0781
Cardiac Magnetic Resonance Fingerprinting for the Investigation of Suspected Inflammatory Cardiomyopathy1Cardiology, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 2Radiology, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 3Department of Biomedical Engineering, Case School of Engineering, Case Western Reserve University, Cleveland, OH, United States
Synopsis
Inflammatory cardiomyopathy (ICMP) needs to be diagnosed early, and cardiac T1 and T2 mapping both have been shown to increase the accuracy of ICMP diagnosis. Cardiac magnetic resonance fingerprinting (cMRF) can be used to robustly acquire both maps in a single breath-hold, so the goal of this preliminary study was to compare the performance of cMRF and routine parameter mapping in patients with suspected ICMP, including those with implantable cardioverter-defibrillators (ICDs), which often cause significant artifacts. The relaxation times in 24 patients were similar in cMRF and routine mapping, while cMRF may have superior performance in patients with an ICD.
Introduction
Inflammatory cardiomyopathy (ICMP) can be caused by a wide range of local and systemic diseases. Since its consequences can be life-threatening, it needs to be diagnosed early and accurately in order to limit damage to the heart. T1 and T2 relaxation time mapping have been shown to be a useful tool to detect myocarditis in a quantitative and reproducible manner, with T1 mapping having a stronger diagnostic performance in the acute phase, and T2 mapping in the chronic phase[1]. In light of this, T1 and T2 mapping might thus also be of interest for the confirmation of cardiac involvement when it is suspected that local or systemic inflammation has reached the heart and caused ICMP.
Since it might be unknown if a suspected ICMP is acute or chronic, both the T1 and T2 relaxation times are of interest, and should be mapped. This can be done in a single breath-hold with cardiac magnetic resonance fingerprinting (cMRF), which has been shown to be robust to different and varying heart rates and to have high reproducibility[2].
ICMP is furthermore often encountered in patients with implantable cardioverter-defibrillators (ICDs), which often cause significant artifacts in parameter maps and render them non-diagnostic. Given the robustness of cMRF, it would be of interest to evaluate its performance in these patients.
The goal of this preliminary study was therefore to compare the performance of cMRF and routine parameter mapping in patients with suspected ICMP, including those with ICDs.
Methods
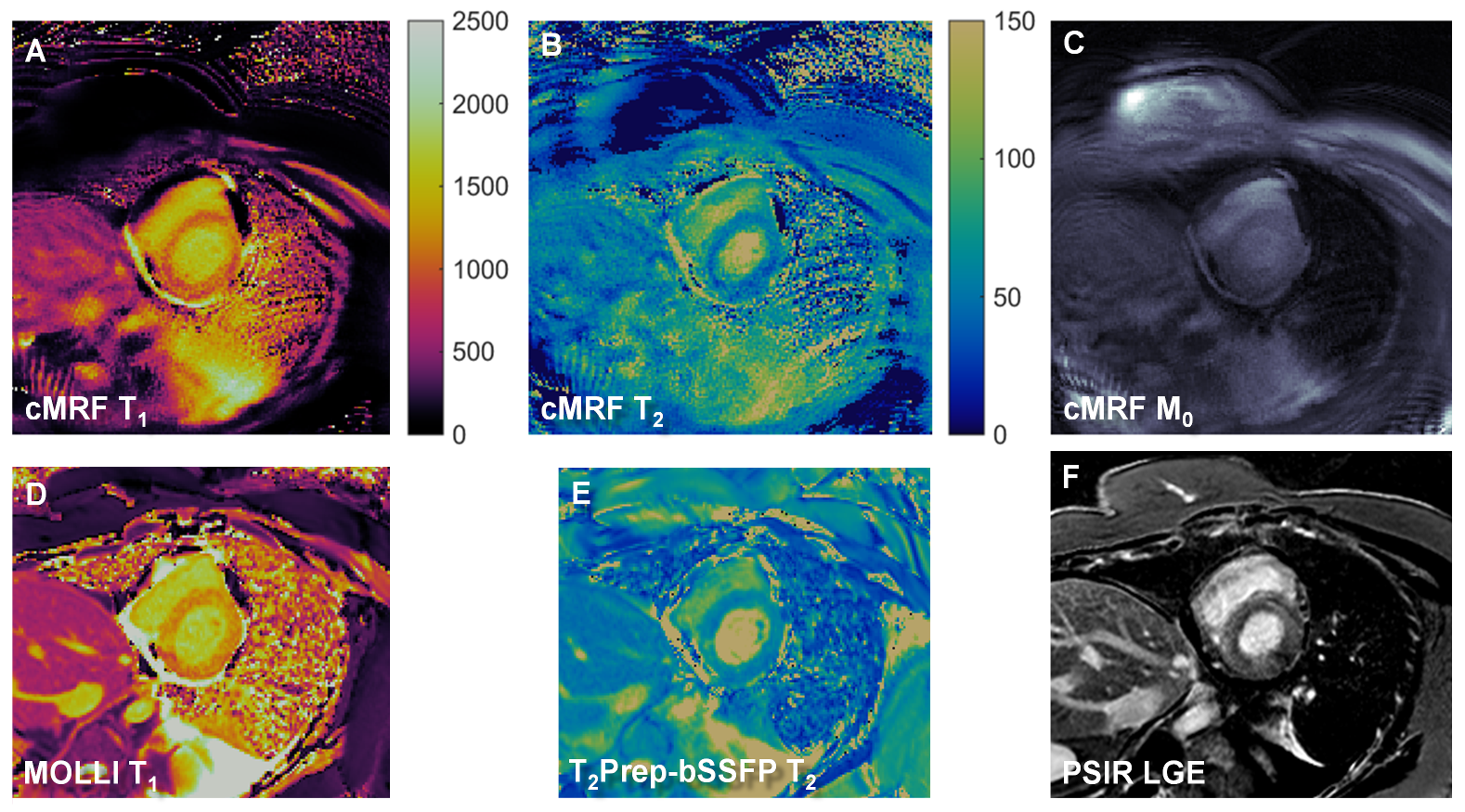
Consecutive patients with suspected ICMP (n=24, of which 4 with an ICD) were prospectively recruited for this IRB-approved study at 1.5T (MAGNETOM Aera, Siemens Healthineers). ECG-triggered cMRF using a 48-fold undersampled spiral readout and a 300x300mm2 FoV was acquired during a single-breath-hold scan of 15 heartbeats, with 50 readouts/heartbeat, flip angles 4-25°, and TR=5.1ms. Five magnetization preparation modules were alternated prior to readout (inversion recovery, No-Prep, TE-T2Prep=30,50,80ms). For each subject, an MRF dictionary was created from the actual trigger times of each acquisition, and direct pattern matching was used to reconstruct T1, T2, and M0 maps[2]. No corrections for slice profile or preparation pulse efficiency were applied. Routine breath-held MOLLI[3] and T2-prepared balanced steady-state free precession (T2prep-bSSFP)[4] as well as late gadolinium enhancement images (LGE) were acquired at the same locations. All techniques were acquired in a basal short-axis slice in each subject, with an additional medioventricular slice being acquired in 10 subjects.
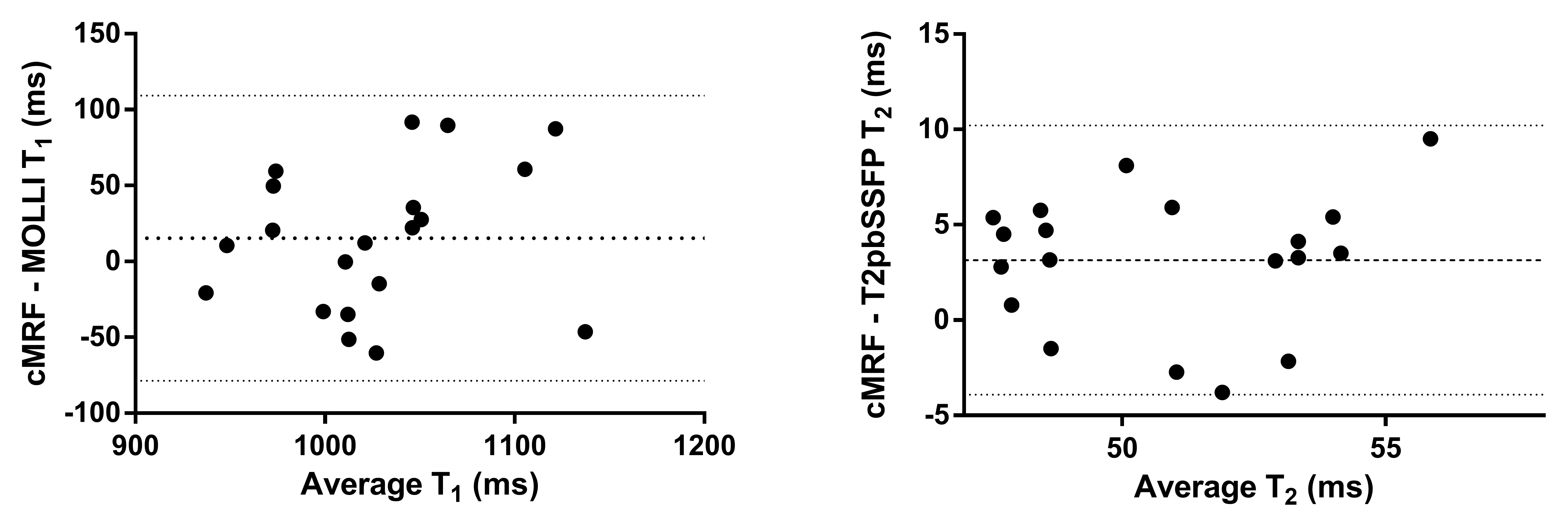
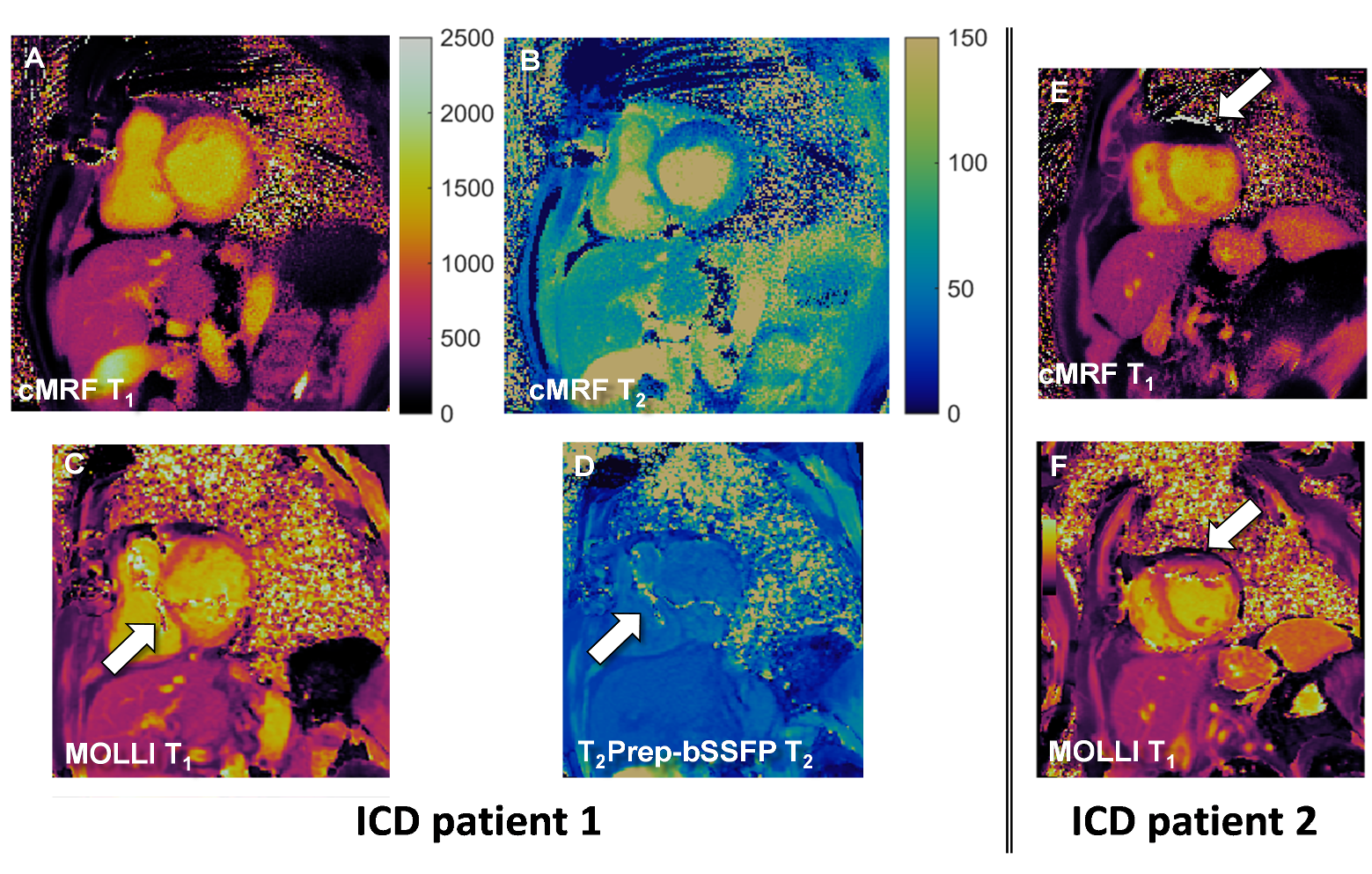
The mean myocardial T1 and T2 values averaged over the acquired slices were calculated for each subject, and a Bland-Altman analysis was performed for all patients without an ICD. In the patients with an ICD, a semi-quantitative score (0=non-diagnostic, 4=sharply defined without apparent artifacts on the LV myocardium) was given to the cMRF and its routine map counterparts. Paired Student’s t-tests were performed to assess significant differences.
Results
cMRF and routine cardiac parameter mapping were acquired in all subjects (Figure 1). The average cMRF values were T1=1028±64ms and T2=52.8±3.8ms, while the average routine values were T1=1019±53ms (p=0.17) and T2=49.3±3.1ms (p=0.001). Significant artifacts affected a single segment of the myocardium in 4 and 6 patients for cMRF and routine mapping, respectively. The Bland-Altman analyses (Figure 2) indicated that cMRF resulted in slightly higher T1 values (bias +15ms, confidence interval ±94ms) as well as T2 values (bias+3.1, confidence interval ±6.9ms), but neither relaxation time had a discernible trend. The 4 patients with ICD had fewer artifacts in the cMRF maps (Figure 3), and higher map quality scores for both T1 (3.0±0.8 vs. 2.3±1.0, p=0.06) and T2 (2.8±1.0 vs. 1.5±1.0, p=0.02).Discussion
In a heterogeneous group of patients with suspected ICMP we demonstrated that cMRF results in similar parameter maps as routine T1 and T2 mapping, but in a single breath-hold. A small but stable T2 bias was observed versus routine mapping, which should not affect diagnostics, but warrants proper reference values for cMRF. The encouraging high cMRF map quality in the small group of patients with an ICD illustrates the robustness of cMRF. This preliminary study thus demonstrates the potential of cMRF to play an important role in the increasingly frequent requests for the diagnosis of ICMP.Acknowledgements
This work was supported by grants from the Swiss Heart Foundation and the Swiss National Science Foundation (#PZ00P3-154719 and #32003B-182615).References
1. P Lurz et al. J Am Coll Cardiol. 2016;67(15):1800-1811. doi: 10.1016/j.jacc.2016.02.013.
2. JI Hamilton et al. Magn Reson Med. 2017;77(4):1446-1458. doi: 10.1002/mrm.26216
3. DR Messroghli et al. Magn Reson Med. 2004;52(1):141-6. doi: 10.1002/mrm.20110
4. S Giri et al. J Cardiovasc Magn Reson. 2009;11:56. doi: 10.1186/1532-429X-11-56.
5. AJ Coristine et al. Proc Int Soc Magn Reson Med 2017
Figures