0782
Motion-Compensated 3D Whole-heart Water-Fat Late Gadolinium Enhancement Imaging for Assessment of Myocardial Viability1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare GmbH, Frimley, United Kingdom, 3Cardiovascular MR Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Water/fat 2D LGE imaging has shown promising results for assessment of fibro-fatty infiltration in the myocardium and characterisation of cardiac masses. However, spatial resolution and volumetric coverage within a clinically feasible scan time remain a challenge. Here we propose a highly efficient respiratory motion-compensated 3D whole-heart water/fat inversion recovery (IR)-prepared LGE imaging sequence. Preliminary results from patients with cardiovascular disease demonstrate the feasibility of the approach, with scan duration of ~8 min. Motion-compensated 3D LGE water images offer a good depiction of myocardial scar, while motion-compensated fat images offer complementary diagnostic information, with clear delineation of epicardial and pericardial fat.
Introduction
Late Gadolinium enhancement (LGE) cardiovascular MRI has been established as the reference technique for the assessment of myocardial viability1. Although inversion recovery (IR) and phase-sensitive IR (PSIR) 2D LGE are well-established techniques for infarct imaging, some technical challenges remain for accurate detection and quantification of fibrosis and scar in the myocardium. These challenges include increasing spatial resolution and coverage within a clinically feasible acquisition time, and improving characterisation and contrast of scar in the myocardium. Recent developments have focused on improving spatial resolution and volumetric coverage, by acquiring 3D datasets under free-breathing typically relying on diaphragmatic navigators for respiratory motion compensation2,3. Although this approach can result in good-quality high-resolution images for subjects with regular breathing, large variations in the respiratory efficiency among subjects may lead to long and unpredictable scan times and decreased image quality, hindering its integration into clinical routine. Water/fat LGE imaging has been recently proposed for distinguishing fibrosis from fatty infiltration of the myocardium, and improving characterisation of cardiac masses4,5. However, this approach has so far only been applied to 2D imaging under breath-holding.
Here we propose a novel undersampled motion-compensated 3D whole-heart water/fat LGE imaging approach. 2D image-navigators (iNAVs)6 are integrated in the acquisition to achieve 100% respiratory efficiency (no data rejection) and predictable scan time. Translational motion information from the iNAVs is exploited in the reconstruction to generate respiratory-resolved motion-corrected 3D images7, enabling high-resolution water/fat LGE imaging for the simultaneous visualisation of fibrous and fatty infiltration of the myocardium.
Methods
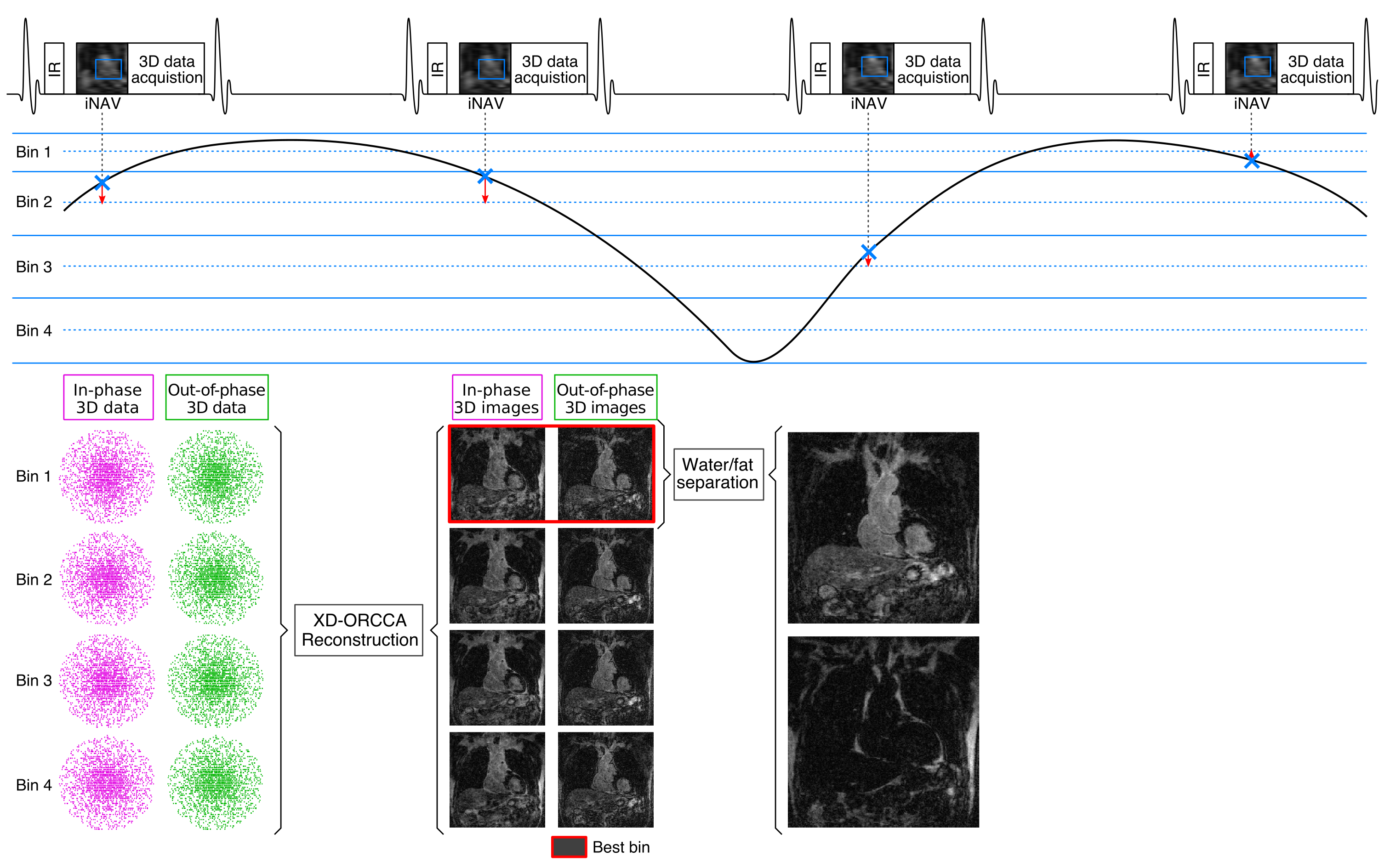
Acquisition consists of an ECG-triggered dual-echo 3D IR-prepared spoiled gradient echo sequence (Fig1a). 3D dual-echo data is acquired every second heartbeat with an undersampled variable-density golden-step Cartesian trajectory with spiral profile order sampling8. 2D iNAVs are also acquired every second heartbeat using low flip-angle excitation pulses before the 3D acquisition. Foot-head (FH) and right-left (RL) respiratory motion is estimated by tracking a template around the heart. FH motion is used to group the 3D dual-echo data into 4 equally populated respiratory bins, which are corrected for translational motion in both FH and RL directions and then jointly reconstructed using the XD-ORCCA7 approach (Fig1b). The respiratory bin with smallest FH displacements (usually end-expiration) is then used to compute 3D whole-heart water/fat LGE images.
Five patients (4 male, 60±10 years) with known or suspected cardiovascular disease were scanned on a 1.5T scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). The clinical protocol included a multi-breath-hold multi-slice 2D-PSIR LGE acquisition, including 2-chamber, 3-chamber, 4-chamber and stack of short-axis views (1.40-1.56mm in-plane resolution, 8mm slice thickness), starting ~10 min after administration of a Gd-based contrast agent (0.15mmol/kg). After conventional 2D LGE imaging, dual-echo 3D data were acquired with a prototype implementation of the proposed sequence and the following imaging parameters: coronal orientation, 3-fold undersampling, resolution=1.3×1.3×2.6mm3, interpolated to 1.3mm3 isotropic during image reconstruction, FOV=312×312×94-114mm3, TR/TE1/TE2=7.16/2.38/4.76ms, bipolar gradient readout, bandwidth=990Hz/px, FA=20°. A subject-specific trigger delay and acquisition window (~120ms) were set coinciding with mid-diastole, and inversion time was selected to null the signal from viable myocardium using a TI scout (Look-Locker) acquisition. 3D water/fat LGE images were reconstructed with the proposed undersampled motion-compensated method and with zero-filling and no motion correction for comparison purposes.
Results
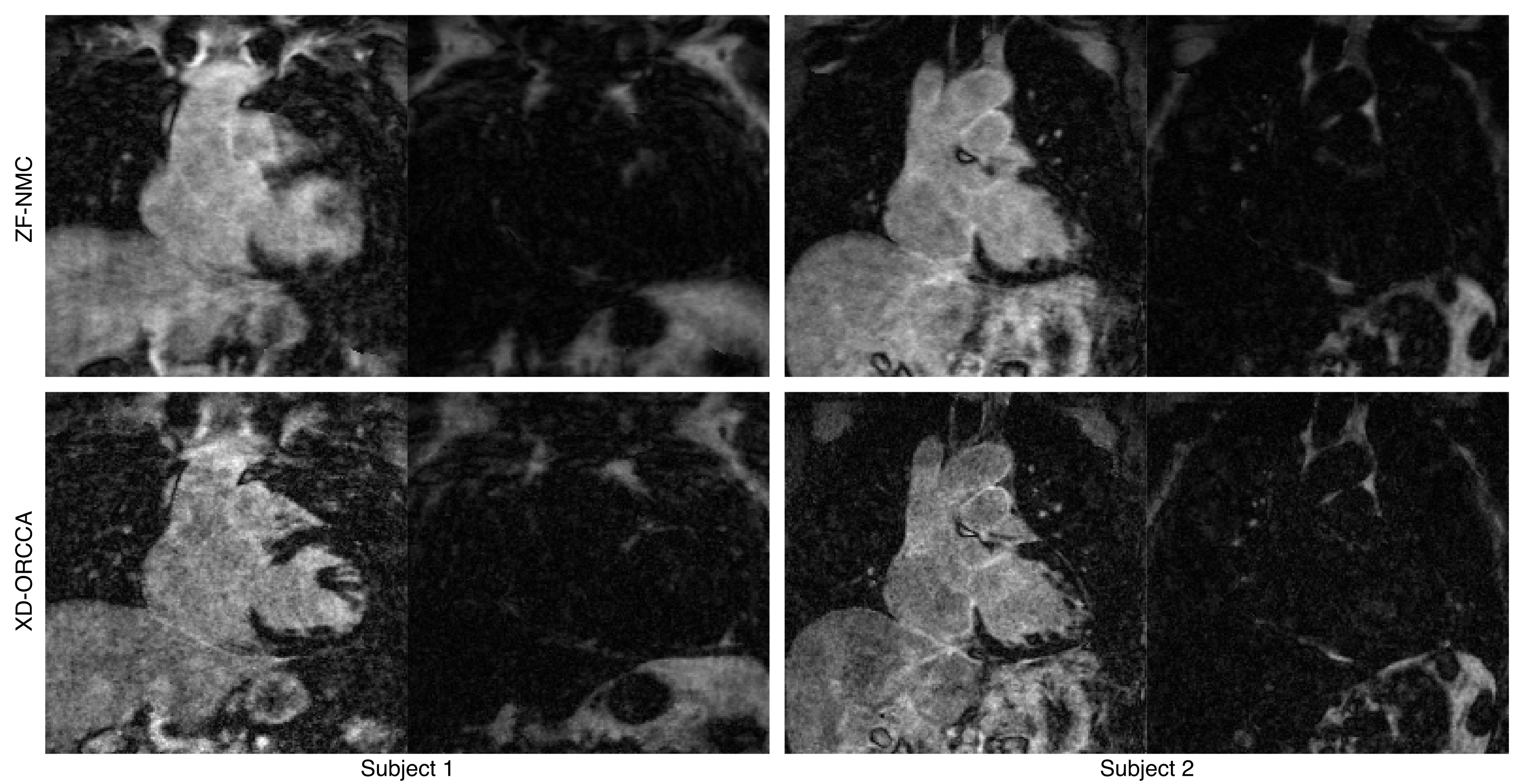
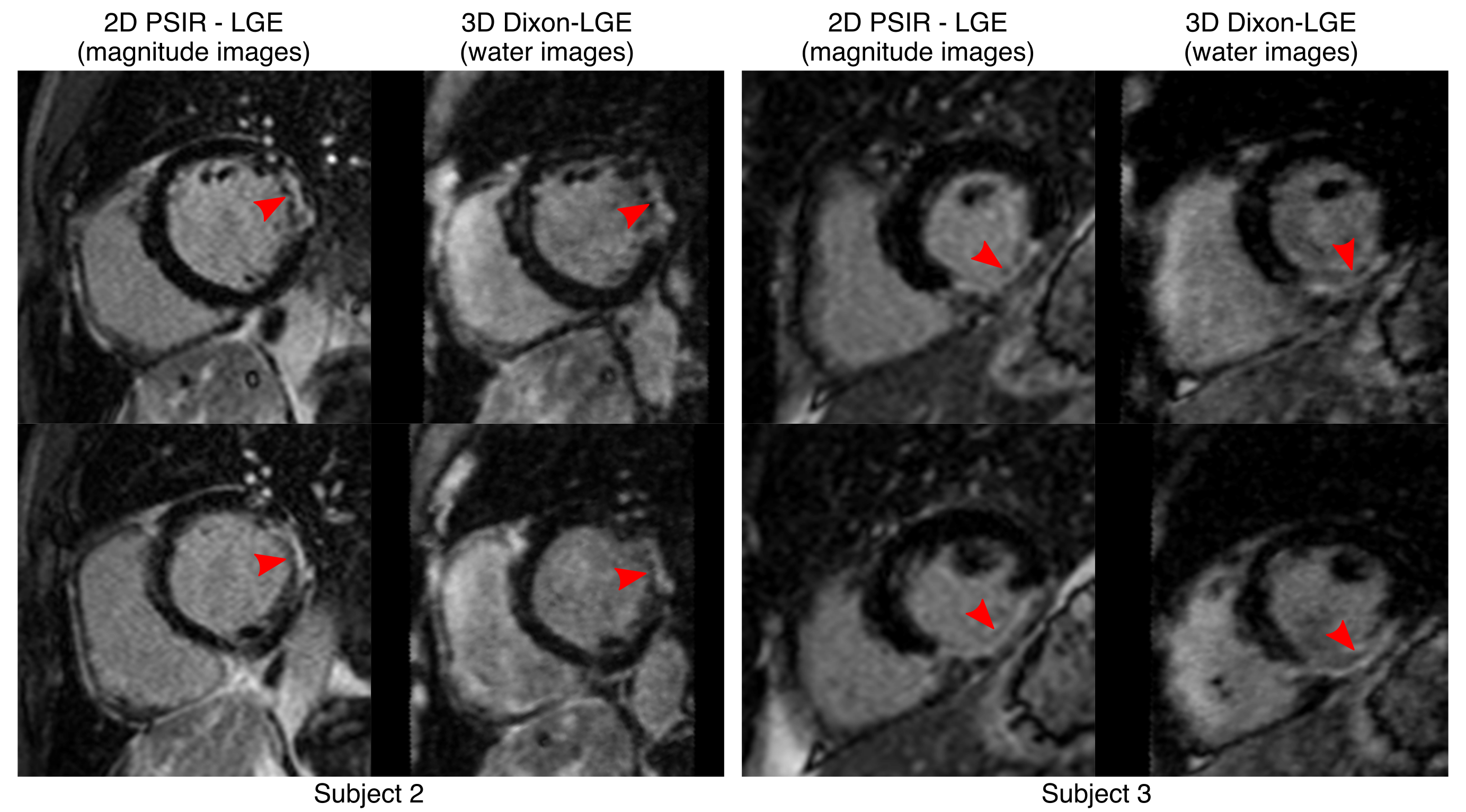
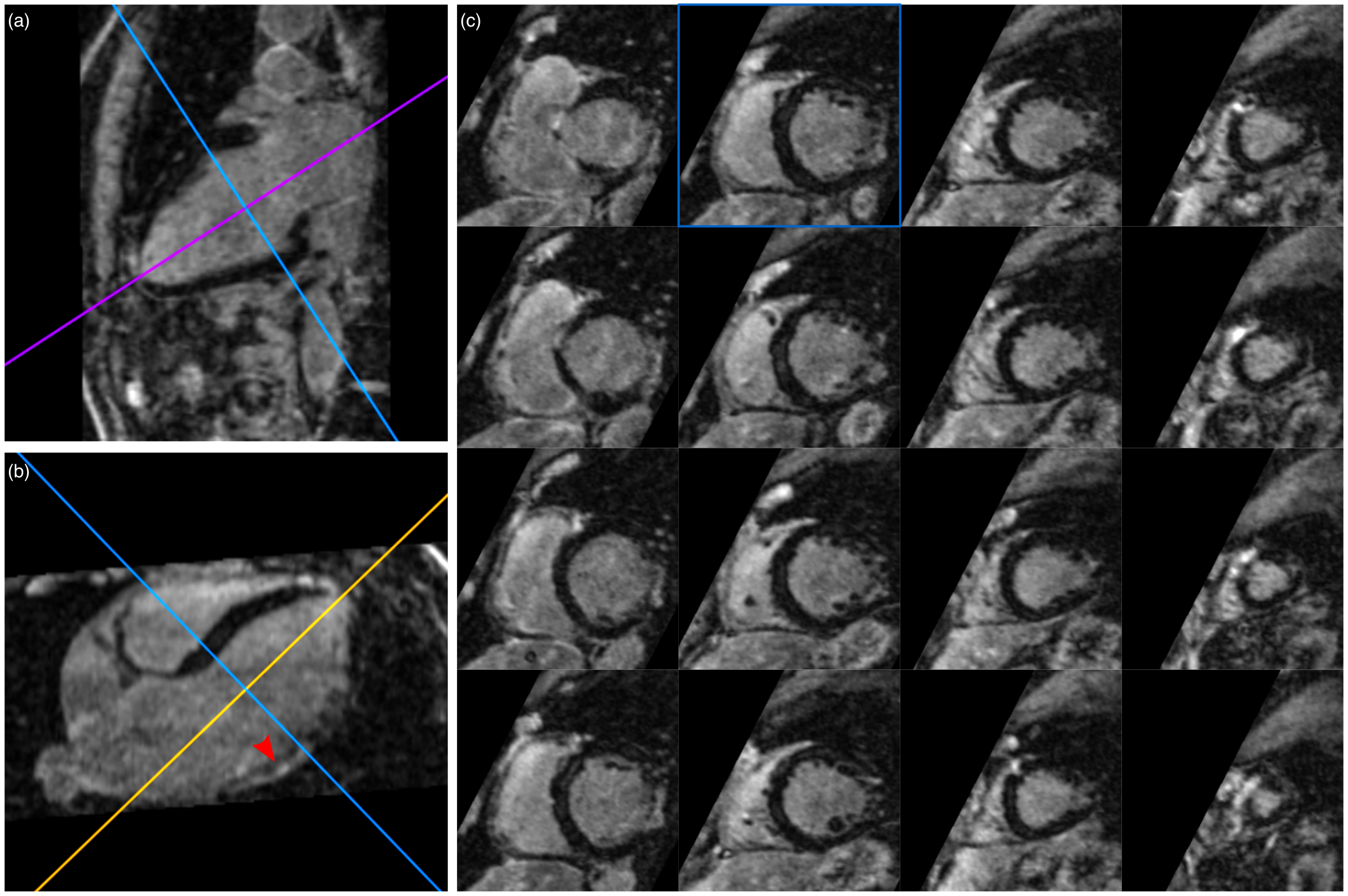
The proposed 3D water/fat LGE acquisition was successfully completed in all subjects, with an average scan time of 7.71±1.76 minutes, acquired 27.2±11.1 minutes after Gd administration. Undersampled motion-compensated reconstruction improves the depiction of anatomical structures in both the water and fat LGE images (Fig2). Despite being acquired after the optimal time point for LGE imaging, water 3D LGE images result in a good depiction of scar, comparable to that of the conventional 2D LGE magnitude images (Fig3), but with higher spatial resolution and whole-heart coverage (Fig4). Furthermore, the proposed approach offers a complementary whole-heart fat image, which could be used to assess fatty infiltration of the myocardium or to quantify epicardial fat (associated with cardiovascular risk) (Fig5).Conclusion
Here we present a novel framework for undersampled respiratory motion-compensated high-resolution 3D whole-heart LGE water/fat imaging. The proposed approach is highly efficient, as it uses all acquired data for image reconstruction, and enables predictable and overall short scan duration of ~8 min, making it suitable for integration into the clinical routine. Compared to conventional LGE imaging, this approach offers improved depiction of scar in the water LGE images, minimising artefacts arising from intra-myocardial fat, and a complementary fat image for assessment of fatty infiltration in the myocardium or quantification of epicardial fat. Future work includes further validation and extending the proposed approach to a 3D water/fat PSIR LGE acquisition and reconstruction scheme.Acknowledgements
This work was supported by EPSRC (EP/L015226/1, EP/P001009, EP/P007619, EP/P032311/1) and Wellcome EPSRC Centre for Medical Engineering (NS/A000049/1).References
1. Kellman P, Arai AE. Cardiac imaging techniques for physicians: Late enhancement. J Magn Reson Imaging 2012;36:529–542
2. Nguyen TD, Spincemaille P, Weinsaft JW, et al. A fast navigator-gated 3D sequence for delayed enhancement MRI of the myocardium: Comparison with breathhold 2D imaging. J Magn Reson Imaging 2008;27:802–808
3. Saranathan M, Rochitte CE, Foo TKF. Fast, three-dimensional free-breathing MR imaging of myocardial infarction: A feasibility study. Magn Reson Med 2004;51:1055–1060
4. Kellman P, Hernando D, Shah S, et al. Multiecho dixon fat and water separation method for detecting fibrofatty infiltration in the myocardium. Magn Reson Med 2009;61:215–221
5. Kellman P, Hernando D, Arai AE. Myocardial Fat Imaging. Curr Cardiovasc Imaging Rep 2010;3:83–91
6. Henningsson M, Koken P, Stehning C, Razavi R, Prieto C, Botnar RM. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med 2012;67:437–445
7. Correia T, Ginami G, Cruz G, et al. Optimized respiratory-resolved motion-compensated 3D Cartesian coronary MR angiography. Magn Reson Med 2018;80:2618–2629
8. Bustin A, Ginami G, Cruz G, et al. Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction. Magn Reson Med 2018 doi: 10.1002/mrm.27354.
Figures