0797
Safety evaluation of human exposure to a 10.5T whole body magnet: protocol design and preliminary results.1Center for Magnetic Resonance Research, University of Minnesota, Minneapolis, MN, United States, 2Psychology, University of Minnesota, Minneapolis, MN, United States, 3School of Public Health Biostatistics, University of Minnesota, Minneapolis, MN, United States, 4Otolaryngology, Head and Neck Surgery, University of Minnesota, Minneapolis, MN, United States, 5Neurology, University of Minnesota, Minneapolis, MN, United States
Synopsis
We present the initial results of our 10.5T safety study measuring the impact on cognitive, vestibular, and physiological metrics. Data from 17 subjects show evidence of short term (same day) but no long term (weeks) fatigue, increased nystagmus upon initial exposure to static field, with no relevant effect on physiological measures when at isocenter.
Audience
Researchers and clinicians interested in understanding the biological effects of UHF static magnetic fields and study designs to evaluate such effects.Purpose
The promise of increased signal- and contrast-to-noise ratios to advance biomedical discovery drives the development of MRI systems with ever increasing static magnetic fields. However, currently 8 Tesla is considered the upper limit for the first level controlled operation mode (IEC 60601-2-33 V3.2 1), and above 8T is still classified as representing significant risk by the US Food and Drug Administration2 (FDA). Therefore, specific subject safety considerations need to be addressed prior to using a >8T system for research in IRB approved studies addressing biomedical questions. In December of 2014, we brought a 10.5T whole body magnet to field. Subsequent to obtaining safety data on animal models showing no effect on vitals3 and applying to the FDA for an Investigational Device Exemption (IDE), we commenced safety studies with human subjects in December 2017 under an IDE. The potential impact of high magnetic fields on cognitive, vestibular and physiologic function are the main targets of the safety study because they have been reported on at various field strengths with sometimes contradictory results in preclinical and theoretical evaluations. The current study was designed to investigate field effects specifically including the long term impact of field exposure (i.e. over several weeks) in addition to the acute effects. This work presents a summary of our safety study protocol and a preliminary analysis of the data obtained.Methods
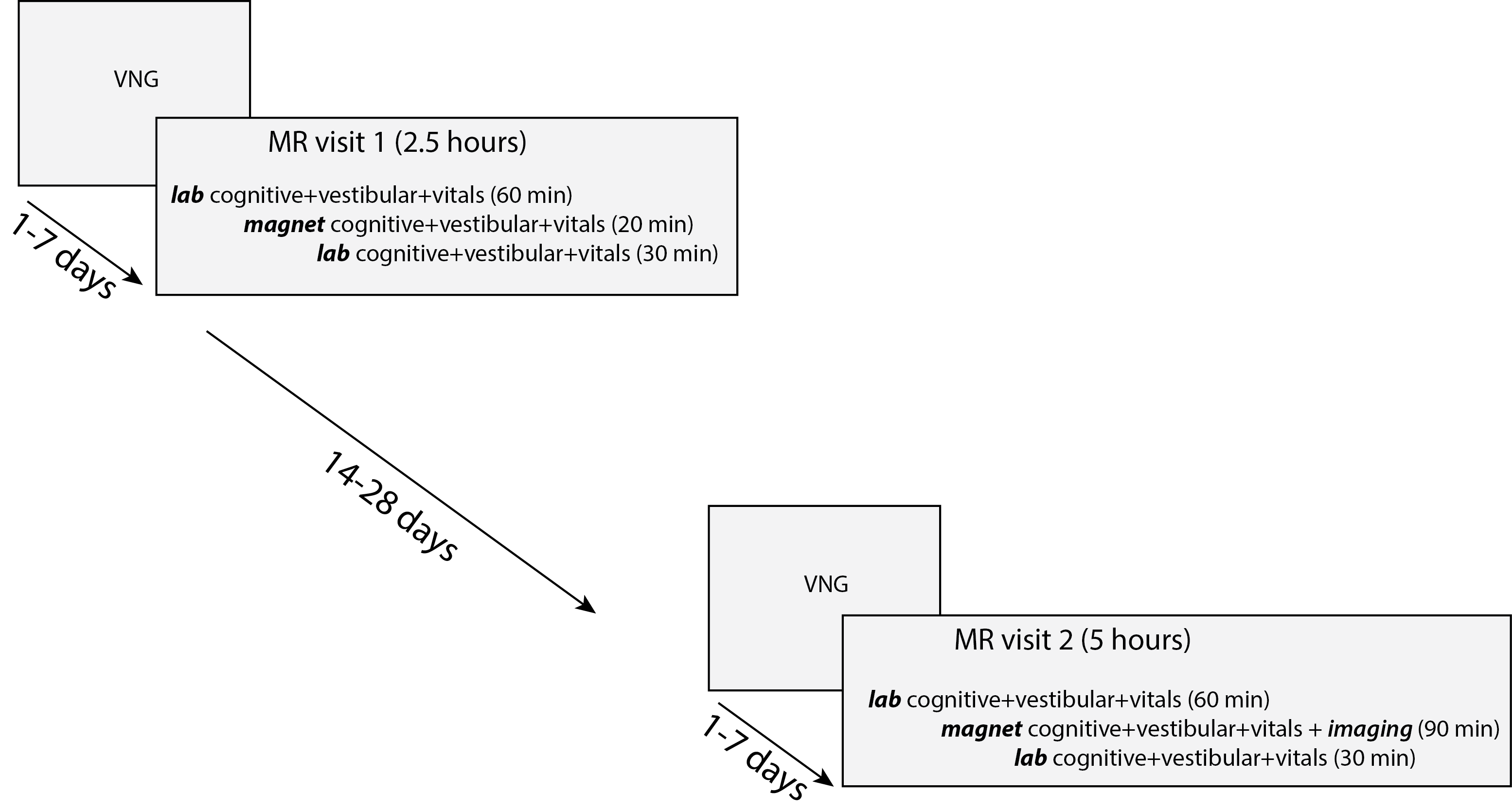
After IRB approval, subjects were recruited and screened using a standard MRI safety evaluation and a study specific medical questionnaire which was reviewed by the study physician. Additional mandatory exclusion criteria included any metallic implants or pregnancy. Approved subjects participated in the two-phase study consisting of four relevant encounters shown in Figure 1. The first magnet exposure is ~20 minutes; the second magnet exposure, 2-4 weeks later, includes imaging and lasts 90 minutes. The cognitive tests include short term memory (WAIS-IV letter number sequence and digit span4, HVLT-R5) and executive functioning (SDMT6, Trailmaking Test7); vestibular tests comprise smooth pursuit and spontaneous eye movement; physiological monitoring includes heart rate, oxygen saturation, blood pressure, and respiration rate. Only raw scores are used for the cognitive tests as non-normed versions of the tests were created so that they could be administered multiple times per visit.
- There were a possible 253 data points per individual per phase.
- Some test sub-measures were combined using previously defined summary values in the scoring guide or in the literature8.
Differences between phases or components of a phase were evaluated using paired student t-tests and significance determined with a two-sided significance level of 0.05.
Results
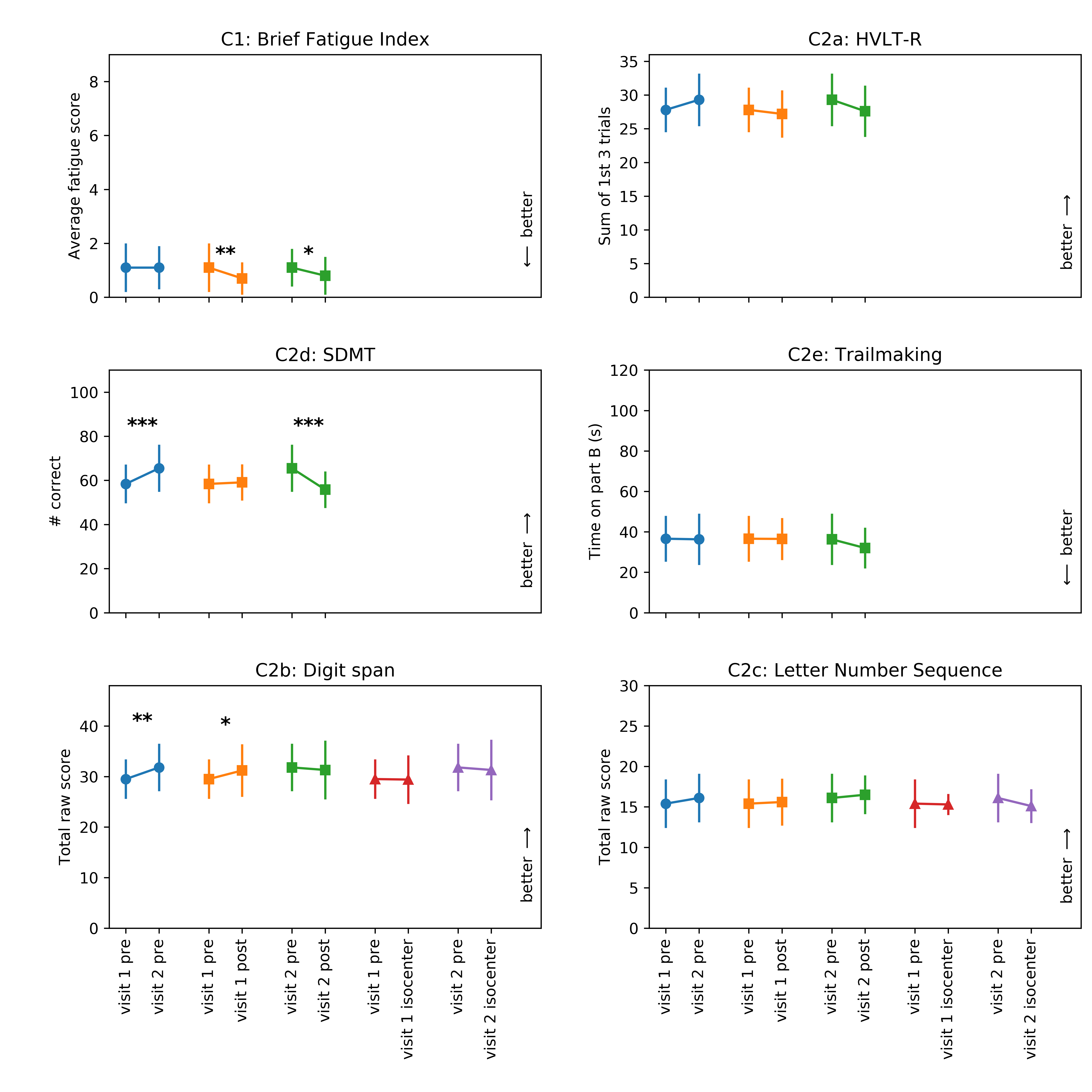
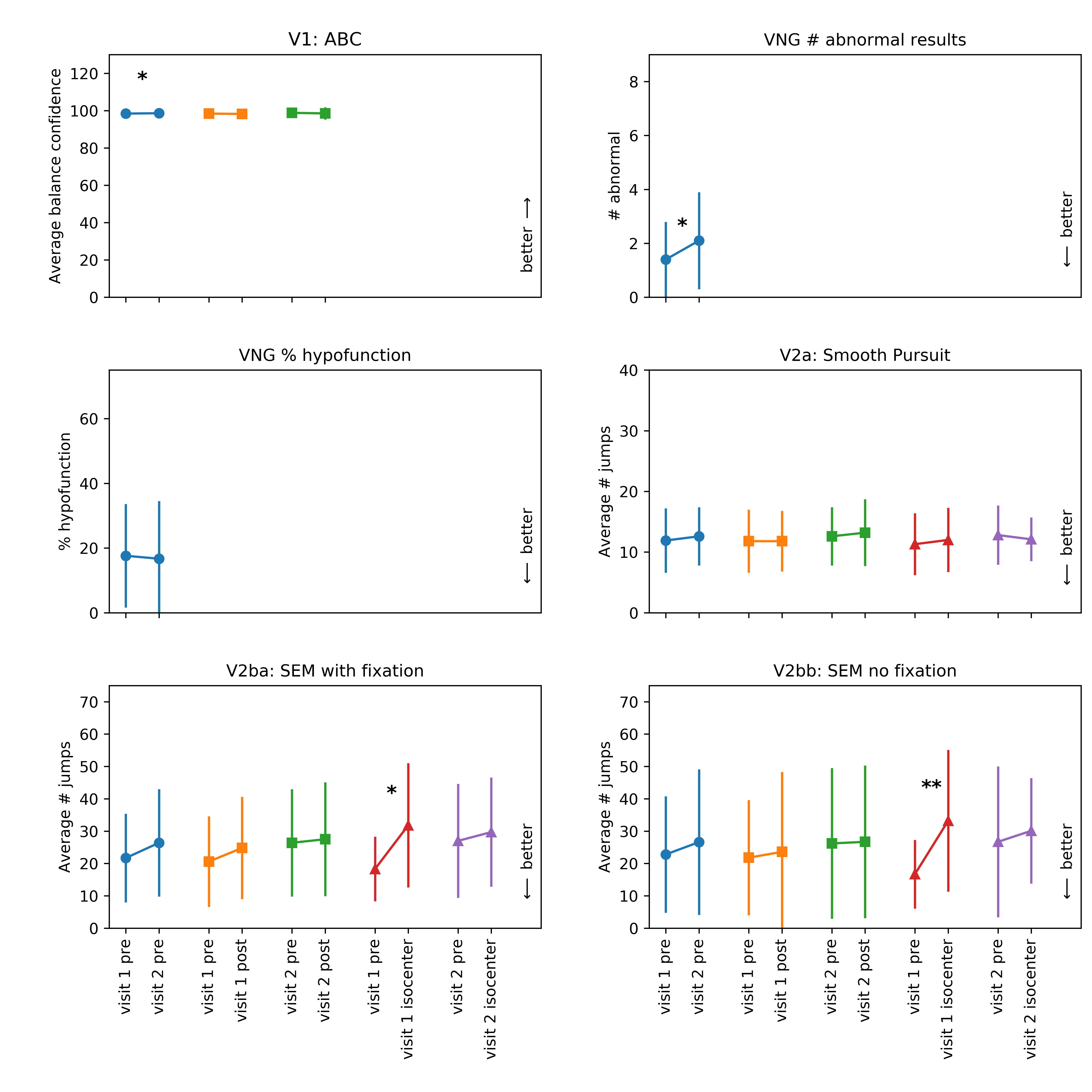
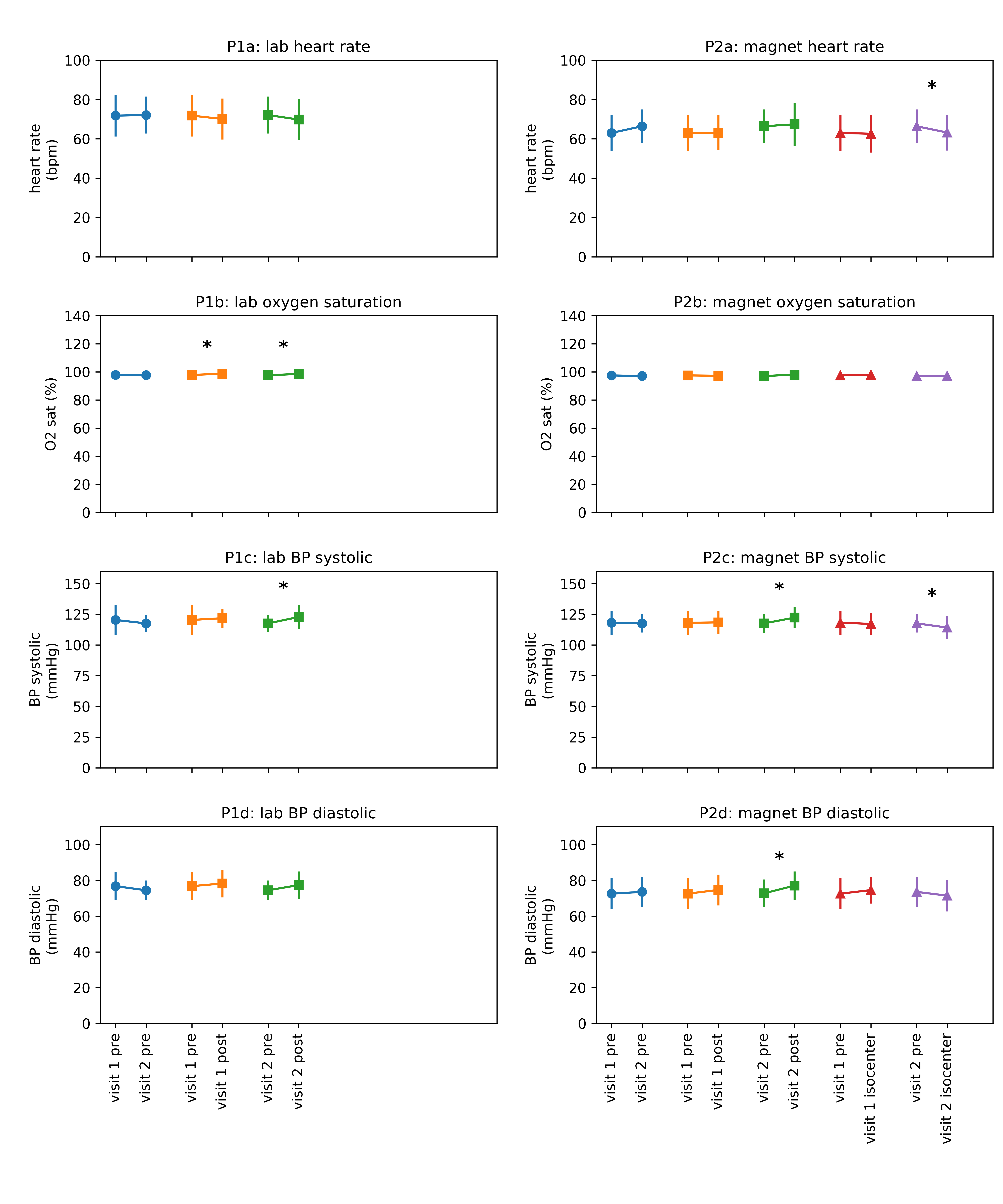
Results from the first 17 subjects (11 male, age ranges from 20-64, mean age=35.8) are shown in Figures 2 (cognitive), 3 (vestibular) and 4 (physiological). We were particularly interested in examining:
- long term effects (before-magnet visit 1 versus before-magnet visit 2)
- short term effects (before versus after magnet, same visit)
- isocenter effects (before-magnet versus isocenter)
Notable long term effects include improved performance on the digit span and SDMT, likely from practice effects. Short term effects include reduced next-day fatigue and increased digit span scores, with worse performance on SDMT in visit 2 and an increase in blood pressure in visit 2. The latter results could be explained by the long duration of visit 2 (approximately 5 hours). The most striking isocenter effect is an increase in nystagmus during visit 1; the lack of such effect during visit 2 could be explained by general acclimation to the static field or in relation to the timing of test administration (1-2 minutes after reaching isocenter during visit 1 versus ~15 minutes after reaching isocenter during visit 2 due to the imaging study). Decreased heart rate and blood pressure were also observed during visit 2 isocenter.
Discussion/Conclusion
While
statistical significance was observed in some comparisons, the biological
significance and/or competing factors needs to be further studied and will be
investigated before concluding this study as will methods to account for the
learning effects.
In the attempt to obtain as much data as
possible to capture primary and secondary effects of field exposure, the study
required many resources, created logistical challenges and included repeated
testing increasing the potential of learning effects. While we believe this
study will accomplish the needed evaluation of the static magnetic field on
human subjects, future evaluations of other high field systems can learn from the
current protocol and outcomes in order to tailor efforts on the most meaningful
or impactful evaluations.Acknowledgements
Supported by: NIBIB P41 EB015894, U01 EB025144, NIH S10 RR029672.References
1. International Electrotechnical
Commission (IEC). Particular requirements for the safety of magnetic resonance
equipment for medical diagnosis. International Standard IEC 60601-2-33. 2010.
2. U.S. Department of Health and Human Services, Food and Drug Administration, Center for Devices and Radiological Health. Guidance for Magnetic Resonance Diagnostic Devices – Criteria for Significant Risk Investigations. 1997.
3. Eryaman Y, Zhang P, Utecht L, et al. Investigating the physiological effects of 10.5 Tesla static field exposure on anesthetized swine. Magn Reson Med. 2018; 79(1):511-514. doi: 10.1002/mrm.26672
4. Wechsler D. Wechsler Adult Intelligence Scale—Fourth Edition. San Antonio, TX: Pearson; 2008.
5. Benedict R H, Schretlen D, Groninger L, Brandt J. Hopkins Verbal Learning Test—Revised: Normative Data and Analysis of Inter-Form and Test-Retest Reliability. The Clinical Neuropsychologist. 1998; 12 (1): 43-55.
6. Smith A. The Symbol Digit Modalities Test (SDMT):manual. Western Psychological Services; 1982.
7. Reitan R M, Wolfson D. The Halstead-Reitan neuropsycholgical test battery: Theory and clinical interpretation. Tucson, AZ: Neuropsychological Press; 1985.
8. Kuslansky G, Kat, M, Verghese J, et al. Detecting dementia with the Hopkins Verbal Learning Test and the Mini-Mental State Examination. Archives of Clinical Neuropsychology. 2004; 19 (1): 89 - 104.
Figures