours post MI with a contrast washout period of at least 5 hours between scans. MEMRI was acquired at 40 to 60 minutes after intraperitoneal (IP) injections of 0.1mmol/kg MnCl2 while LGE-MRI images was acquired at 20 to 40 minutes after IP injections of 0.5mmol/kg gadolinium-diethylenetriamine penta acetic acid-bismethylamide (Gd-DTPA-DMA). Imaging was performed using a 9.4T MRI Agilent system and a multi-slice inversion recovery sequence as described4 in the short-axis orientation to cover the whole left ventricle (LV) (TE/TR = 3.04/1.11ms, TI = ~600ms for MEMRI and ~350ms for LGE-MRI, excitation pulse = 90⁰, slice thickness = 1.0mm, FOV = 25.6mm2, and matrix size = 1282). CINE movies were also acquired for cardiac function measurement using a gated gradient echo sequence. Data were analysed using ImageJ software (National Institutes of Health) and Segment (Medviso, Sweden).Results
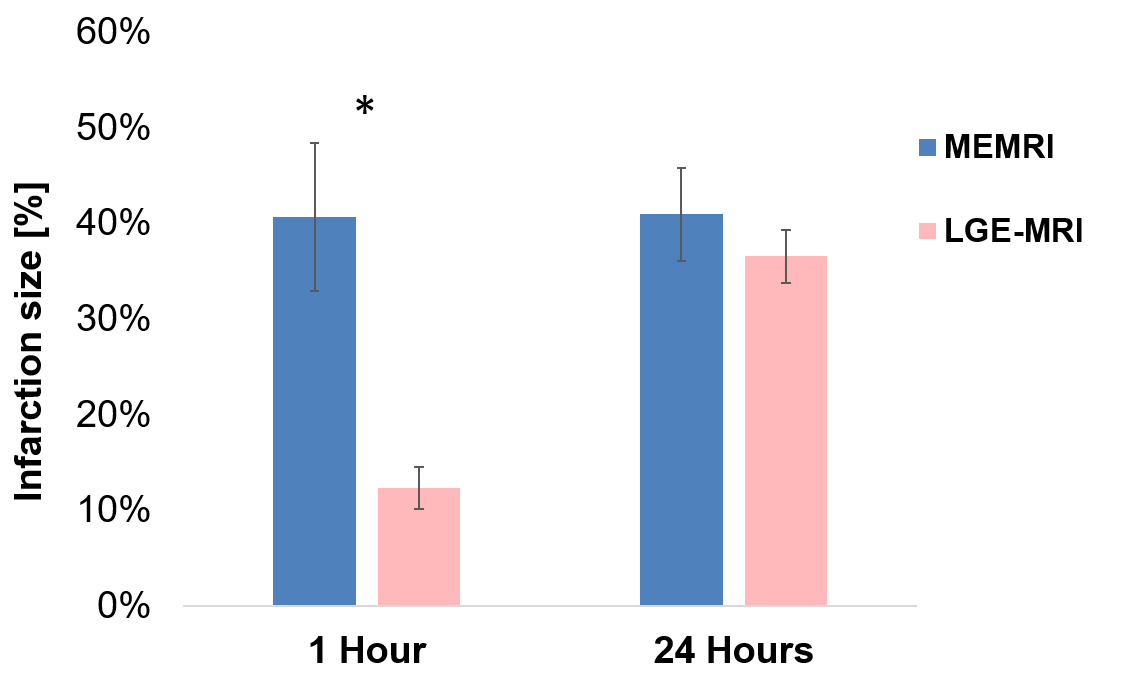
Physiological results show reduction in cardiac function as soon as 1 hour following permanent infarction and no further changes in EDV, ESV and EF at 24 hours post MI (Table 1). At 1 hour post MI, Mn2+ enhancement is seen in viable myocardium from MEMRI allowing early delineation of the estimated final infarct region whereas only subtle enhancement seen in LGE-MRI image (Figure 1). Figure 2 shows a significant difference in the estimated final infarct size from MEMRI (41 ± 8%) and LGE-MRI (12 ± 2%) (p = 0.03) at 1 hour post MI. At 24 hours post MI, there is no significant different in the infarct size from MEMRI (41 ± 5%) compared to LGE-MRI (37 ± 3%). Figure 3 shows a direct comparison of MEMRI and LGE-MRI acquired in the same animal at 22 and 27 hours after MRI, respectively. Matching histological section shows pale region in triphenyltetrazolium chloride (TTC) staining, indicating infarcted tissue (Figure 3).Discussion
MEMRI provides an accurate earlier quantification of the final infarct size, as compared to LGE-MRI. Acutely after ischemic injury Mn2+ uptake in viable myocytes occurs while no uptake is seen in infarct region where myocytes function has ceased. This allows the infarct area to be distinguished at early time point after myocardial infarction. Further, our results suggest that LGE-MRI underestimates infarct size during the first hours after MI, as at this time point only minimal membrane rupture will have occurred and Gadolinium will not have accumulated.Conclusion
The present study shows that manganese-enhanced MRI can quantify final infarct size earlier than LGE-MRI. This provides a sensitive approach which could be used as early measures of cell death and myocardial viability to assess the efficacy of new drugs which target acute MIAcknowledgements
The author acknowledge the following financial support: Nur Hayati Jasmin is funded by King's Scholarship of Malaysia; DJ Stuckey is funded by British Heart Foundation.References
- K. Reimer, J. E. Lowe, M. M. Rasmussen, and R. B. Jennings. (1977). The wavefront phenomenon of ischemic cell death. 1. Myocardial infarct size vs duration of coronary occlusion in dogs. Circulation, 56.
- Doltra, A., Amundsen, B. H., Gebker, R., Fleck, E., & Kelle, S. (2013). Emerging concepts for myocardial late gadolinium enhancement MRI. Current Cardiology Reviews, 9(3).
- Waghorn, B., Schumacher, A., Liu, J., Jacobs, S., Baba, A., Matsuda, T, Hu, T. C.-C. (2011). Indirectly probing Ca(2+) handling alterations following myocardial infarction in a murine model using T1-mapping manganese-enhanced magnetic resonance imaging. Magnetic Resonance in Medicine, 65(1).
- Price, A. N., Cheung, K. K., Lim, S. Y., Yellon, D. M., Hausenloy, D. J., & Lythgoe, M. F. (2011). Rapid assessment of myocardial infarct size in rodents using multi-slice inversion recovery late gadolinium enhancement CMR at 9.4T. Journal of Cardiovascular Magnetic Resonance, 13(1), 44.
Figures

Table
1:
Physiological parameters at 1 and 24 hour after LAD ligation.

Figure 1: Manganese-enhanced MRI
(MEMRI) or Late gadolinium enhancement (LGE) acquired in the same mouse at 1
hour and 24 hours after myocardial infarction. At 1 hour post MI, uptake of
manganese in the viable myocardium allows the estimated final infarct area to be distinguished,
but only subtle enhancement was seen in LGE-MRI. At 24 hours post MI the final infarct region appears as hypoenhancement in the MEMRI image and hyperenhancement in LGE-MRI image.
Figure
2: Result shows a
significant different in the estimated final infarct size (mean ± standard error) from MEMRI (n=4) and LGE-MRI (n=3) at 1
hour post MI. At 24 hours post MI, there is no significant different in the final infarct size from MEMRI (n=7) compared to LGE-MRI (n=7). *Significant
difference (Unpaired Student’s t- test).

Figure 3: Direct
comparison of MEMRI and LGE-MRI acquired in the same animal at 22 and 27 hours
after MI respectively. Arrowhead shows hypoenhancement of
the infarct in the MEMRI image corresponds with hyperenhancement of the infarct in LGE-MRI image. In vivo data corresponded with TTC
histological staining for infarct.