0744
Highly Accelerated Dynamic 2D and 3D Vessel-Encoded Arterial Spin Labelling Angiography1Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom
Synopsis
Vessel-encoded ASL can produce vessel-selective cerebral angiograms, but to separate blood from multiple arteries more images are needed than for standard ASL angiography, which increases scan time. Angiograms are however well suited for under-sampling and compressed sensing reconstruction because of their high intrinsic sparsity. In this work we demonstrate in-vivo that vessel-selective angiograms allow for higher acceleration factors, yielding comparable image quality to conventional angiography with matched scan time using 2D and 3D time-resolved golden angle radial acquisitions. With this optimised acquisition and reconstruction method, scan time of the 3D case can be reduced from 8:35 hours to ~5 minutes.
Introduction
Arterial spin labelling (ASL) angiography is a non-invasive method for obtaining information about cerebral blood supply1,2. Unlike other angiographic methods, an ASL preparation can be used to create angiograms that show artery specific blood supply. Vessel-encoded (VE) ASL does this in an SNR efficient way3. However, compared with standard ASL, which only requires a single pair of ‘tag’ and ‘control’ images, VE-ASL requires N+1 images, where N is the number of encoded arteries, thus increasing scan time.
Vessel-encoding increases sparsity in angiograms by separating voxels with non-zero intensity across multiple vessel-specific images. Simulations4,5 have shown that compressed sensing (CS)6,7 reconstructions allow higher acceleration (R factors) for VE than non-VE angiograms because of this increased sparsity. In this work we aim to demonstrate this benefit in-vivo, and present a method for acquisition of dynamic VE-ASL angiograms using both 2D and 3D golden angle radial schemes.
Methods
The proposed pulse sequence (figure 1) included a pre-saturation module followed by a 1.0 s vessel-encoded pseudo-continuous ASL pulse train8,9. The right and left internal carotid arteries (RICA, LICA) and the basilar artery (BA) were encoded with a 4-cycle Hadamard encoding3. Following each ASL preparation, data were immediately acquired using either a single slab 2D (50 mm thick) or full 3D spoiled gradient echo radial golden angle readout lasting 1.3 s. After each preparation module 108 spokes in k-space were acquired and these were spread across 12 frames in 2D and 6 in 3D, giving temporal resolutions of 105 ms and 209 ms, respectively. Key imaging parameters were: TE/TR = 5.9/11.6 ms, FA = 7°, voxel size = 1.1 mm in-plane (2D), 1.1 mm isotropic (3D), scan time = 5:26 minutes (2D, fully sampled) and 22:14 minutes (3D, R = 23). A fully Nyquist sampled 3D acquisition would take 8:35 hours (requiring 57,906 spokes per frame for each vessel-encoding cycle).
An iterative reconstruction algorithm (FISTA)10, was used to reconstruct the data in a CS framework using a non-uniform fast Fourier transform11 and coil sensitivity profiles estimated using an adaptive combine approach12. The regularisation factor, 𝜆, was set to optimally weight image sparsity (in the x-t domain) against data consistency.
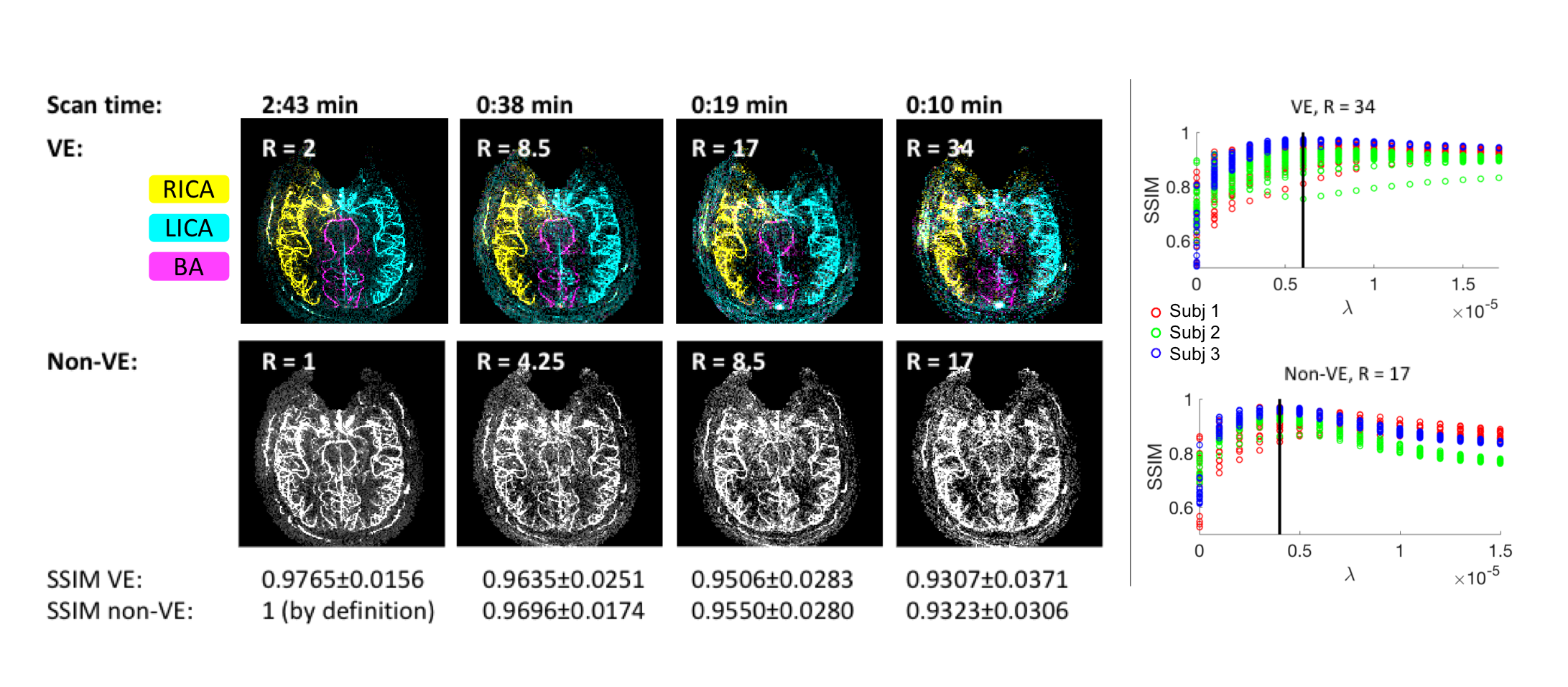
Imaging was performed on a 3T scanner (Magnetom Verio, Siemens, Erlangen, Germany) on three volunteers (1 F, mean age: 29) in 2D, and on one (M, 27) in 3D. Data with a range of acceleration factors were created using subsets of all acquired spokes. For an acceleration factor R, the data was split into R independent subsets. In 2D, the fully sampled data was used as ground truth and the reconstructions were compared with it using a structural similarity index (SSIM)13 that correlates well with perceptual image quality. SSIM ranges from 0 to 1 and was Fisher transformed to make the underlying distribution more Gaussian for significance testing using a t-test. Non-VE scans were also acquired for the 2D case for time-matched comparison. As no ground truth was available for the 3D case, it was assessed qualitatively.
Results
Both VE and non-VE 2D dynamic angiograms were reconstructed with high SSIM, even at high under-sampling factors. The optimal regularisation factor did not vary considerably across subjects (Figure 2).
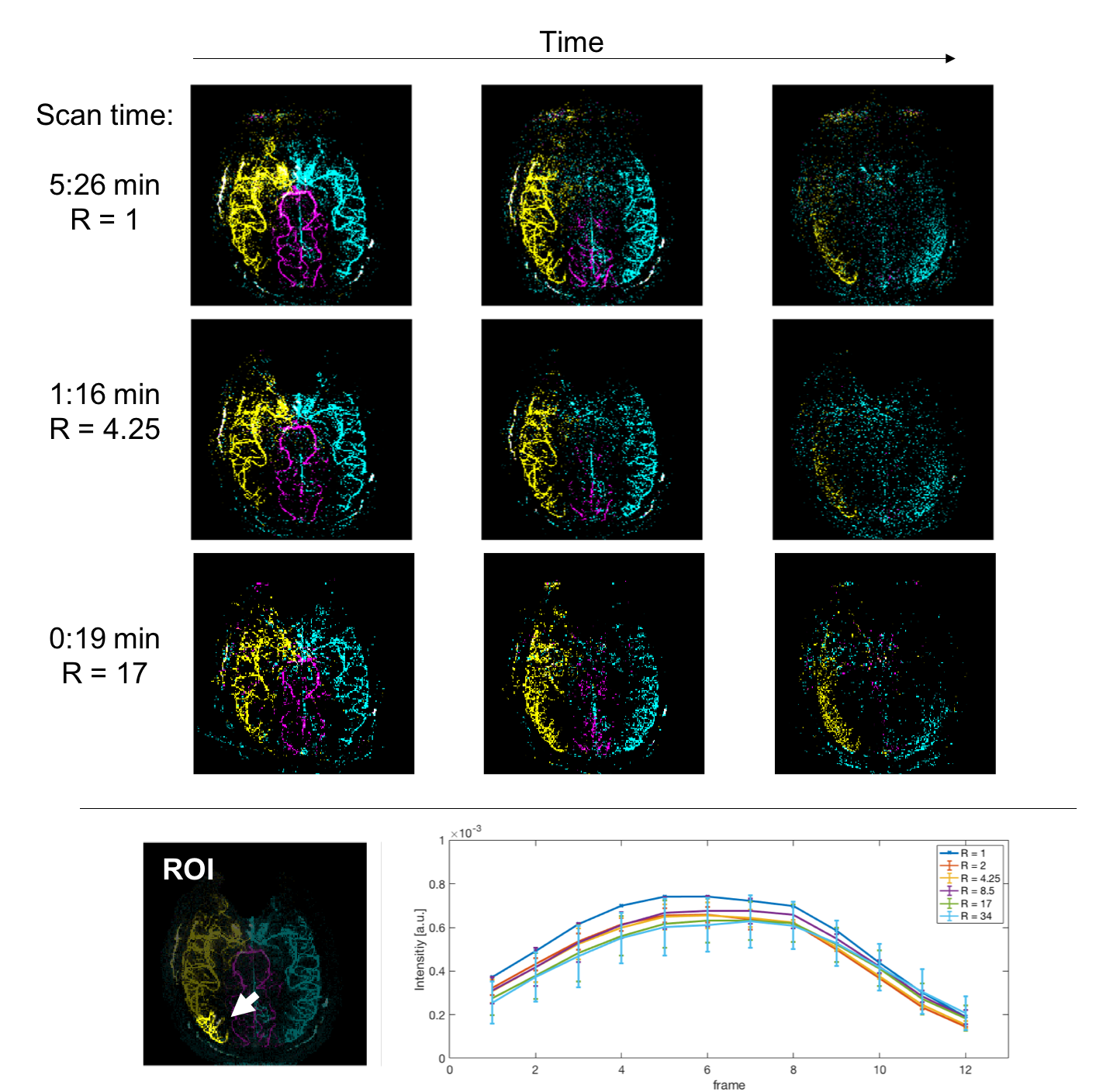
Dynamic features were also well preserved across under-sampling factors. Figure 3 shows an example subject and how the vessel intensity is preserved at high acceleration factors.
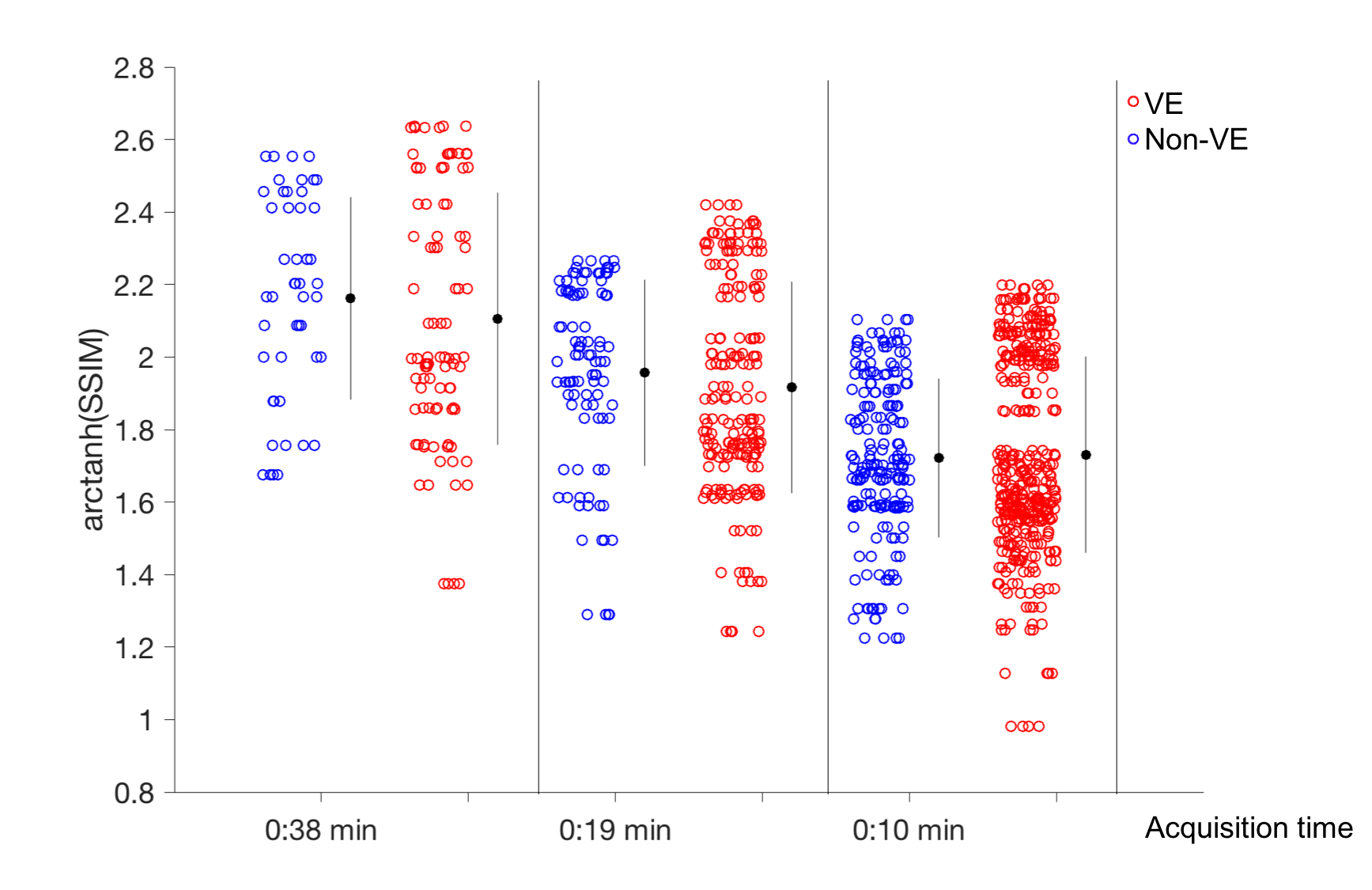
There was no significant difference between the reconstruction quality of VE images and non-VE images acquired with the same scan time, but the VE-data had a higher variability than the non-VE data (figure 4).
In 3D, detailed angiograms were reconstructed from as little as 5 minutes of acquisition, R= 97 (Figure 5).
Discussion
There was no significant difference in image quality between VE and non-VE at matched scan times, indicating that vessel-selective information can be obtained essentially for free. The higher variability of the VE data could be explained by increased sensitivity to motion, because the images are constructed from four acquisitions rather than two.
The 3D results show that with a ~5-minute scan, high resolution whole-brain VE-ASL angiography can become a feasible alternative to time-of-flight angiography, providing dynamic and vessel-specific information with complete background suppression.
To improve the reconstruction further, constraints in the temporal domain (such as enforcing temporal smoothness) will be explored. Furthermore, the competing effects of sparsity and SNR on CS reconstruction will be characterised.
Conclusion
In 2D we have demonstrated in-vivo image quality comparable to non-VE angiograms at matched scan time, and in 3D, high quality angiograms were achieved, reducing scan time from a theoretical 8:35 hours to ~5 minutes.Acknowledgements
This work was funded by EPSRC and the Royal Academy of Engineering. The Wellcome Centre for Integrative Neuroimaging is supported by core funding from the Wellcome Trust (203139/Z/16/Z).References
1. Dixon W.T., Du L.N., Faul D.D., Gado M., Rossnick S., 1986. Projection angiograms of blood labeled by adiabatic fast passage. Magn Reson Med 3,454–462.
2. Nishimura DG, Macovski A, Pauly JM, Conolly SM., 1987. MR angiography by selective inversion recovery. Magn Reson Med 4,193–202.
3. Wong, E. C. 2007. Vessel-encoded arterial spin-labeling using pseudocontinuous tagging. Magn Reson Med 58,1086–1091.
4. Schauman S.S., Chiew M., Okell T.W., 2018, Vessel-encoding improves compressed sensing reconstruction of arterial spin labelling angiograms. Presented at the British Chapter of ISMRM Post-Graduate Symposium 2018.
5. Schauman, S.S., Chiew, M., Okell, T.W., 2018. Accelerated Acquisition of Vessel-Encoded Arterial Spin Labelling Angiograms with Compressed Sensing. Presented at the Joint Annual Meeting ISMRM-ESMRMB 2018.
6. Candès, E.J., Romberg, J.K., Tao, T., 2006. Stable signal recovery from incomplete and inaccurate measurements. Communications on Pure and Applied Mathematics 59, 1207–1223.
7. Donoho, D.L., 2006. Compressed sensing. IEEE Transactions on Information Theory 52, 1289–1306.
8. Okell, T.W., Chappell, M.A., Woolrich, M.W., Günther, M., Feinberg, D.A., Jezzard, P., 2010. Vessel-encoded dynamic magnetic resonance angiography using arterial spin labeling. Magn Reson Med 64, 430–438.
9. Okell, T.W., 2018. Combined angiography and perfusion using radial imaging and arterial spin labeling. Magn Reson Med
10. Beck, A., Teboulle, M., 2009. A Fast Iterative Shrinkage-Thresholding Algorithm for Linear Inverse Problems. SIAM J. Imaging Sci. 2, 183–202.
11. Fessler, J.A., Sutton, B.P., 2003. Nonuniform fast Fourier transforms using min-max interpolation. IEEE Transactions on Signal Processing 51, 560–574.
12. Walsh, D.O., Gmitro, A.F., Marcellin, M.W., 2000. Adaptive reconstruction of phased array MR imagery. Magn Reson Med 43, 682–690.
13. Wang, Z., Bovik, A.C., Sheikh, H.R., Simoncelli, E.P., 2004. Image Quality Assessment: From Error Visibility to Structural Similarity. IEEE Transactions on Image Processing 13, 600–612.
Figures