0756
SmartPulse, a Machine Learning Approach for Calibration-Free Dynamic RF Shimming in Body Imaging1NeuroSpin, CEA, Université Paris-Saclay, Gif-sur-Yvette, France, 2Parietal, Inria, Université Paris-Saclay, Gif-sur-Yvette, France, 3Siemens Heathcare SAS, Saint-Denis, France, 4Department of Radiology, AP-HP, CHU Henri Mondor, Créteil, France, 5Université Paris-Est Créteil Val-de-Marne, Créteil, France, 6INSERM Unité U955, Equipe 18, Créteil, France
Synopsis
At high field, tailored static or, better, dynamic RF shimming can be used to reduce artifacts due to transmit B1 field inhomogeneity, but those methods require extra time for calibration, which can disrupt clinical workflows. Recently, universal pulses (UP) were introduced in brain imaging to get rid of calibration. In this work, a machine learning method is proposed to extend universal pulse kT-point design to body imaging where inter-subject variability is more pronounced, by classifying subjects into one of several predefined categories. This method outperforms UP design, and yields images similar to those obtained with state-of-the-art tailored design.
Introduction
High field MRI provides a higher signal-to-noise ratio that can be beneficial to reach finer spatial resolution, but the shorter associated radiofrequency (RF) wavelength often leads to “B1+ artifacts” in large organs.1-3 To reduce them, static RF shimming makes use of parallel transmission4 (pTx) to adjust RF complex weights on each available transmit channel. Thus, in clinical routine, the user can usually choose between a “standard” RF shimming with predefined weights,5,6 and a “tailored” one relying on measurements of B1+ fields for each patient. Dynamic RF shimming, such as with tailored kT-points7 for non-selective excitation, reduces inhomogeneity even further.8-10 To overcome extra scan times necessary to calibrate B1+ in all tailored techniques (mapping, pulse design), universal pulses11 (UP) were proposed for neuroimaging as a plug-and-play dynamic RF shimming solution. Unfortunately, this may not perform as well in body imaging due to the more pronounced inter-subject variability of B1+ in that case. Here, a trade-off between tailored and UP designs is achieved with the machine-learning-based SmartPulse technique, which provides calibration-free dynamic RF shimming adapted to population subsets. This method is applied and evaluated with “smart” kT-points in routine abdominal imaging on a dual-transmit MAGNETOM Skyra 3T scanner (Siemens Healthcare GmbH, Erlangen, Germany) equipped with two-channel pTx.Theory and Methods
The SmartPulse process consists in (i) dividing a database of subjects whose RF field distributions are known into clusters of similar subjects and design one UP for each cluster, and (ii) using a set of simple features to classify subjects into the most fitting cluster, thus attributing them the best possible precomputed pulse (lowest inhomogeneity), without resorting to additional calibration.
A database of B1+ and off-resonance abdominal maps of Nprev = 50 subjects from a previous study9 was first divided into three clusters based on mutual affinity between their respective tailored kT-points pulses as shown in Figure 1. For each cluster, a 5-kT-point pulse was computed, minimizing normalized root-mean-square error (NRMSE) from an 11° flip angle (FA) target simultaneously for all subjects comprised in it.11 B1+ field maps were obtained from the manufacturer standard adjustment procedure used for patient-specific static RF shimming, along with the virtual observation points12 needed for specific absorption rate calculation. Off-resonance maps were measured with a two-echo GRE breath-hold acquisition (ΔTE= 0.95ms).
Using Nadd = 30 additional subjects’ field distributions, a classifier was trained on this database of Ntrain = 80 labelled subjects to recognize the best pulse from the three ones available, relying only on patient features (Figure 2) accessible from the preliminary localizer sequence common to all protocols. Classification was implemented using Scikit-learn13 and consisted in an extremely randomized trees algorithm14 and a nonlinear support vector machine multiclass classifier15,16 joined by Scikit-learn’s “soft” vote.
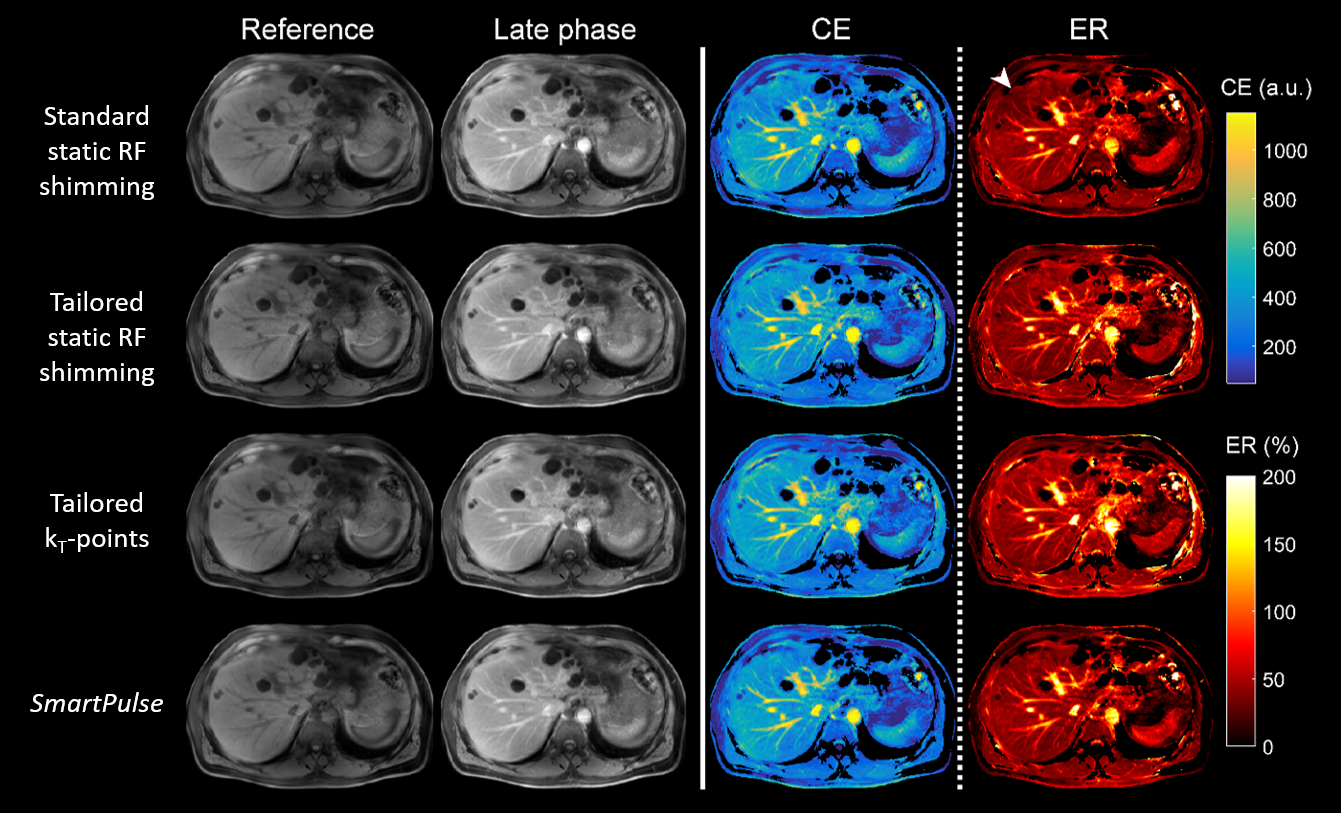
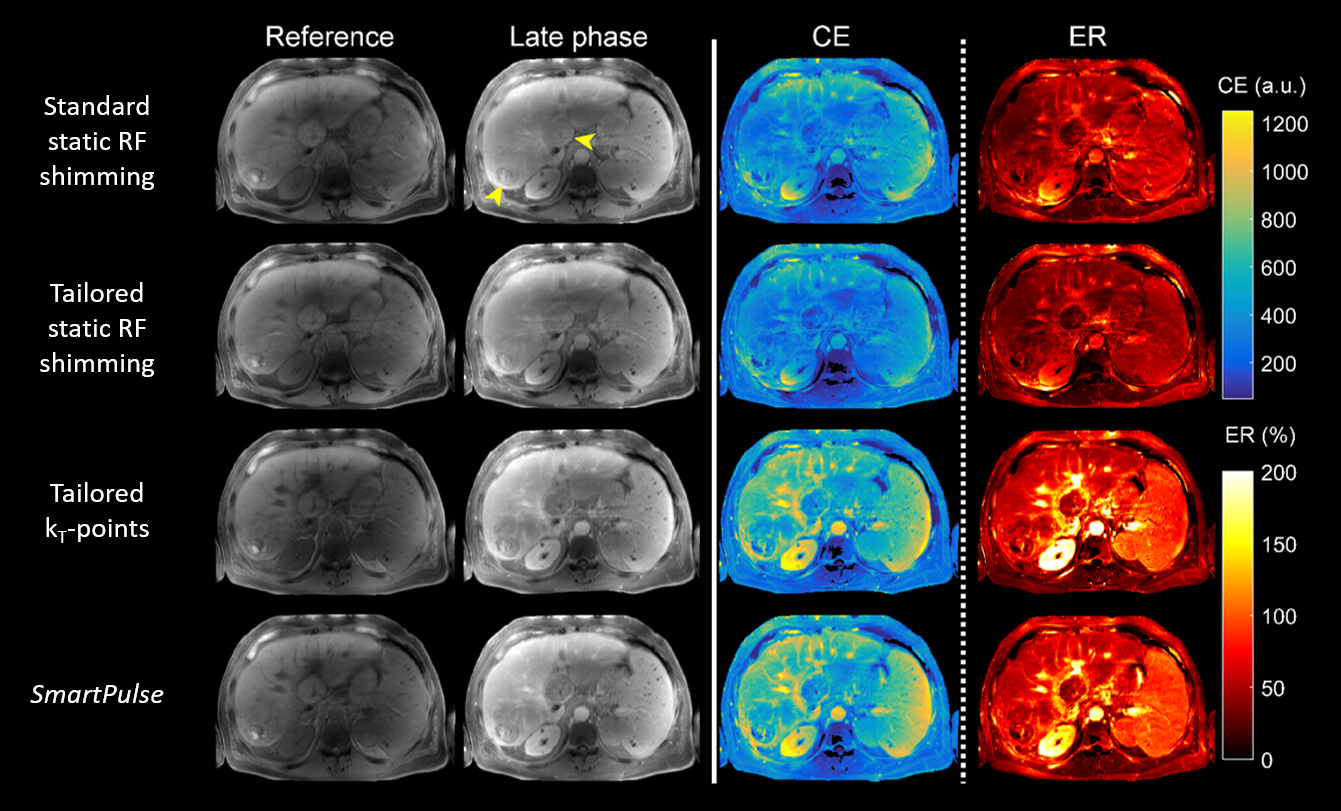
The method was tested on an additional set of Ntest = 53 subjects and compared with four strategies: (1) vendor’s standard “TrueForm” calibration-free static RF shimming, (2) vendor’s tailored static RF shimming, (3) tailored and (4) universal kT-points pulses. The assessment was based on measured field maps and Bloch equation simulations to yield FA-NRMSE across all subjects. The UP was calculated on the database used for clustering (Nprev), and tailored kT-points were computed as done in a previous study.9 Finally, 23 subjects from the test population underwent 3D breath-hold Dynamic Contrast-Enhanced MRI – compatible with non-selective excitation – while a pulse designer was present. SmartPulse could be compared to strategies (1), (2) and (3) by repeating the acquisition with each transmit scheme before injection and in the late phase with the same sequence parameters: FA= 11°, TE/TR= 3/6 ms, 320×220×72 matrix, 1.2×1.2×3.5 mm3 resolution, GRAPPA factor 2, 80%/50% phase/slice resolution, partial-Fourier factor of 6/8, 505 Hz/pixel bandwidth, "quick" fat saturation.17 Contrast enhancement (CE) and enhancement ratio (ER) images were computed as: $$$\small\mathsf{CE} = \mathsf{S_{late}} - \mathsf{S_{ref}}$$$ and $$$\small\mathsf{ER} = \frac{\mathsf{CE}}{\mathsf{S_{ref}}}$$$, where Sref and Slate represent signal before and after injection.Results and Discussion
The
proportion of test subjects who were assigned the pulse yielding minimal NRMSE,
within a 2% tolerance margin, was 81%. As shown in Figure 3, SmartPulse outperformed all
calibration-free approaches and vendor’s tailored static RF shimming, and could
be improved with better classification. Although FA homogeneity was
systematically better with tailored kT-points, the difference was
barely noticeable on in-vivo images (Figures 4 and 5).
With no need for on-line field mapping nor pulse design, SmartPulse can fit
seamlessly into a clinical protocol and is able to restore sufficient
excitation uniformity where standard or tailored static RF shimming
occasionally fail. With more than 50 tests on patients, the soundness and
robustness of this machine-learning-based approach has been shown.Acknowledgements
This work is dedicated to the memory of Professor Alain Rahmouni, who passed away on January 26th 2018. Major figure of French radiology, internationally respected, Professor Rahmouni developed an advanced MR teaching and research program at CHU Henri Mondor imaging department. Bridging early technological innovations in MR to clinical practice was always his ambition. This research study is one of the many projects he supported in this field. Professor Alain Rahmouni will be remembered by all the authors of this abstract, and many more.
The authors wish to thank all the MRI technicians of Henri Mondor Hospital for their patience and understanding, as well as Lisa Leroi and Gaël Saib for their help in coining a name for the proposed method.
This project was funded by CEA’s Programme Transversal, Technologies pour la Santé (Transversal Programme for Health Technologies).
References
1. Bernstein MA, Huston J, Ward HA. Imaging artifacts at 3.0T. J Magn Reson Imaging. 2006 Oct 1;24(4):735–46.
2. Padormo F, Beqiri A, Hajnal JV, Malik SJ. Parallel transmission for ultrahigh-field imaging. NMR Biomed. 2016 Sep 1;29(9):1145–61.
3. Kukuk GM, Gieseke J, Nelles M, König R, Andersson M, Muschler E, et al. Clinical liver MRI at 3.0 Tesla using parallel RF transmission with patient-adaptive B1 shimming. In: Proc Intl Soc Mag Reson Med [Internet]. 2009 [cited 2016 Oct 4]. p. 119. Available from: http://cds.ismrm.org/protected/09MProceedings/files/00119.pdf
4. Katscher U, Börnert P, Leussler C, van den Brink JS. Transmit SENSE. Magn Reson Med. 2003 Jan;49(1):144–50.
5. Nistler J, Renz W. Method for controlling a magnetic resonance system [Internet]. US7847554 B2, 2010 [cited 2016 Nov 4]. Available from: http://www.google.ch/patents/US7847554
6. Geppert C, Nistler J, Renz W, Panagiotelis I, Speckner T. Reduced B1-inhomogeneities in breast MRI using optimized RF excitation. In: Proc ISMRM. 2008.
7. Amadon A, Cloos MA. Method and apparatus for compensating for B1 inhomogeneity in magnetic resonance imaging by nonselective tailored RF pulses. WO2011/128847A1, 2011.
8. Cloos MA, Boulant N, Luong M, Ferrand G, Giacomini E, Le Bihan D, et al. kT-points: Short three-dimensional tailored RF pulses for flip-angle homogenization over an extended volume. Magn Reson Med. 2012 Jan;67(1):72–80.
9. Tomi-Tricot R, Gras V, Mauconduit F, Legou F, Boulant N, Gebhardt M, et al. B1 artifact reduction in abdominal DCE-MRI using kT-points: First clinical assessment of dynamic RF shimming at 3T. J Magn Reson Imaging. 2018 Jun;47(6):1562–71.
10. Gras V, Luong M, Amadon A, Boulant N. Joint design of kT-points trajectories and RF pulses under explicit SAR and power constraints in the large flip angle regime. J Magn Reson. 2015 Dec;261:181–9.
11. Gras V, Vignaud A, Amadon A, Bihan DL, Boulant N. Universal pulses: A new concept for calibration-free parallel transmission. Magn Reson Med. 2017 Feb 1;77(2):635–43.
12. Eichfelder G, Gebhardt M. Local specific absorption rate control for parallel transmission by virtual observation points. Magn Reson Med. 2011 Nov 1;66(5):1468–76.
13. Pedregosa F, Varoquaux G, Gramfort A, Michel V, Thirion B, Grisel O, et al. Scikit-learn: Machine learning in Python. J Mach Learn Res. 2011;12(Oct):2825–2830.
14. Geurts P, Ernst D, Wehenkel L. Extremely randomized trees. Mach Learn. 2006 Apr 1;63(1):3–42.
15. Cortes C, Vapnik V. Support-vector networks. Mach Learn. 1995 Sep 1;20(3):273–97.
16. Wu T-F, Lin C-J, Weng RC. Probability estimates for multi-class classification by pairwise coupling. J Mach Learn Res. 2004;5(Aug):975–1005.
17. Le Y, Kroeker R, Kipfer HD, Lin C. Development and evaluation of TWIST Dixon for dynamic contrast-enhanced (DCE) MRI with improved acquisition efficiency and fat suppression. J Magn Reson Imaging. 2012 Aug 1;36(2):483–91.
Figures
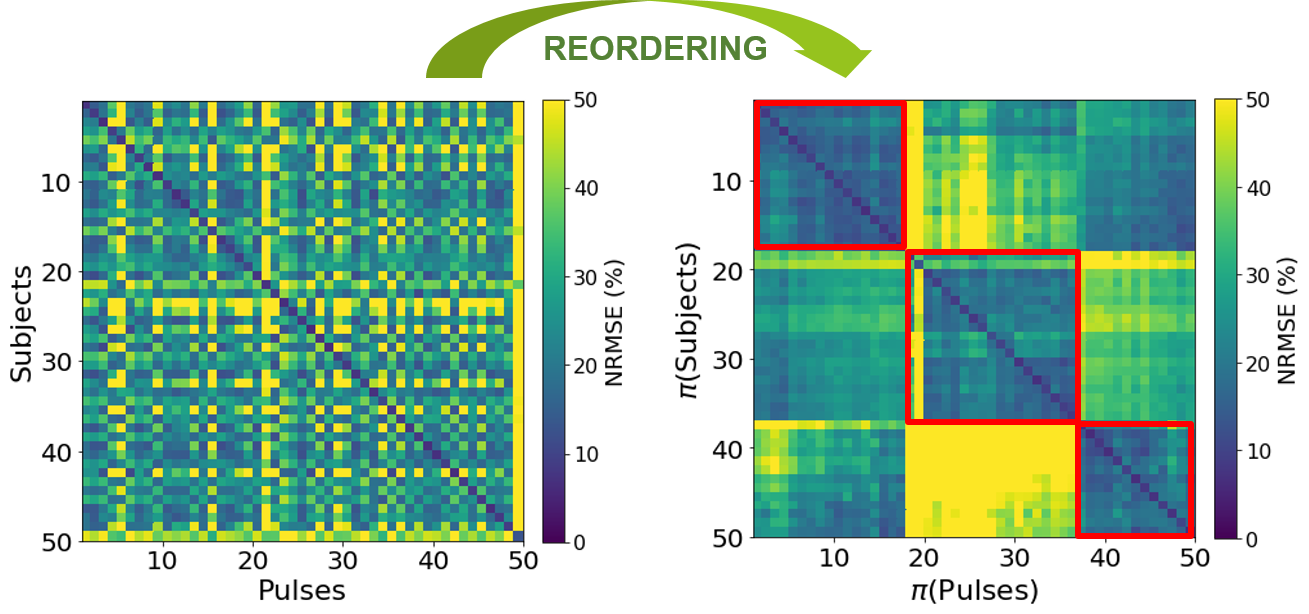
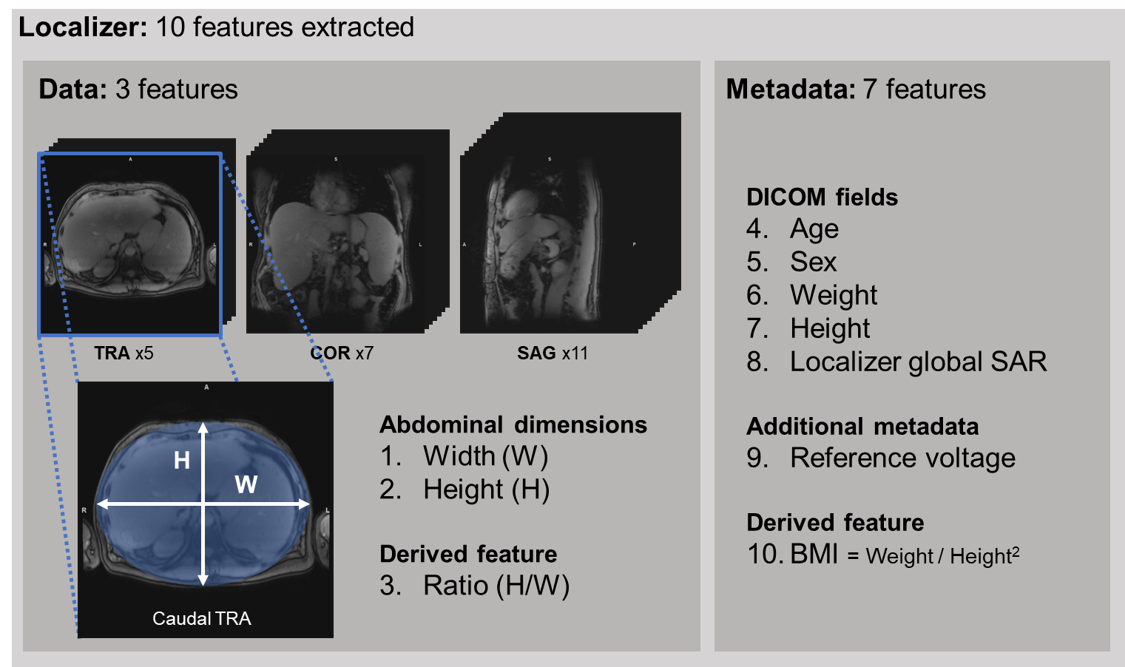
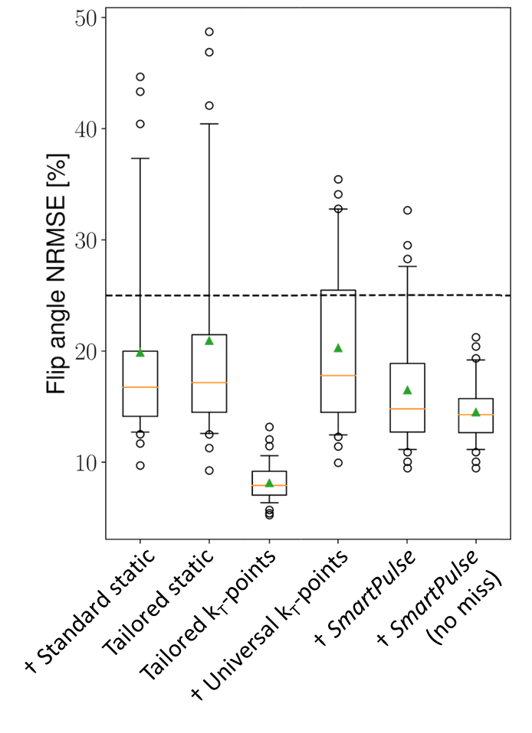
Figure 3. Distribution of flip angle NRMSE obtained on Ntest = 53 test subjects, with various pulses. The dashed line corresponds to a 25% standard static shimming NRMSE threshold between “standard” (Figure 4) and “difficult” (Figure 5) subjects.
With 93% of subjects brought below 25% NRMSE, SmartPulse outperforms other calibration-free techniques (indicated by “†”): standard static (79%) and universal kT-points (72%). With a perfect classifier (no miss), all subjects would have a NRMSE between 9% and 21%.
Green triangle= mean value; orange line= median; box edges= 25th (Q1) and 75th (Q3) percentiles; whiskers= 5th and 95th percentiles; circles= outliers.