0789
Simultaneous myocardial T1 and T2 mapping in 11 heartbeats using a radial sequence with inversion recovery and T2 preparation1Department of Radiological Sciences, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 2Department of Medicine, Division of Cardiology, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 3Division of Cardiology, Veterans Affairs Greater Los Angeles Healthcare System, Los Angeles, CA, United States, 4Biomedical Physics Inter-Departmental Graduate Program, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
Myocardial T1 and T2 mapping are promising cardiovascular magnetic resonance (CMR) techniques for quantitative tissue characterization and provide complementary information. Simultaneous T1 and T2 mapping strategies are attractive because of shorter scan time and the potential for inherently co-registered T1/T2 maps. By estimating T1 and T2 at the same time, the T2/T1 bias present in conventional T1 and T2 mapping sequences can be minimized and more accurate T1 and T2 estimation accomplished. In this work, we sought to develop a simultaneous T1 and T2 mapping technique that can achieve high accuracy and precision, without heart-rate dependence, and with high reproducibility comparable to the standard MOLLI and conventional T2 mapping techniques.
Introduction
Myocardial T1 and T2 mapping are promising cardiovascular magnetic resonance (CMR) techniques for quantitative tissue characterization1-4 and provide complementary information. Simultaneous T1 and T2 mapping strategies are attractive because of shorter scan time and the potential for inherently co-registered T1/T2 maps. By estimating T1 and T2 at the same time, the T2/T1 bias present in conventional T1 and T2 mapping sequences can be minimized and more accurate T1 and T2 estimation accomplished. In this work, we sought to develop a simultaneous T1 and T2 mapping technique that can achieve high accuracy and precision, without heart-rate dependence, and with high reproducibility comparable to the standard MOLLI and conventional T2 mapping techniques.Methods
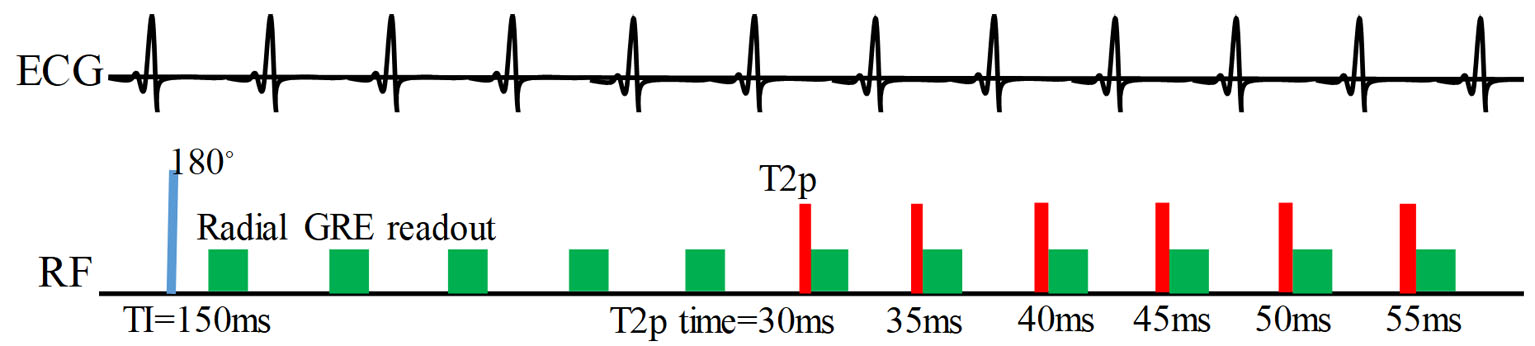
Figure 1 illustrates the proposed sequence, which uses combined inversion recovery and T2-preparation with a golden angle, radial, spoiled gradient echo readout. After the raw data were acquired using the proposed radial sequence, the magnitude and phase images were reconstructed using view sharing and compressed sensing5. We then extended a previously described BLESSPC6 T1 estimation algorithm to calculate T1 and T2 maps simultaneously, which was based on Bloch equations.
We determined reference T1 and T2 values using the standard spin-echo sequences in phantom studies. We tested the proposed sequence, MOLLI, and a conventional T2- preparation mapping at simulated heart rate (HR) ranging from 40 bpm to 100 bpm (10 increments). For T1 and T2 precision testing, we repeated the test 10 times at a simulated heart rate of 60 bpm. In vivo, we repeated the three sequences three times at the same mid-left ventricular short-axis position at end-expiration in 10 healthy volunteers.
Results
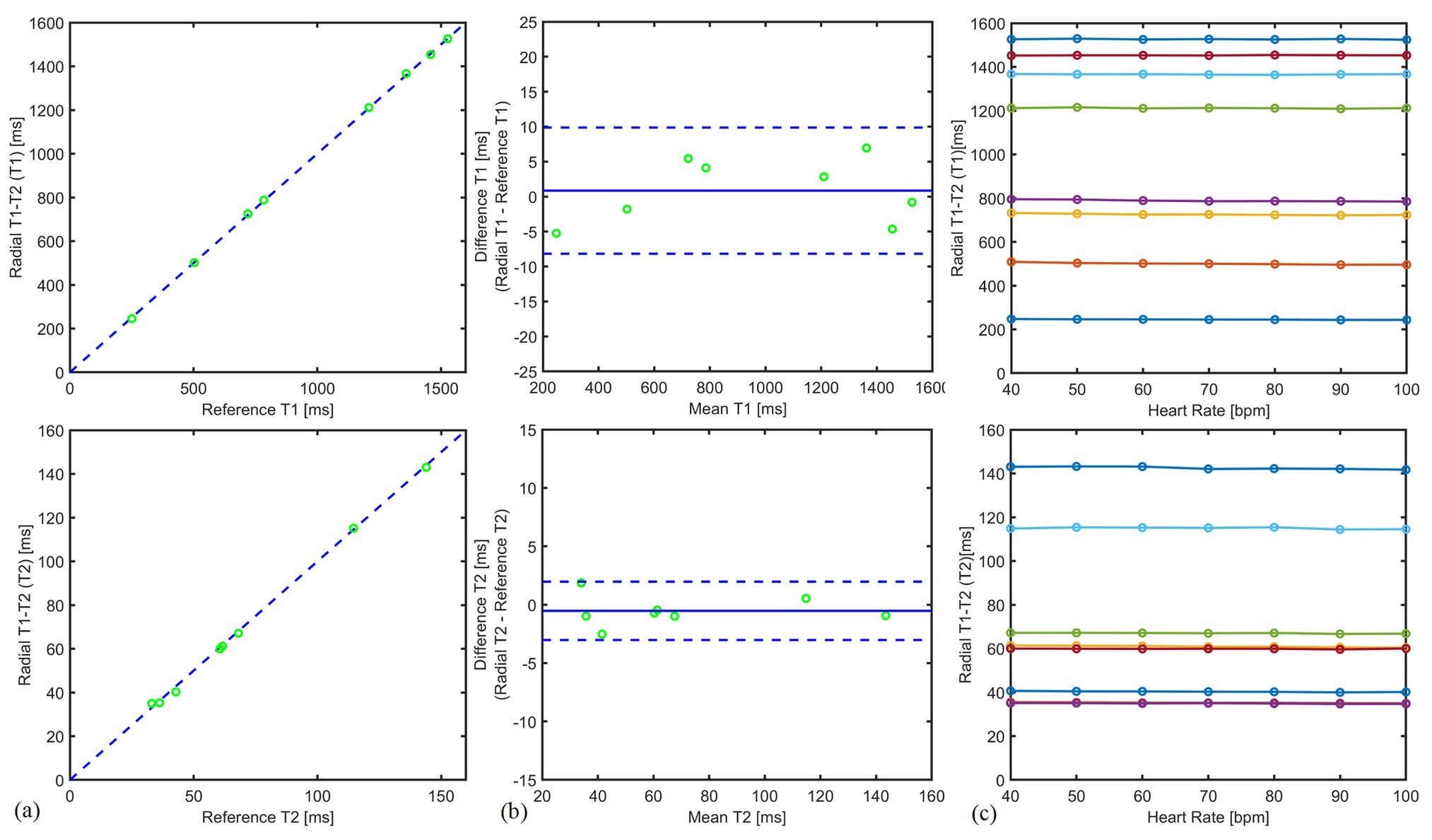
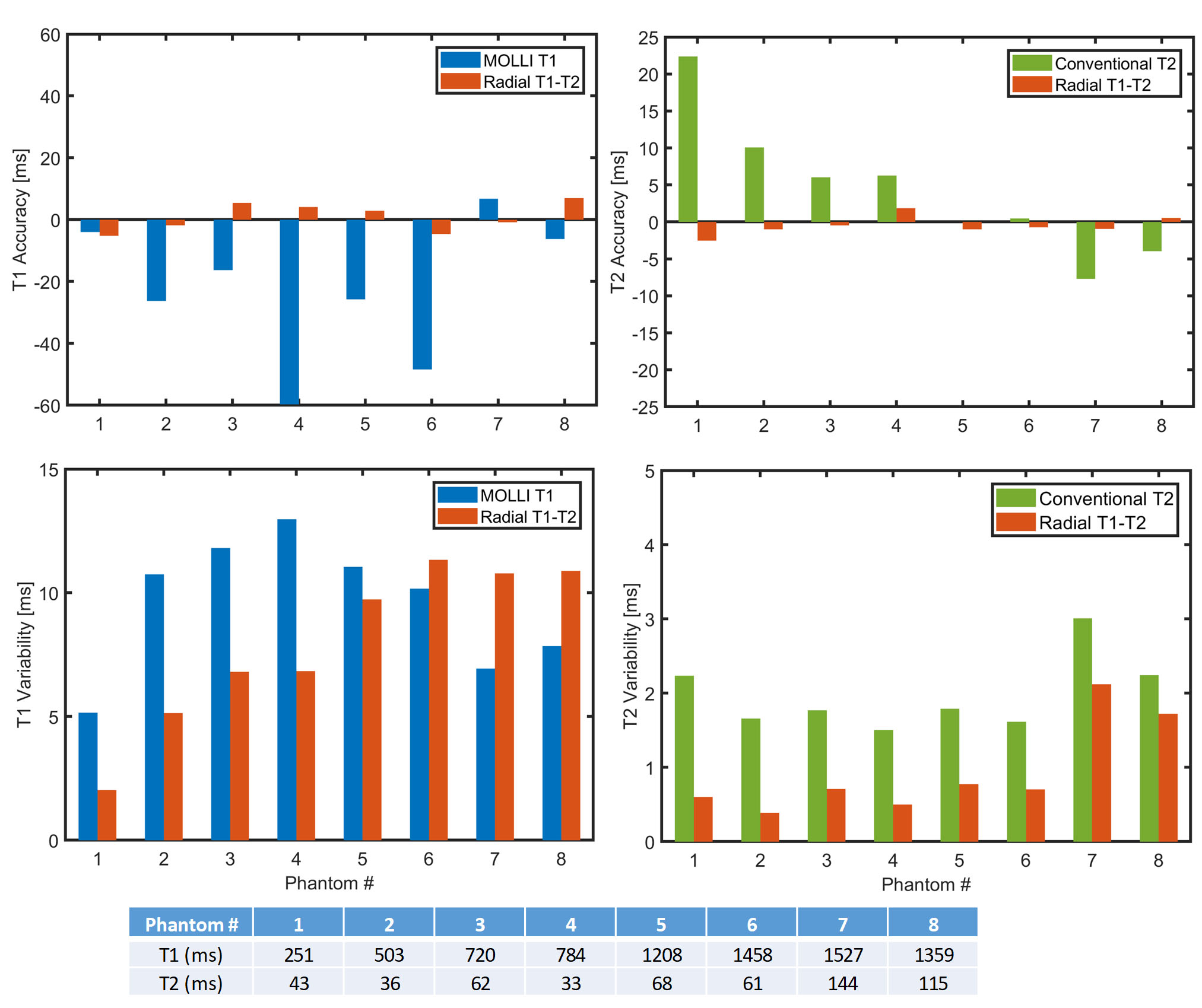
Figure 2 shows T1 and T2 estimation results of the proposed method compared to reference T1 and T2 values, as well as the results at different heart rates in phantom studies. The measured T1 and T2 values show a strong correlation with reference T1 and T2 values (correlation coefficients > 0.999 for both T1 and T2). The maximum difference using the proposed method was 0.7% for T1 measurements and 0.4% for T2 measurements for a heart rate range of 40 - 100 bpm. Our proposed technique is more accurate than MOLLI (p < 0.05) while achieving similar precision (p = 0.3) in T1 estimation (Figure 3). Compared to conventional T2 mapping, our radial technique is more accurate (p <0.05) and precise (p<0.001).
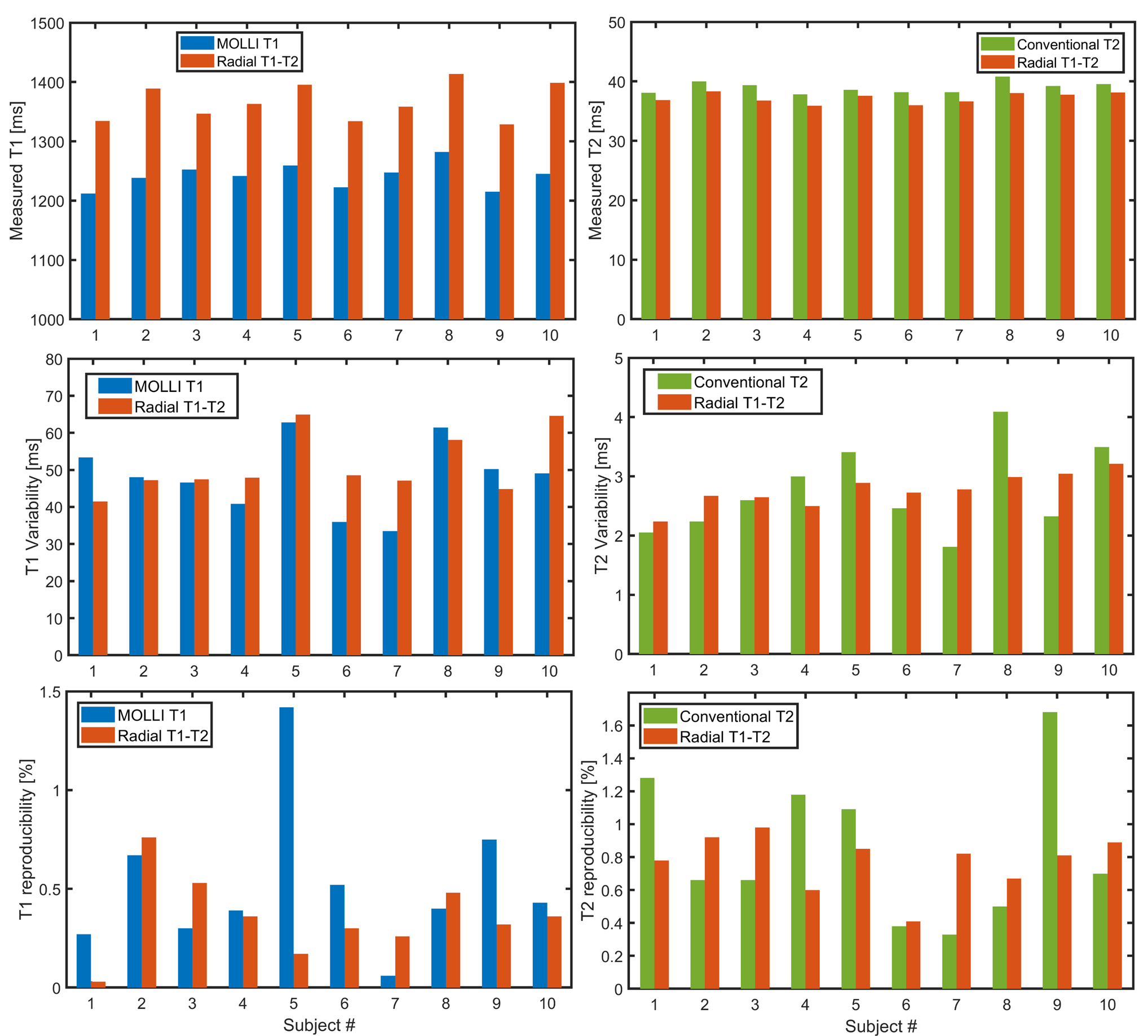
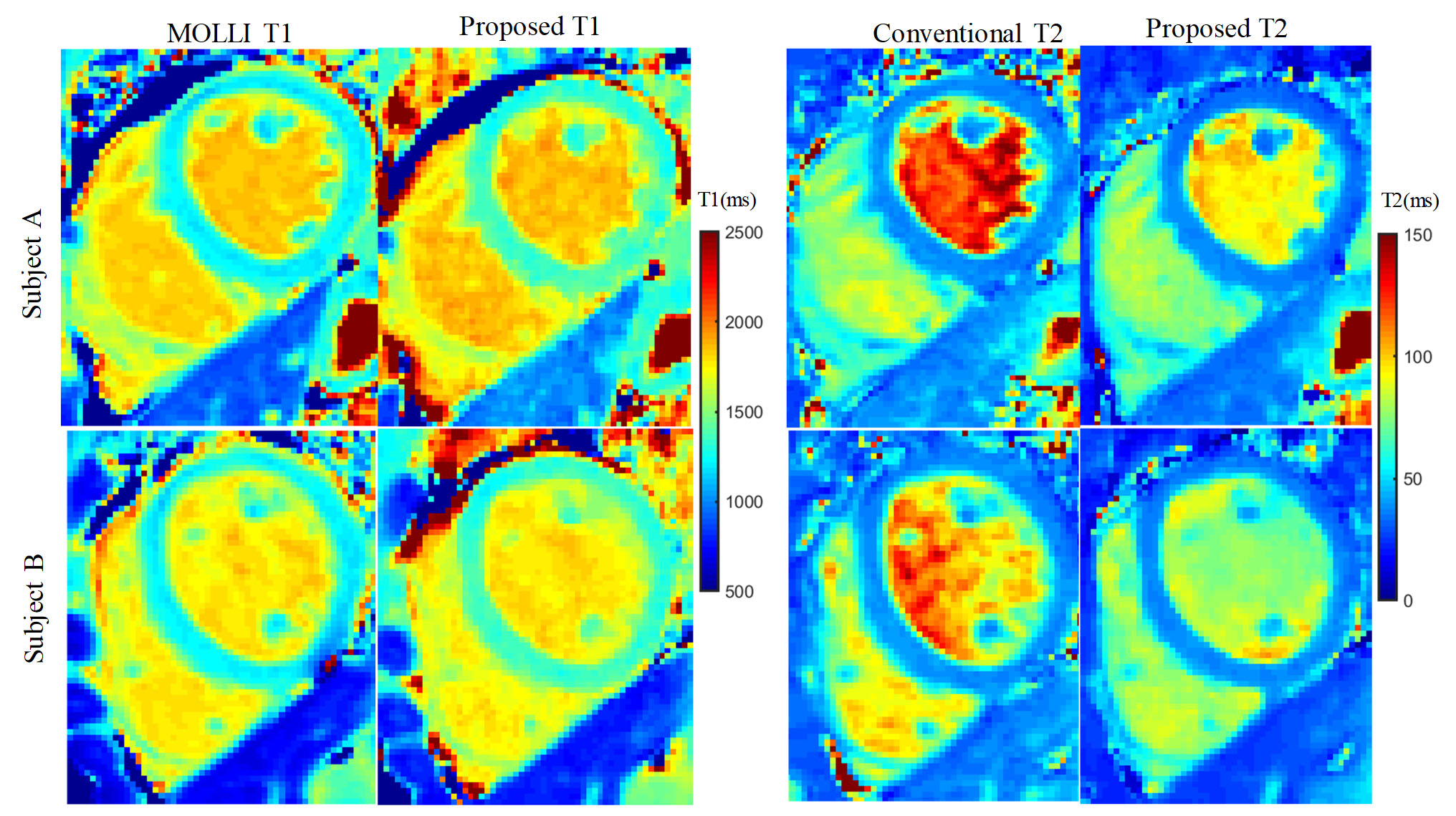
Figure 4 provides a comparison among our radial T1-T2 approach, MOLLI, and conventional T2 mapping sequences for each volunteer. The left ventricular (LV) myocardial T1 and T2 values, T1 and T2 variability across the entire LV myocardium, and reproducibility as reflected by the coefficient of variation for the mean LV myocardial T1 are results from three repeated scans. Compared to MOLLI, our proposed technique yielded significantly higher T1 estimates (1366±31 ms vs. 1242±21 ms, p<0.001) with similar reproducibility (51±8 ms vs. 48±10 ms, p=0.3) in vivo. Compared to conventional T2 mapping techniques, the T2 values obtained using our proposed approach are significantly lower (37.2±8.9 ms vs. 39.0±9.7 ms, p<0.001, p< 0.001) with similar reproducibility (2.8±0.3 ms vs. 2.7±0.7 ms, p =0.6). Figure 5 shows examples of T1 and T2 maps generated in two different subjects using our proposed method compared to those generated and by product MOLLI T1 and conventional T2 mapping sequences.
Discussion
For simultaneous myocardial T1 and T2 mapping, several techniques have been proposed; most have used Cartesian acquisitions7-11, which limits the number of images that can be reconstructed for parameters fitting. Using a golden angle radial acquisition scheme enabled our approach to leverage view sharing for improvement of T1 and T2 precision through reconstruction of a large dataset. Recent work demonstrated the feasibility of MR fingerprinting for simultaneous myocardial T1 & T2 quantification12. However, to ensure good accuracy and precision, fingerprinting requires a relatively long breath-hold (16 heartbeats) and an acquisition window of 240 – 280 ms. Our proposed approach may be more promising for simultaneous T1/T2 mapping because it requires only 11 heartbeats and has a shorter acquisition window (~200 ms).Conclusion
The proposed radial T1-T2 mapping method allows for accurate, precise, and simultaneous myocardial T1 and T2 mapping in a single breath-hold with 11 heartbeats. For T1 and T2 estimation, our proposed technique achieved reproducibility comparable to the reference MOLLI T1 and conventional T2 mapping techniques while reducing scan time and exhibiting better accuracy without heart rate dependence.Acknowledgements
Research reported in this publication was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under Award Number R01HL127153.References
1. Messroghli DR, Moon JC, Ferreira VM, et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imagi. J. Cardiovasc. Magn. Reson. 2017;19:75.
2. Bohnen S, Radunski UK, Lund GK, Kandolf R, Stehning C, Schnackenburg B, Adam G, Blankenberg S, Muellerleile K. Performance of T1 and T2 Mapping Cardiovascular Magnetic Resonance to Detect Active Myocarditis in Patients With Recent-Onset Heart Failure. Circ. Cardiovasc. Imaging 2015;8:e003073.
3. Lurz P, Luecke C, Eitel I, et al. Comprehensive Cardiac Magnetic Resonance Imaging in Patients With Suspected Myocarditis. J. Am. Coll. Cardiol. 2016;67:1800–1811.
4. Mewton N, Liu CY, Croisille P, Bluemke D, Lima JAC. Assessment of myocardial fibrosis with cardiovascular magnetic resonance. J. Am. Coll. Cardiol. 2011;57:891–903.
5. Marty B, Coppa B, Carlier PG. Fast, precise, and accurate myocardial T1mapping using a radial MOLLI sequence with FLASH readout. Magn. Reson. Med. 2018;79:1387–1398.
6. Shao J, Rapacchi S, Nguyen K-L, Hu P. Myocardial T1 mapping at 3.0 tesla using an inversion recovery spoiled gradient echo readout and bloch equation simulation with slice profile correction (BLESSPC) T1 estimation algorithm. J. Magn. Reson. Imaging 2016;43:414–25.
7. Blume U, Lockie T, Stehning C, Sinclair S, Uribe S, Razavi R, Schaeffter T. Interleaved T 1 and T 2 relaxation time mapping for cardiac applications. J. Magn. Reson. Imaging 2009;29:480–487.
8. Kvernby S, Warntjes MJB, Haraldsson H, Carlhäll C-J, Engvall J, Ebbers T. Simultaneous three-dimensional myocardial T1 and T2 mapping in one breath hold with 3D-QALAS. J. Cardiovasc. Magn. Reson. 2014;16:102.
9. Akçakaya M, Weingärtner S, Basha TA, Roujol S, Bellm S, Nezafat R. Joint myocardial T1 and T2 mapping using a combination of saturation recovery and T2 -preparation. Magn. Reson. Med. 2016;76:888–96.
10. Xanthis CG, Bidhult S, Greiser A, Chow K, Thompson RB, Arheden H, Aletras AH. Simulation-based quantification of native T1 and T2 of the myocardium using a modified MOLLI scheme and the importance of Magnetization Transfer. Magn. Reson. Imaging 2018;48:96–106.
11. Santini F, Kawel-Boehm N, Greiser A, Bremerich J, Bieri O. Simultaneous T 1 and T 2 quantification of the myocardium using cardiac balanced-SSFP inversion recovery with interleaved sampling acquisition (CABIRIA). Magn. Reson. Med. 2015;74:365–371.
12. Hamilton JI, Jiang Y, Chen Y, Ma D, Lo W-C, Griswold M, Seiberlich N. MR fingerprinting for rapid quantification of myocardial T1, T2, and proton spin density. Magn. Reson. Med. 2017;77:1446–1458.
Figures