0808
Cardiac motion resolved Magnetic Resonance Fingerprinting with joint reconstruction: jMORE-MRF1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Philips Healthcare, Guilford, United Kingdom, 3Philips Research Europe, Hamburg, Germany
Synopsis
ECG-triggered cardiac Magnetic Resonance Fingerprinting (cMRF) has been proposed to provide simultaneous myocardial T1 and T2 mapping from a single scan. A “free-running” motion-resolved cardiac MRF (MORE-MRF) approach has been recently introduced to provide T1 and T2 myocardial characterization over the entire cardiac cycle. Here we propose to improve MORE-MRF by exploiting redundancy between the different cardiac phases within a novel motion resolved multi-contrast reconstruction framework. The feasibility of this joint MORE-MRF approach (jMORE-MRF) was evaluated in phantom and healthy subjects and compared against conventional T1 and T2 mapping techniques.
Introduction
Cardiac MRI is currently the gold standard for the assessment of left ventricular volumes and function. Quantitative myocardial T1 and T2 mapping is an emerging technique that enables assessment of diffuse fibrosis (T1), edema and inflammation (T2)1. In current clinical practice, these images are acquired sequentially under several breath-holds, resulting in long scan times and potentially misaligned images and motion corrupted parametric maps. ECG-triggered cardiac MR fingerprinting (MRF)2–4 has been proposed to simultaneously measure T1 and T2 maps in a single scan at the diastolic cardiac phase. A “free-running” motion-resolved cardiac MRF (MORE-MRF)5 approach has been recently introduced to provide T1 and T2 myocardial characterization over the entire cardiac cycle, thus enabling simultaneous assessment of cardiac tissue viability and function in a single breath-hold scan. However, MORE-MRF is limited to a reduced number of cardiac phases. Here we propose to improve MORE-MRF reconstruction by exploiting redundancy between the different cardiac phases within a novel motion resolved multi-contrast reconstruction framework. The feasibility of this joint MORE-MRF approach (jMORE-MRF) was evaluated in phantom and five healthy subjects and compared against conventional T1 and T2 mapping techniques.Methods
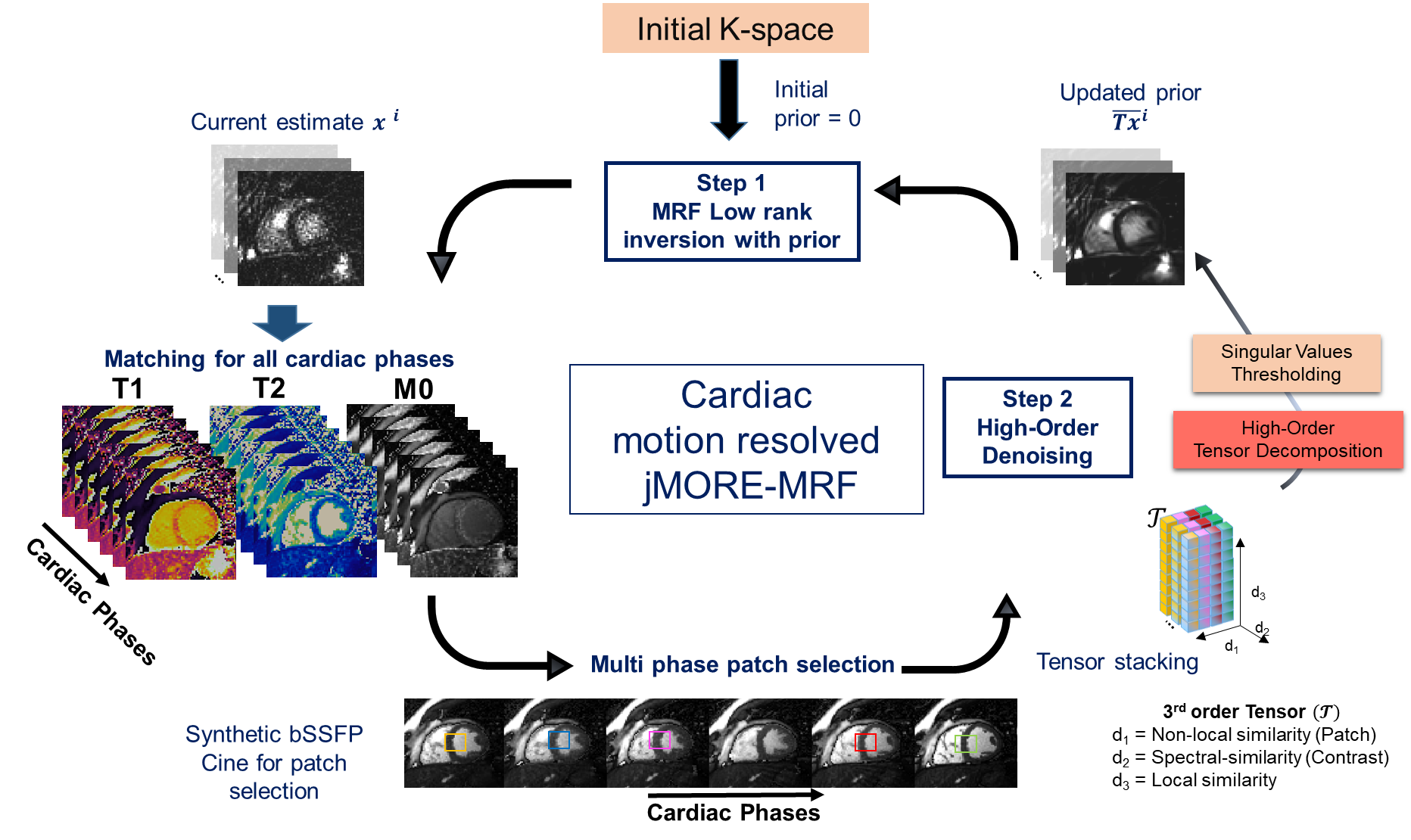
MORE-MRF consists of a continuous bSSFP MRF acquisition with inversion (IR) pulses followed by a variable flip angle pattern5,6 that is repeated every 2.95s. Acquisition is performed with a tiny golden angle (~23o) radial trajectory7. The reconstruction process uses ECG-based retrospective soft-gating and a novel multi contrast patch based undersampled reconstruction (HD-PROST8,9). HD-PROST for MORE-MRF alternates the optimization of 2 steps: 1) low-rank inversion(LRI)10 regularised with denoised images from step 2 as prior, and 2) a higher-order tensor-based denoising that assumes low rankness along 3 dimensions: locally (within a patch)11,12, non-locally (between similar patches) and along different contrasts. Singular images, resulting from the temporal compression (based on the dictionary) of the time-points images, are reconstructed with this approach. In this study, we extend HD-PROST to exploit low rankness also in the cardiac motion dimension by searching for similar patches in all cardiac phases simultaneously, thus providing implicit motion compensation of multi contrast data and joint reconstruction of multiple cardiac phases (Fig.1). A matching step and the generation of a synthetic cine are performed between steps 1) and 2) to obtain same contrast reference images for patch selection throughout the cardiac phases.Experiments
2D free-running cardiac MRF acquisitions were performed on a standardised phantom13 and five healthy subjects using a 1.5T MR scanner (Ingenia, Philips Healthcare) using anterior and posterior coils (28-channels). Acquisition parameters included: TR/TE=4/1.99ms, 7300 time-points, one radial spoke per time-point, 2x2mm2 resolution, FOV=288x288mm2, 10 mm slice thickness, 10 repetitions of IR and flip angle train, 29.5s breath-hold. Eight and sixteen cardiac phases were reconstructed with MORE-MRF (independent reconstruction of each cardiac phase) and jMORE-MRF (joint reconstruction). Reconstruction parameters were set empirically and equally for both methods. For comparison purposes, 2D T1-MOLLI14, T1-SASHA15 and T2-GRASE16 maps were acquired with matching acquisition parameters.Results
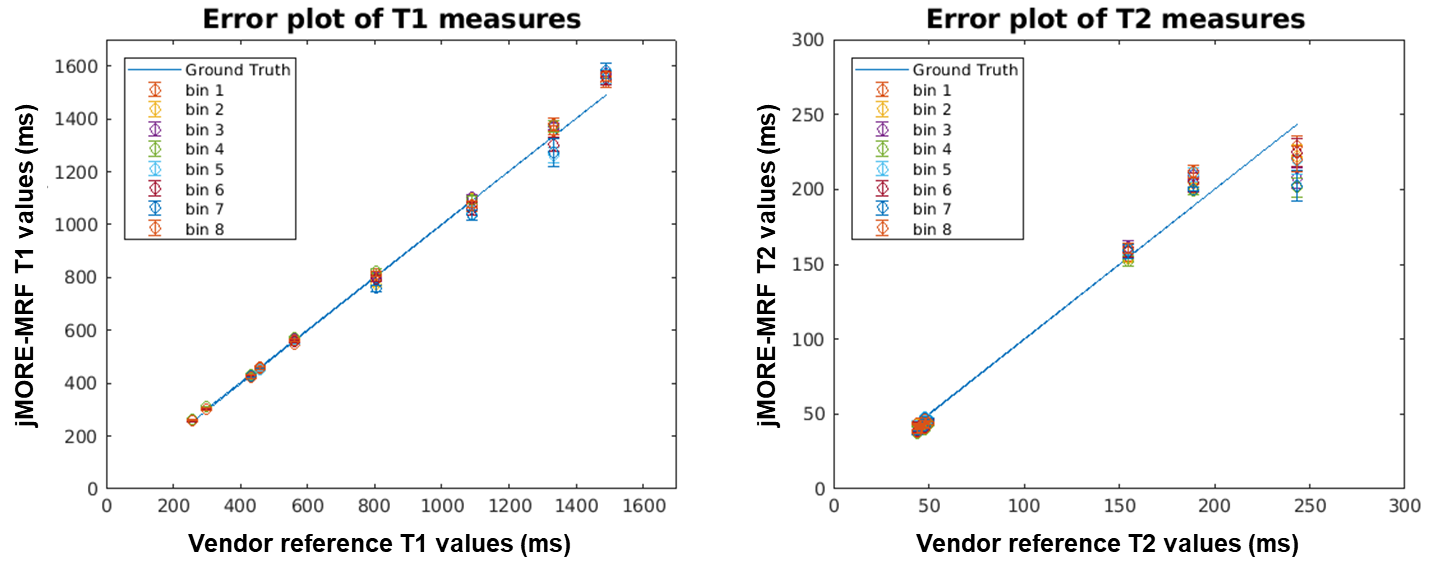
T1
and T2 phantom measurements for 8 phases reconstructed with
jMORE-MRF are shown in Fig.2, demonstrating good agreement with the reference
values provided by the vendor and consistency across different phases. MORE-MRF
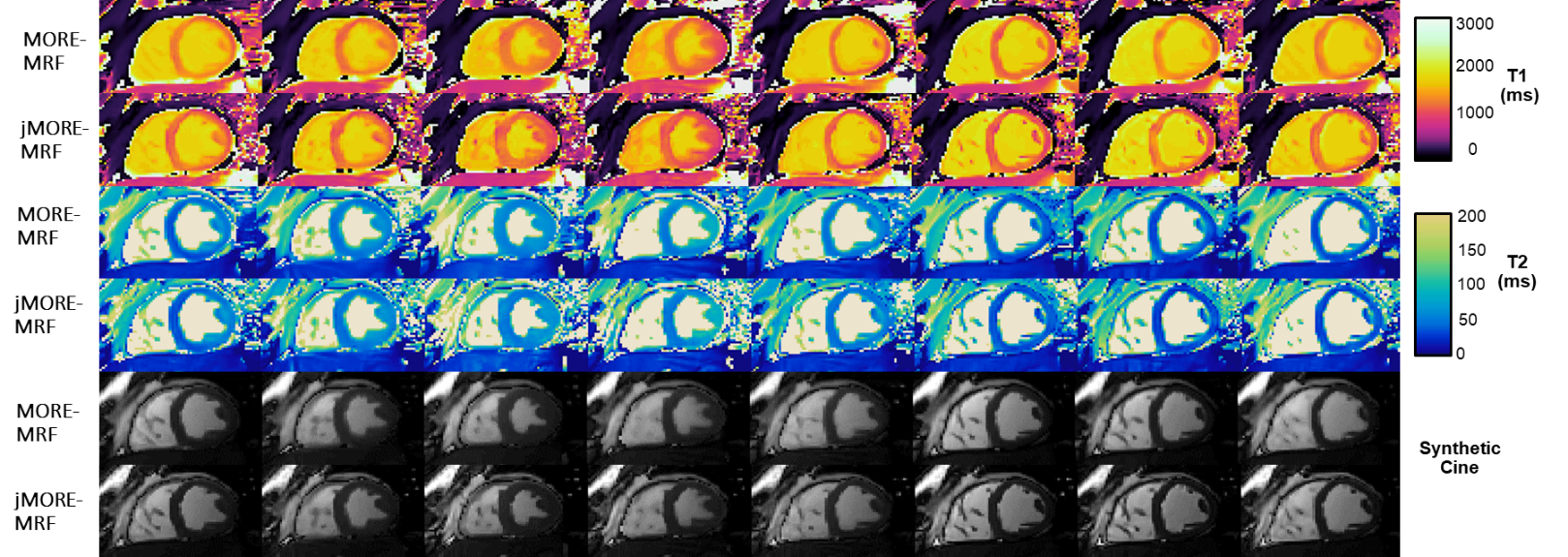
and jMORE-MRF reconstructions for 8 cardiac phases are compared in Fig.3 for a
representative healthy subject. T1, T2 parametric maps and
a synthetic bSSFP cine are included in Fig.3. Exploiting redundancy in the
cardiac dimension allows for improved reconstruction of the time-point images with
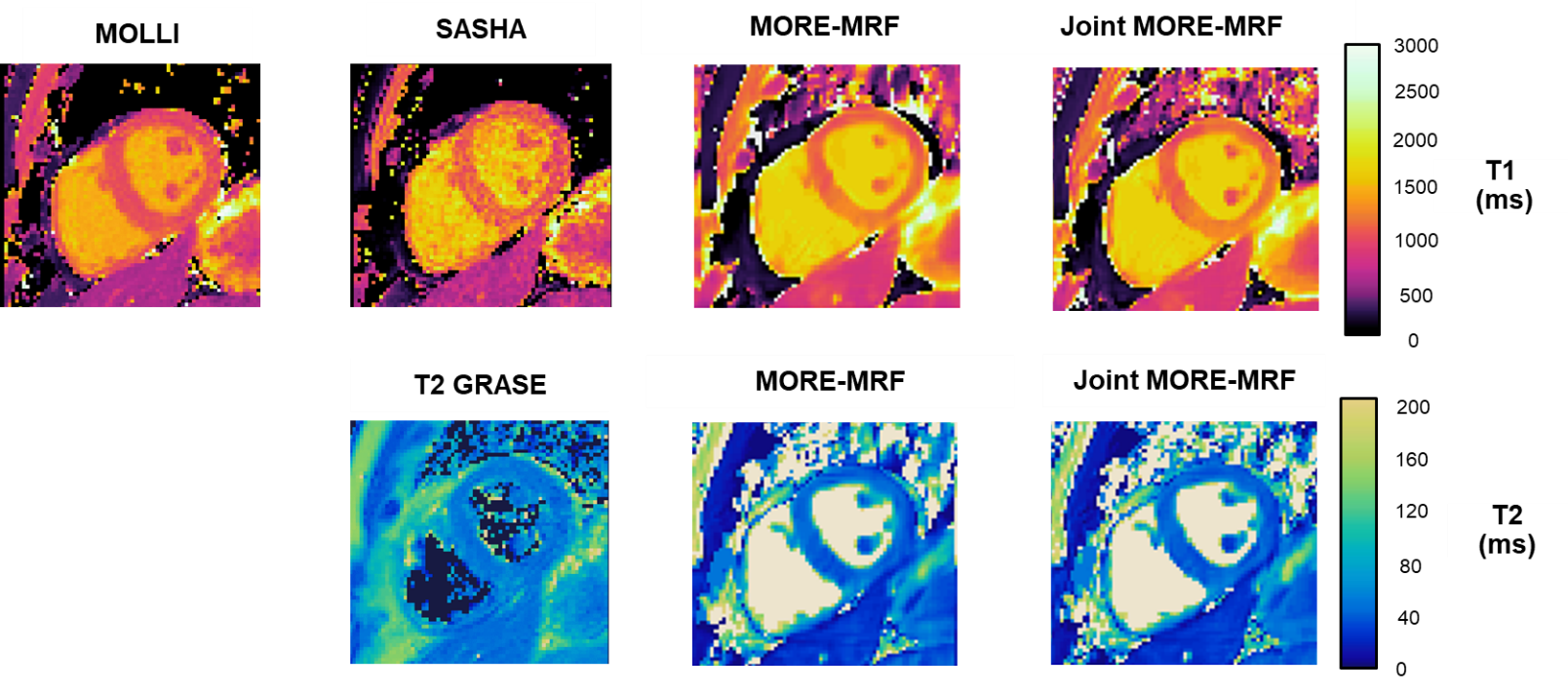
jMORE-MRF leading to more detailed parametric maps. Comparison between diastolic maps
obtained with T1-MOLLI, T1-SASHA, T2-GRASE, MORE-MRF and jMORE-MRF are shown in
Fig.4. Although good qualitative correspondence can be observed between the techniques,
some blurring can be observed with MORE-MRF which is resolved with jMORE-MRF. Average
diastolic T1 measurement and standard deviation on 5 subjects for
SASHA, MOLLI, MORE-MRF and joint MORE-MRF are 1132±100ms, 1025±37ms, 1174±73ms and
1138.4±69ms respectively. T2 values for T2GRASE, MORE-MRF and
jMORE-MRF are 52±5ms, 45±5ms and 44±5ms.
A
comparison between MORE-MRF and jMORE-MRF for 16 cardiac phases is shown in
Fig.5. Temporal profiles show improved map quality using jMORE-MRF compared to
MORE-MRF. Dynamic T1 map, T2 map and synthetic bSSFP cine
are also included in Fig. 5 for jMORE-MRF.Conclusions
Improvements of a continuous 2D free-running myocardial MRF framework have been demonstrated with the proposed jMORE-MRF reconstruction. This novel motion resolved multi-contrast reconstruction framework enables simultaneous cardiac function and quantitative tissue characterisation, with high image quality, by exploiting redundancies between the different cardiac phases. jMORE-MRF doubled the number of achievable cardiac phases with respect to the previously proposed MORE-MRF. Future work will further validate the proposed approach in healthy subjects and patients with cardiovascular disease.Acknowledgements
This work was supported by EPSRC (EP/L015226/1, EP/P001009/1, EP/P032311/1) and Wellcome EPSRC Centre for Medical Engineering (NS/ A000049/1).References
1. Kim PK, Hong YJ, Im DJ, et al. Myocardial T1 and T2 Mapping : Techniques and Clinical Applications. 2017;18:113–131.
2. Hamilton JI, Jiang Y, Chen Y, et al. MR fingerprinting for rapid quantification of myocardial T 1 , T 2 , and proton spin density. Magn. Reson. Med. 2017;77:1446–1458 doi: 10.1002/mrm.26216.
3. Hamilton JI, Jiang Y, Ma D, et al. Investigating and reducing the effects of confounding factors for robust T1 and T2 mapping with cardiac MR fingerprinting. Magn. Reson. Imaging 2018;53:40–51 doi: 10.1016/J.MRI.2018.06.018.
4. Ma D, Gulani V, Seiberlich N, et al. Magnetic resonance fingerprinting. Nature 2013;495:187–92 doi: 10.1038/nature11971.
5. Jaubert O, Cruz G, Schneider T, Rueckert D, Botnar RM, Prieto C. MORE-MRF:Towards Motion Resolved Cardiac Multi-Parametric Mapping with Magnetic Resonance Fingerprinting. Proc. 26th Annu. Meet. ISMRM Paris,France. 2018.
6. Assländer J, Lattanzi R, Sodickson DK, Martijn A. Relaxation in Spherical Coordinates : Analysis and Optimization of pseudo-SSFP based MR-Fingerprinting. arXiv:2017:1–22.
7. Wundrak S, Paul J, Ulrici J, Hell E, Rasche V. A Small Surrogate for the Golden Angle in Time-Resolved Radial MRI Based on Generalized Fibonacci Sequences. IEEE Trans. Med. Imaging 2015;34:1262–1269 doi: 10.1109/TMI.2014.2382572.
8. Bustin A, Cruz G, Jaubert O, Lopez K, Botnar RM, Prieto C. High-Dimensionality Undersampled Patch-Based Reconstruction (HD-PROST) for Accelerated Multi-Contrast Magnetic Resonance Imaging. Proc. 27th Annu. Meet. ISMRM Montr. Canada. 2019.
9. Bustin A, Ginami G, Cruz G, et al. Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction. Magn. Reson. Med. 2018 doi: 10.1002/mrm.27354.
10. Assländer J, Cloos MA, Knoll F, Sodickson DK, Hennig J, Lattanzi R. Low rank alternating direction method of multipliers reconstruction for MR fingerprinting. Magn. Reson. Med. 2018;79:83–96 doi: 10.1002/mrm.26639.
11. Zhang T, Pauly JM, Levesque IR. Accelerating parameter mapping with a locally low rank constraint. Magn. Reson. Med. 2015;73:655–661 doi: 10.1002/mrm.25161.
12. Cruz G, Bustin A, Jaubert O, Schneider T, Botnar RM, Prieto C. Locally Low Rank Regularization for Magnetic Resonance Fingerprinting. Proc. 26th Annu. Meet. ISMRM Paris,France. 2018.
13. Captur G, Gatehouse P, Kellman P, et al. A T1 and ECV phantom for global T1 mapping quality assurance: The T1 mapping and ECV standardisation in CMR (T1MES) program. J. Cardiovasc. Magn. Reson. 2016;18:W14 doi: 10.1186/1532-429X-18-S1-W14.
14. Messroghli DR, Radjenovic A, Kozerke S, Higgins DM, Sivananthan MU, Ridgway JP. Modified Look-Locker inversion recovery (MOLLI) for high-resolutionT1 mapping of the heart. Magn. Reson. Med. 2004;52:141–146 doi: 10.1002/mrm.20110.
15. Chow K, Flewitt JA, Green JD, Pagano JJ, Friedrich MG, Thompson RB. Saturation recovery single-shot acquisition (SASHA) for myocardial T1 mapping. Magn. Reson. Med. 2014;71:2082–2095 doi: 10.1002/mrm.24878.
16. Sprinkart AM, Luetkens JA, Träber F, et al. Gradient Spin Echo ( GraSE ) imaging for fast myocardial T2 mapping. J. Cardiovasc. Magn. Reson. 2015;17:12 doi: 10.1186/s12968-015-0127-z.
Figures