0803
First in Human: MRI-guided radiation therapy of the heart with implantable cardiac defibrillator1Radiation Oncology, Radiology, and Biomedical Engineering, Washington University in St Louis, St Louis, MO, United States, 2Radiation Oncology, Washington University in St Louis, St Louis, MO, United States, 3Cardiovascular Diseases and Electrophysiology, Washington University in St Louis, St Louis, MO, United States, 4Radiation Oncology, Barnes Jewish Hospital, St Louis, MO, United States, 5Radiation Oncology and Biomedical Engineering, Washington University in St Louis, St Louis, MO, United States, 6Cardiology, Loyola University Medical Center, Maywood, IL, United States
Synopsis
Low-field (0.35 T) magnetic resonance imaging guided radiation therapy (MR-IGRT) was used for the first time to treat a patient with a cardiovascular implantable electronic device (CIED) and a cardiac fibroma located on the left ventricle. Stereotactic body radiation therapy (SBRT) was delivered in 5 fractions at a dose of 700 cGy/fraction with MRI-based real-time tumor tracking and beam gating. Lessons learned include the need for metal artifact suppression, higher MRI temporal resolution, and MRI safety workflows adapted to radiation oncology.
Purpose:
In
this report, low-field (0.35 T) magnetic resonance imaging (MRI) guided
radiation therapy (MR-IGRT) was used for the first time to simulate and treat a
patient with an unresectable cardiac fibroma and a cardiovascular implantable
electronic device (CIED). MR-IGRT is an attractive modality for treating the
heart due to MRI's superior soft tissue contrast and the ability to delineate
heart structures versus cone beam CT (CBCT).
At
our institution, MRIs are routinely performed on patients with CIEDs in the
Department of Radiology. In the Department of Radiation Oncology (RO), we
routinely treat patients with CIEDs on CBCT image-guided radiation therapy
(IGRT) systems but not on MRI.Methods:
A 61-year old Caucasian male patient with an unresectable left ventricular cardiac fibroma was treated using a low-field (0.35 T) MRI-Linac (ViewRay, Oakwood Village, OH). The patient had an MR Conditional implantable cardiac defibrillator (ICD, Medtronic Evera Surescan Model DDMC3D4) and leads (Model 5076 CapSureFix Novus and Model 6935 Sprint Quattro Secure S). The patient was classified by the cardiologist as standard risk (not device-dependent with MR Conditional device). The ICD was cleared by RO physicists for radiation dose and MRI despite the off-label use at low-field.1
Based on lessons learned from Radiology and Radiation Oncology MRI screening, an improved MRI safety protocol was employed to ensure patient safety during the MRI simulation and subsequent therapies. A time-out was performed prior to the vendor device specialist reprogramming the ICD and the radiation therapist setting up the patient for the MR-IGRT.
The ViewRay MR-IGRT currently uses axial 3D and sagittal 2D cine true fast imaging with steady-state precession (TrueFISP). The axial 3D TrueFISP covered a 24 cm high volume with 1.6x1.6x3 mm voxels in a single exhalation breathhold [flip angle: 600, 17 s acquisition, 385 Hz/pixel]. The sagittal 2D cine TrueFISP acquired a single 3.5x3.5x7 mm slice at four frames/s [flip angle: 600, 1351 Hz/pixel, two averages]. However, these sequences were vulnerable to null band artifacts from the ICD. Alternative gradient echo pulse sequences were tested offline to eliminate the null band artifacts.
The patient first received a low-field MRI simulation for treatment planning that included a 3D volume acquisition and a 2D cine to evaluate the feasibility of real-time gating. Based on the success of the simulation, stereotactic body radiation therapy (SBRT) was delivered in five fractions (over five consecutive days) using the MRI-Linac with 6MV flattening filter free (6FFF) photons. For each fraction, the MRI safety protocol was followed and the axial 3D TrueFISP images were acquired for patient setup and alignment to the treatment plan. Radiation was delivered using the 2D cine TrueFISP images to track the tumor and gate the beam.
Results:
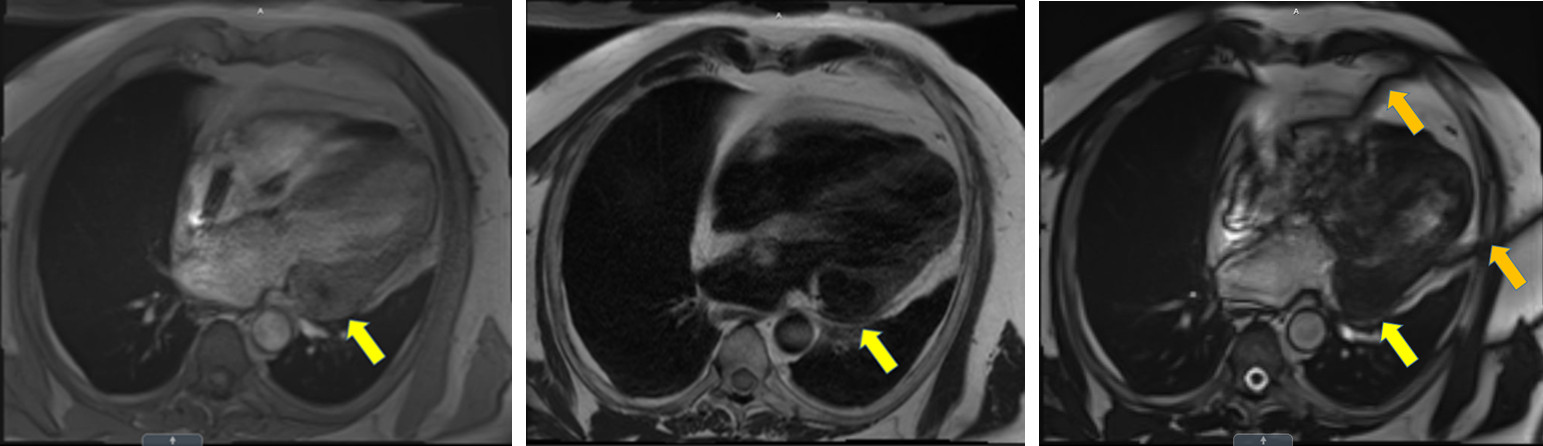
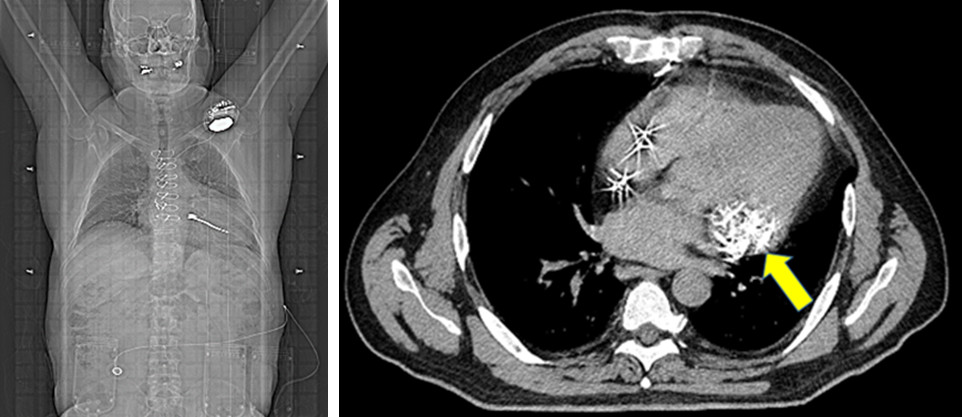
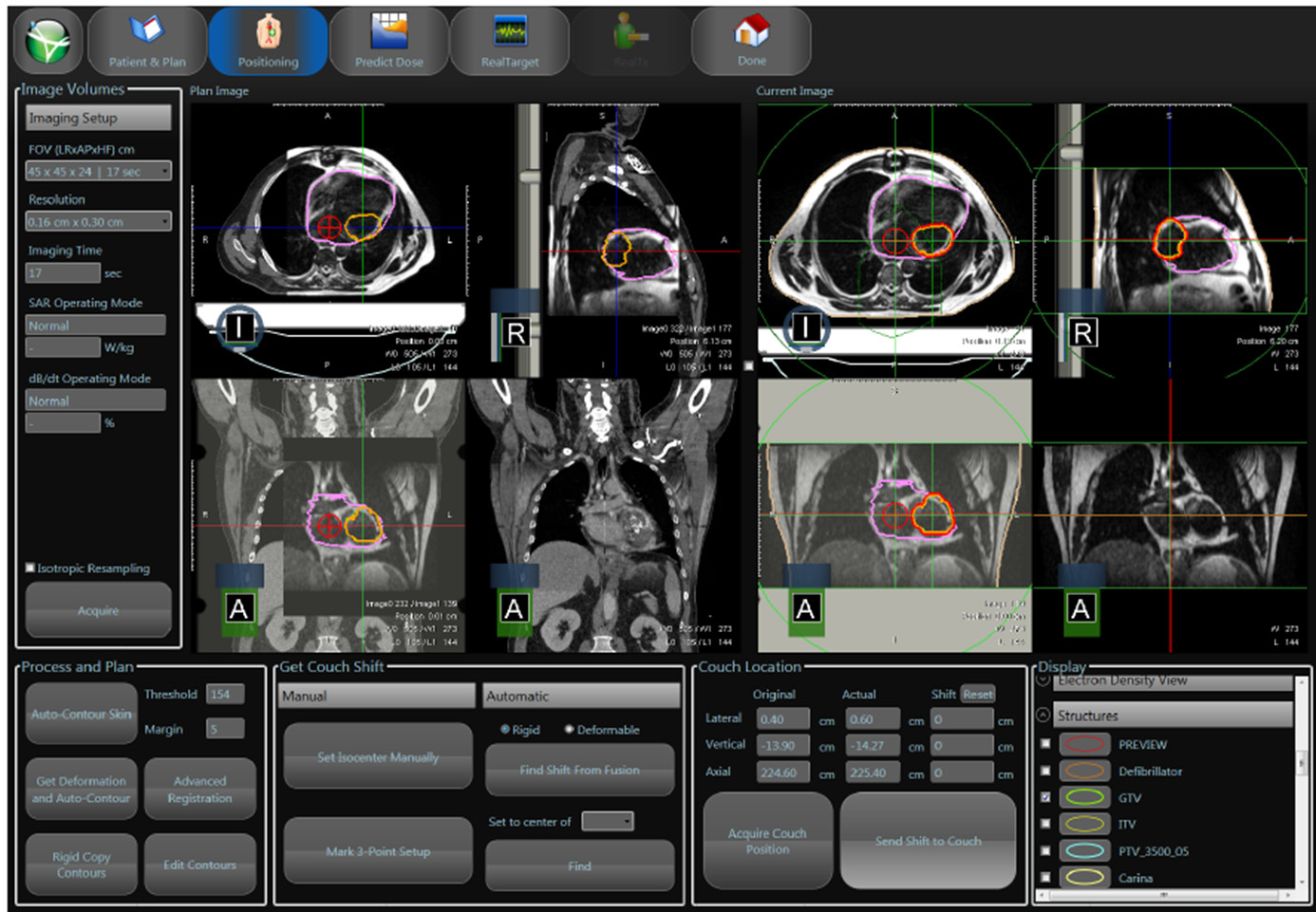
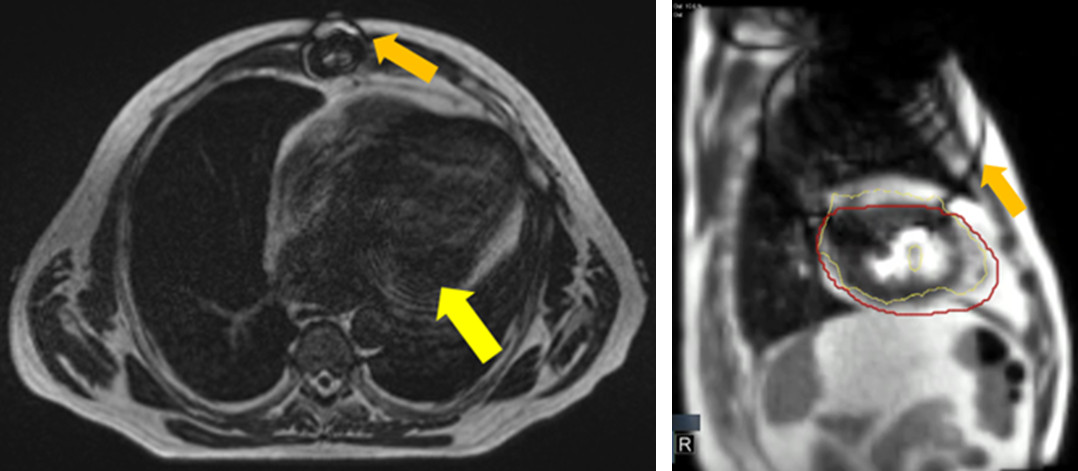
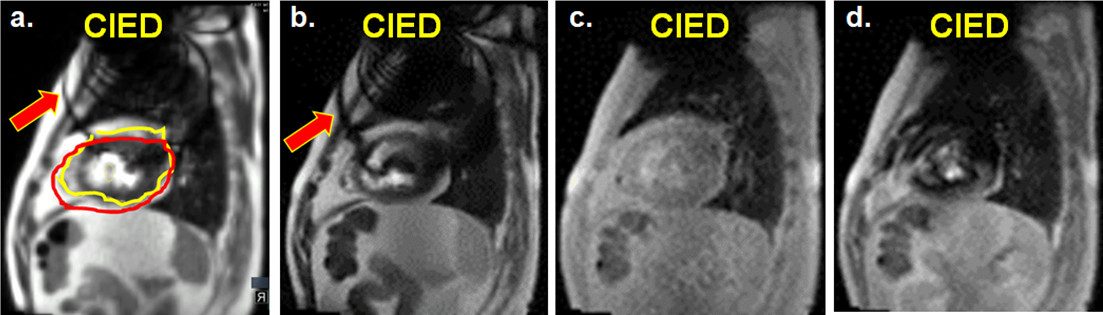
Diagnostic MRIs of the cardiac fibroma were performed one month prior to the RO consultation at the patient's local hospital (Fig. 1). CT simulations performed for treatment planning show the location of the ICD, leads, and sternal wires (Fig. 2). The MR-IGRT patient setup with the treatment plan is shown in Fig. 3. Low field 3D TrueFISP MRIs used in treatment planning and patient setup are shown in Fig. 4. 2D cine TrueFISP MRIs had null band artifacts intersecting the tracking and gating targets (Fig. 4). The alternative gradient echo sequences eliminated the null band artifacts but had a reduced contrast-to-noise ratio (CNR, Fig. 5).Discussion:
This is the first demonstration of MR-IGRT in a patient with a CIED. The patient was successfully treated without incident. Target tracking was not severely impacted by the presence of null bands in the gating target for this patient. 3D and 2D cine T1-weighted MRI eliminated null bands but the image quality suffered from low CNR.
Nevertheless, improvements in image quality and metal artifact reduction will enable MR-IGRT of the heart in CIED patients. Noninvasive stereotactic cardiac radiosurgery2 could create a large demand for MR-IGRT given the superior image quality of MRI versus conventional CBCT and the ability to track the target in real-time. The benefits of these therapies may increase the demand for MR-IGRT therapies in high-risk patients (e.g., with unsafe CIEDs or device dependence).
Conclusion:
CIEDs pose a significant challenge in MR-IGRT of the left thorax due to the potential for image artifacts and device irradiation. MRI safety is a critical concern since the device must be programmed into a safe mode for each MRI exam (MRI simulation and each treatment fraction). Improved alternative sequences and image reconstructions are required to minimize the effects of artifacts on treatment planning and real-time beam gating.Acknowledgements
No acknowledgement found.References
1. Indik, Julia H., et al. 2017 HRS expert consensus statement on magnetic resonance imaging and radiation exposure in patients with cardiovascular implantable electronic devices. Heart Rhythm 14(7):e97-e153 (2017).
2. Cuculich PS, Schill MR, Kashani R, et al. Noninvasive cardiac radiation for ablation of ventricular tachycardia. N. Engl. J. Med. 377:2325-2336 (2017).
Figures