0783
Heartbeat-to-Heartbeat Quantitative Myocardial Oxygenation Imaging within a Single Breath-Hold using a Combined Gradient Echo-Spin Echo EPI (GESE-EPI) Sequence in Patients with Hypertension1A.A. Martinos Center for Biomedical Imaging, Boston, MA, United States, 2Department of Radiology, University Medical Center Groningen, Groningen, Netherlands, 3Cardiovascular Research Center, Massachusetts General Hospital, Boston, MA, United States, 4Medicine, Harvard Medical School, Boston, MA, United States, 5Department of Nuclear Medicine and Molecular Imaging, University Medical Center Groningen, Groningen, Netherlands, 6Department of Radiology, Harvard Medical School, Boston, MA, United States, 7Medical Imaging Centre of Southwest Finland, Turku University Hospital, Turku, Finland, 8Division of Health Sciences and Technology, Harvard-MIT, Cambridge, MA, United States
Synopsis
Dynamic Cardiac BOLD imaging techniques can suffer from signal variabilities due to changes in heartrate during a breath-hold. We demonstrate that a 2-echo-GESE-EPI sequence can provide T2- and T2*-weighted images simultaneously per heartbeat, but the dynamic changes in these images represent physiological effects mixed with heartrate changes. We then proposed a 5-echo-GESE-EPI for dynamic T2- and T2*-mapping per heartbeat as a readout for myocardial oxygenation. These dynamically acquired T2- and T2*-values were demonstrated to increase over the time of a breath-hold for healthy volunteers, while shown to remain constant and even reverse in hypertension patients.
Introduction
Cardiac magnetic resonance offers several tools to determine tissue characteristics and can assess tissue oxygenation by making use of the different paramagnetic properties of hemoglobin[1]. Measure of myocardial oxygenation could help determine the presence of microvascular dysfunction which is believed to be associated with increased risks in cardiovascular diseases, for example in hypertension[2]. The challenge for this disease is that the oxygenation is not strongly altered as in vascular stenosis[3] and only a dynamic imaging approach might show the alterations. A number of T2 and T2* relaxation-based sequences can measure oxygenation in the myocardium[4], however there remains a trade-off between quantitative or dynamic measurements. This work shows that a dynamic signal intensity (SI) based sequence could be prone to heartrate changes and proposes a 5-echoes modified gradient-echo-spin-echo-EPI (GESE-EPI) sequence to mitigate this issue by providing T2- and T2*-maps per heartbeat. The sequence is used to acquire breath-hold data on healthy subjects and hypertension patients to determine oxygenation.Methods
GESE-EPI sequences were applied to 7 healthy volunteers (one with a BMI>25) on a 3T Skyra and 3 hypertension patients on a 3T Prisma Siemens MRI with a Body-18 and Spine-32 coil using: ECG triggering at end-diastole, acceleration RinplanexRzoom=2x3, res=2.77x2.77x7mm, two asymmetric saturation pulses were used and FOVPE was decreased to 38.1% (FOV=127x350x92mm). Two separate acquisitions were performed: 1)dual-echo GESE-EPI with TEs=9.8/38ms, TR=120ms, and 2)5-echo GESE with TEs=9.8/21.61/34.24/46.86/59.48ms, TR=120ms. The resulting images from the 5-echo-GESE-EPI were used to create T2- and T2*-mapping per heartbeat, using an iterative parameter fitting technique[5]. The images and heartrates from the 2-echo-GESE-EPI acquisitions were compare with a Bloch simulated Mxy-variation based on the heartrate and a MOLLI(5(3)3)-based T1-value.
A T2prep-FLASH series (TE=0,25,55ms) were acquired to generate control T2-maps. For the healthy subjects FLASH series with 9 different TEs (3-21ms) were also acquired to provide control T2*-maps. Semi-automatically drawn ROIs in the septum were used to compare the GE and SE signal intensities and T2- and T2*-values from the GESE maps with the control T2- and T2*-maps. To determine dynamic changes of BOLD during a breath-hold a linear fit through the T2- and T2*-values of the septum was performed. Furthermore, the dynamically acquired GESE-EPI was performed twice in the same healthy to confirm reproducibility of the oxygenation rates.
Results
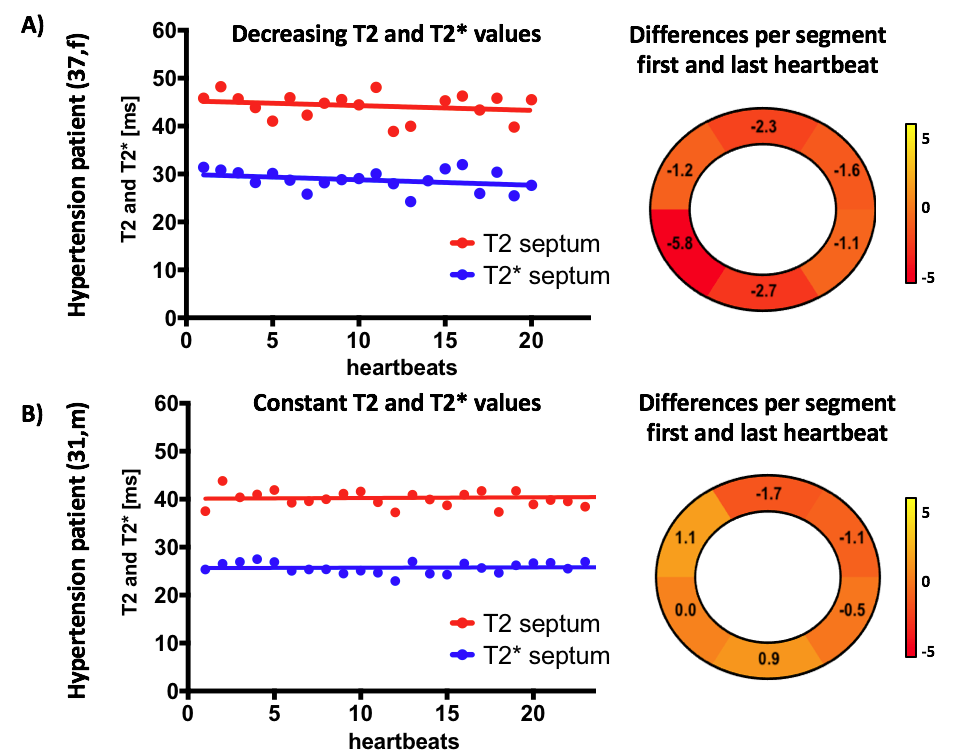
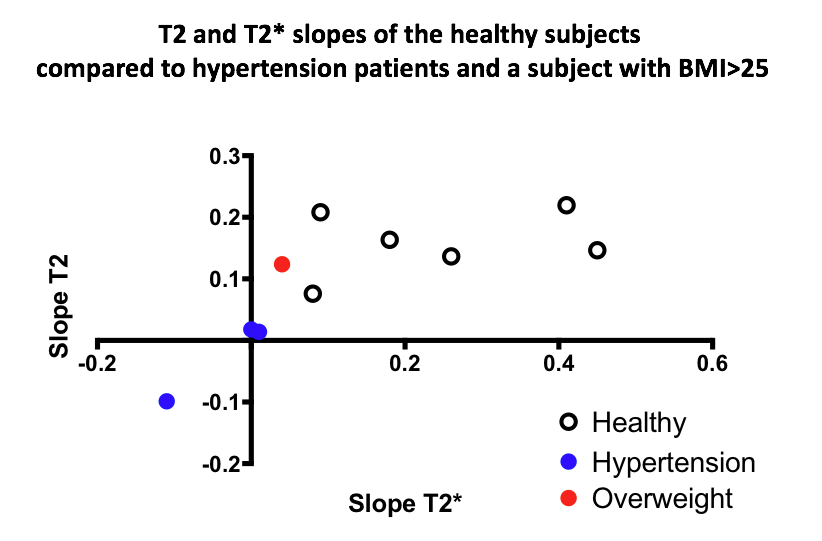
GE- and SE-images were acquired per heartbeat during a breath-hold using the 2-echo and 5-echo-GESE-EPI sequence. Fig1A shows the increase in RR-interval time of 21.5% observed in one subject, which translate to a predicted Mxy increase of 11.0% solely due to the heartrate. The acquired GE and SE images showed an increase in SI over time(Fig1B), which is a mixture of heartrate and oxygenation during the breath-hold. The 5-echo-GESE-EPI provides heartrate independent T2 and T2*-maps per heartbeat that shows a reduced increase of the T2- and T2*-values(Fig1C). Analysis of the septal ROI shows good correlation with the control mapping approaches in both healthy subjects and hypertension patients(Fig2). Furthermore, the change of the T2 and T2*-values during a breath-hold shows a significant positive slope in all healthy subjects which was also reproducible in a rescan(Fig3A). Most of the segments showed the same increase, except for one near the air-, liver-, lung-interface and one of the coronaries(Fig3B). Different T2- and T2*-changes were observed in the hypertension patients, where one subject showed a negative slope(Fig4A) and two others show approximate no change(Fig4B). This difference in slopes compared to healthy subjects might indicate an alteration of myocardial oxygenation. However, while all healthy controls show positive T2- and T2*-slopes, one subject with a BMI>25 showed a smaller increase(Fig5).Discussion
Where a signal intensity based cardiac dynamic BOLD sequence such as the 2-echo-GESE-EPI suffers from heartrate changes, the 5-echo-GESE-EPI shows T2 and T2*-maps per heartbeat over the time of a breath-hold that not influences by heartrates. The choice of slice position should not influence conclusions since microvascular dysfunction is expected to be diffuse[6]. The mechanism behind the increasing T2- and T2*-values is based on the increase in CO2 levels of the blood during a breath-hold, which triggers vasodilation[7]. Vasodilation could be compromised in hypertension patients[8] and this non-invasive oxygenation imaging approach might be able to assess this. Further research is needed to determine the correlation of these oxygenation measures and potential alterations in the oxygenation and vasculature.Conclusion
The 2-echo- and 5-echo-GESE-EPI were successfully applied to the heart and enabled dynamic myocardial T2- and T2*-imaging and mapping per heartbeat. The heartbeat-to-heartbeat T2- and T2*-maps give a direct measure of the myocardial oxygenation during a breath-hold. This approach could potentially offer a new MR technique for the analysis of microvasculature diseases.Acknowledgements
This work was supported in part by NIH research grants: R01EB020613, R01EB019437, P41EB015896, and the shared instrumentation grants: S10RR023401, S10RR019307, S10RR019254, S10RR023043References
1. Pauling L, Coryell CD. The Magnetic Properties and Structure of Hemoglobin, Oxyhemoglobin and Carbonmonoxyhemoglobin. Proc Natl Acad Sci. 1936;22:210–6
2. Camici PG, Crea F. Coronary Microvascular Dysfunction. N Engl J Med. 2007;:830–40
3. Fischer K, Yamaji K, Luescher S, Ueki Y, Jung B, Tengg-kobligk H Von, et al. Feasibility of cardiovascular magnetic resonance to detect oxygenation deficits in patients with multi-vessel coronary artery disease triggered by breathing maneuvers. 2018;:1–11.
4. Friedrich MG, Karamitsos TD. Oxygenation-sensitive cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2013;15:1
5. Schmiedeskamp H, Straka M, Newbould RD, Zaharchuk G, Andre JB, Olivot JM, et al. Combined spin- and gradient-echo perfusion-weighted imaging. Magn Reson Med. 2012;68:30–40.
6. Salerno M, Kramer CM. Advances in Parametric Mapping with Cardiac Magnetic Resonance Imaging. JACC Cardiovasc Imaging. 2014;6:806–22.
7. Fischer K, Guensch DP, Friedrich MG. Response of myocardial oxygenation to breathing manoeuvres and adenosine infusion. Eur Heart J Cardiovasc Imaging. 2015;16:395–401.
8. Arnold JR, Karamitsos TD, Bhamra-Ariza P, Francis JM, Searle N, Robson MD, et al. Myocardial oxygenation in coronary artery disease: Insights from blood oxygen level-dependent magnetic resonance imaging at 3 Tesla. J Am Coll Cardiol. 2012;59:1954–64
Figures