0743
Comparison of Four 3D Black Blood MRI Sequences for the Characterization of Unruptured Intracranial Aneurysm Wall Enhancement1Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 2Radiology, Changhai Hospital, Shanghai, China
Synopsis
Aneurysm wall enhancement (AWE) post Gadolinium contrast on high-resolution black blood MRI has been studied as a marker of unstable intracranial aneurysms. However, a recent study showed slow flow could mimic AWE. This study evaluated four black blood sequences with high- and low-resolution fast-spin-echo (SPACE), with and without MSDE/DANTE blood suppression modules. In 30 unruptured saccular aneurysms, we found low-resolution SPACE significantly overestimated AWE (20/30 enhanced) compared to high-resolution SPACE (16 enhanced) and sequences with MSDE/DANTE (14 and 13 enhanced). High-resolution DANTE-SPACE has the best blood suppression and image quality, which is a preferred method for AWE assessment.
Purpose
Aneurysm wall enhancement (AWE) post Gadolinium contrast on high-resolution black blood MRI has been studied as a marker of unstable intracranial aneurysms 1. Identifying aneurysm with and without AWE has the potential to improve patient management. For example, a longer follow up interval can be chosen for stable aneurysms (non-AWE), and smaller but high-risk aneurysms (with AWE) could be selected for early intervention. However, a recent study showed slow flow could mimic AWE2. Thus, there is an urgent need to standardize sequences for AWE characterization. We aim to compare four black blood sequences with high and low resolution, with and without MSDE3/DANTE4 advanced blood suppression, in order to determine an optimized sequence for AWE assessment.Methods
Study Population: 25 patients (12 male, mean age 58±12 years) with 30 unruptured saccular aneurysms were recruited. All patients underwent 3T MRI pre- and post-Gd contrast injection. Sequences: Pre-contrast 3D black-blood fast-spin-echo MRI (SPACE5) was first performed: whole brain coverage, TR/TE 1000ms/10ms, echo train length 60, 0.6mm isotropic resolution, scan time 8 minutes. Following contrast-enhanced MRA, four sequences were performed sequentially. 1) post contrast high-resolution SPACE, similar to pre. 2) MSDE-SPACE, similar scanning parameters as (1) except an additional MSDE blood suppression module (preparation time 15ms, first order moment of 500mT*ms2/m). 3) DANTE-SPACE, similar parameters as (1) except an additional DANTE blood suppression module (100 pulses, 1ms gap, flip angle 10). 4) low resolution SPACE, similar TR/TE, echo train and coverage with (1) and resolution reduced to 0.9mm isotropic. Scan time 4 minutes. Image analysis: AWE was assigned if the wall signal was equal to or greater than that of the pituitary infundibulum. Pattern of enhancement was characterized as eccentric or concentric. A previous developed enhancement score6 was also used (0-5, higher score means larger area of enhancement). Image quality score (1-4) was given as previously described7. The lumen area and signal was measured at the middle slice of the aneurysm. Lumen contrast ratio (CR) was defined as lumen signal over adjacent gray matter signal, in order to quantify blood suppression efficiency.Results
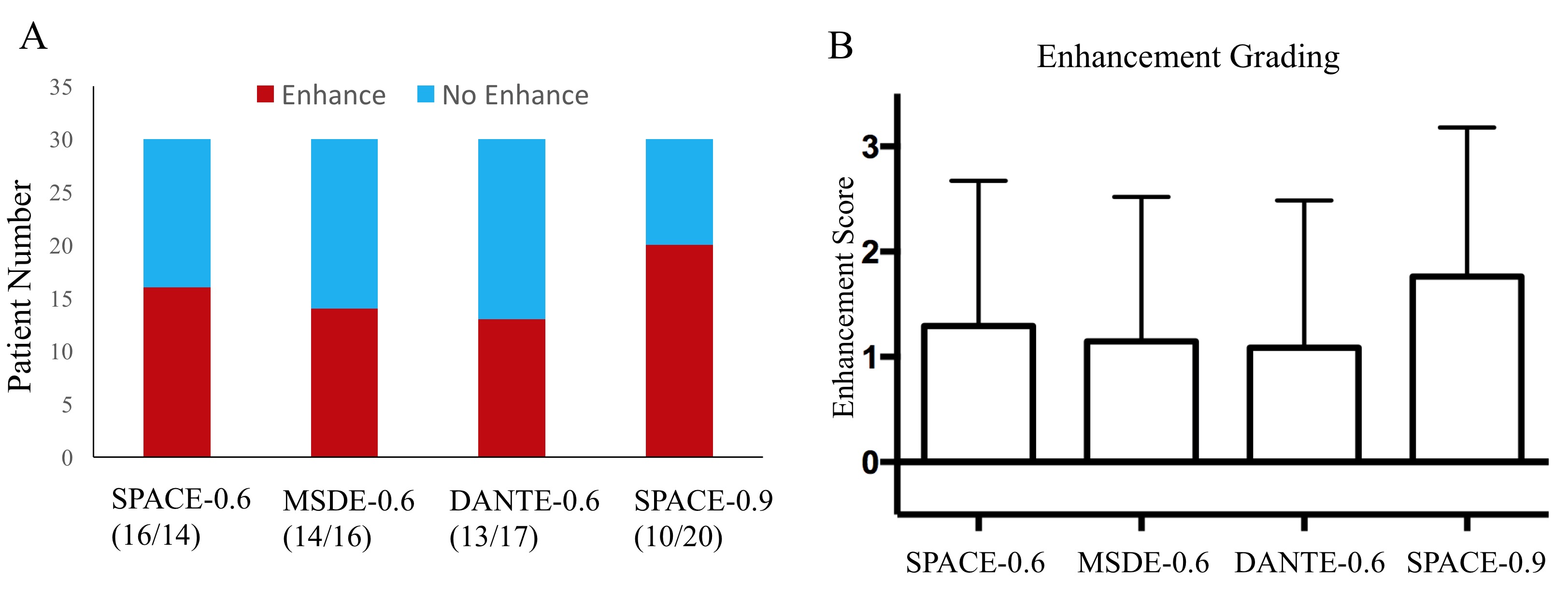
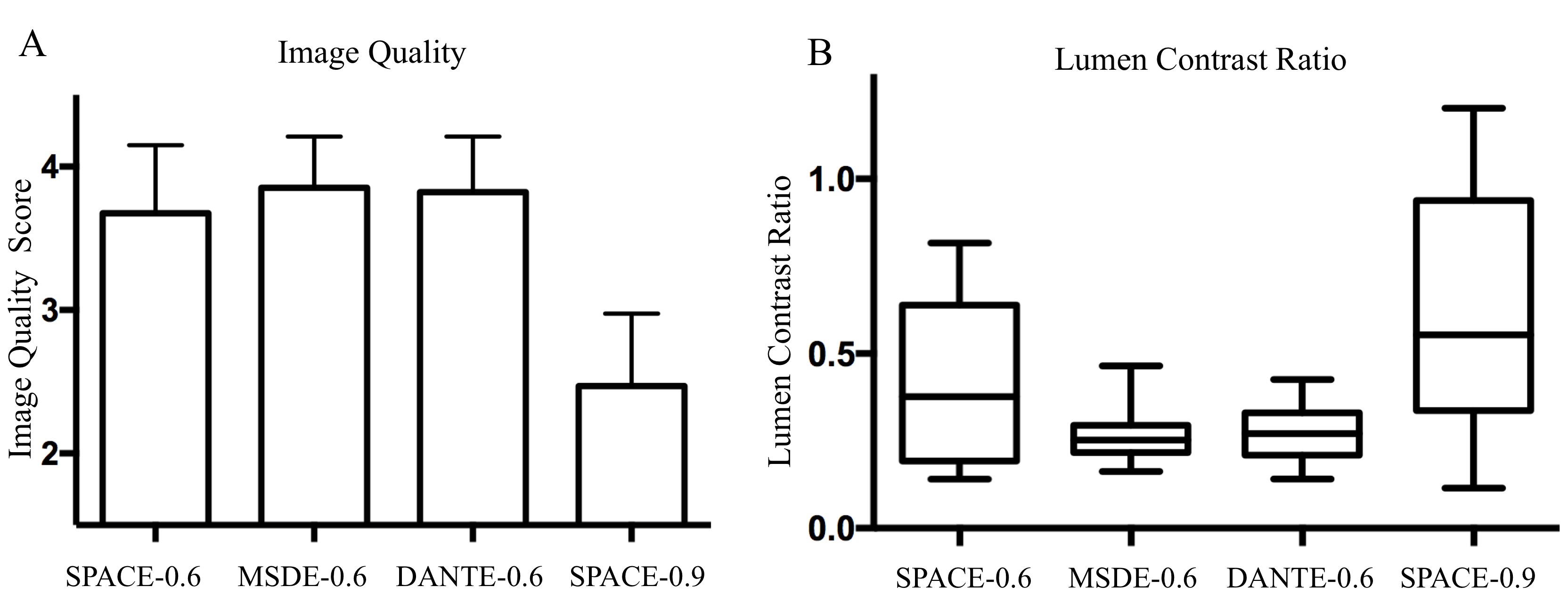
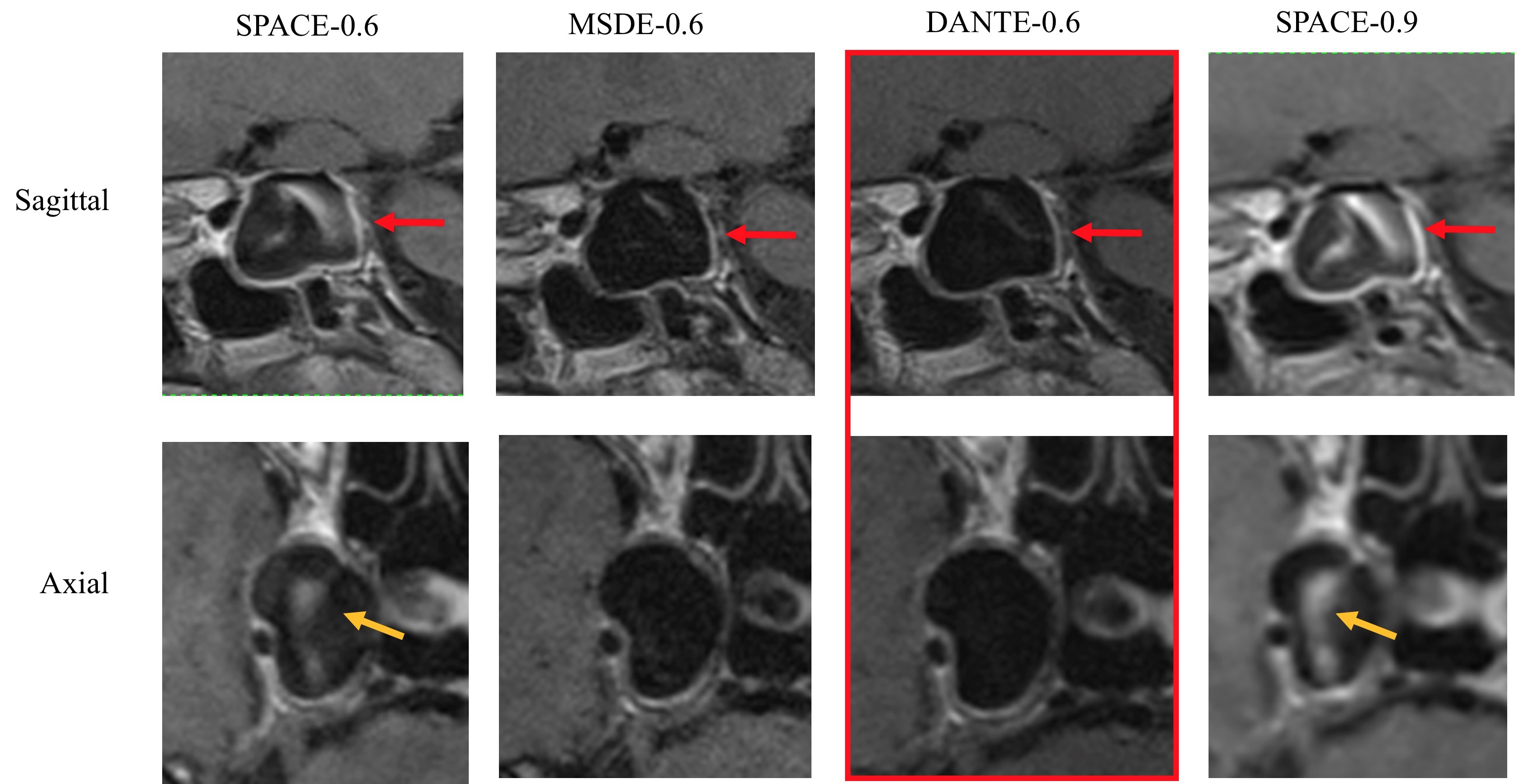
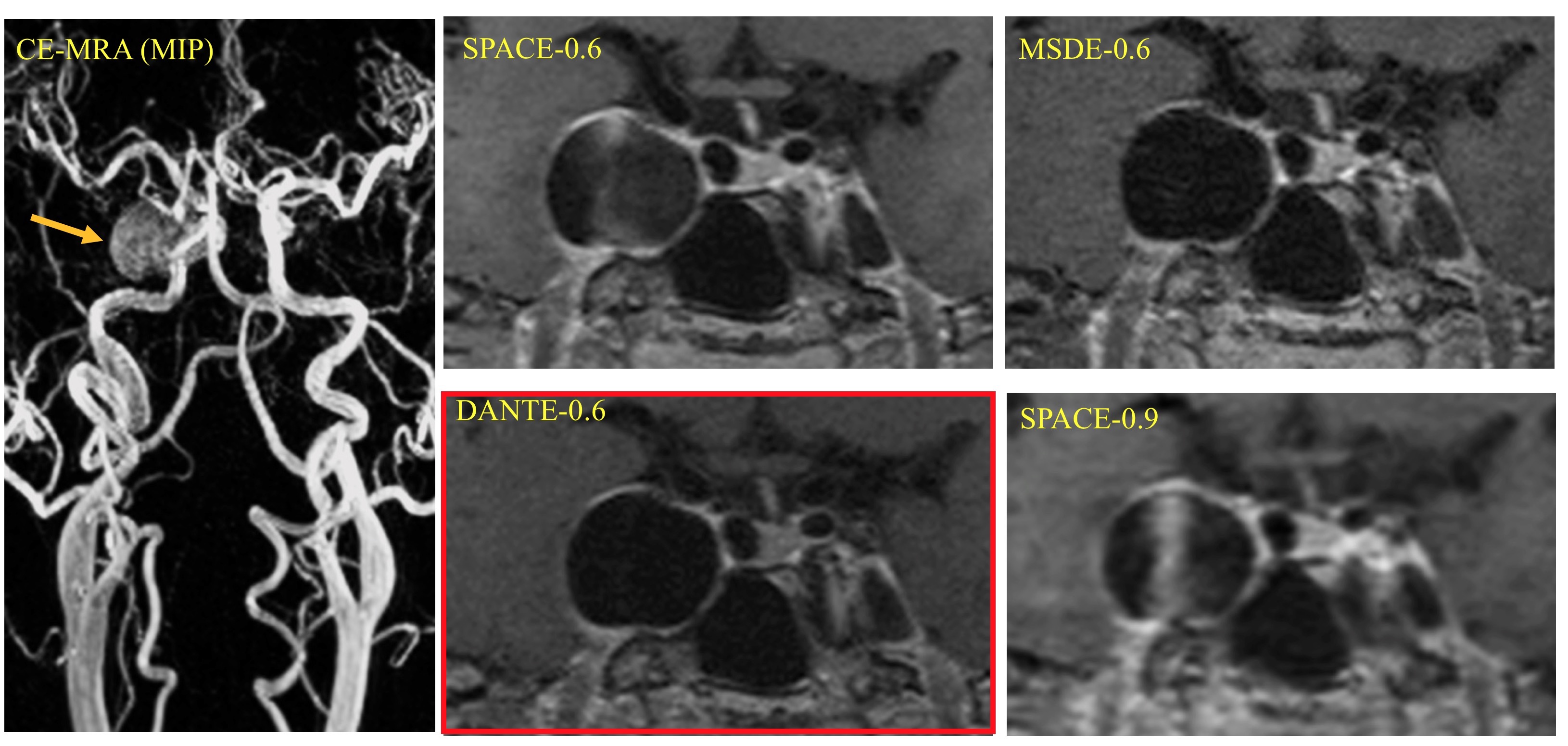
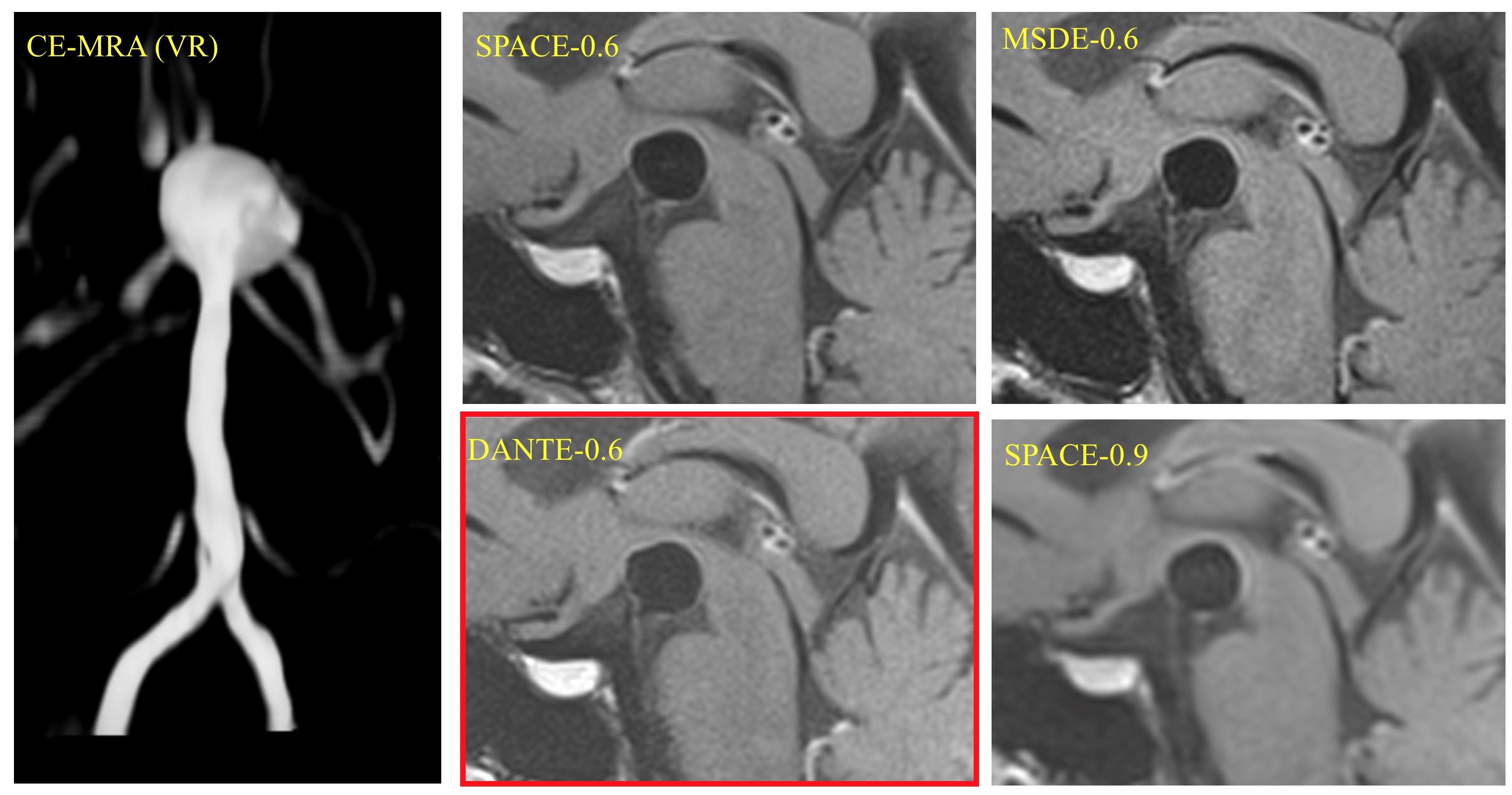
Of the 30 aneurysms, there were 25 internal carotid aneurysms (ICA), 2 basilar aneurysms (BA), 1 vertebral aneurysm (VA), 2 anterior communicating aneurysms (ACA). Average size of aneurysms was 11±8mm. Low-resolution SPACE significantly overestimated AWE (20/30 enhanced) compared to high-resolution SPACE (16 enhanced) and sequences with MSDE/DANTE (14 and 13 enhanced), as shown in Figure 1A. When there was AWE, the characterization of eccentric/concentric pattern was similar for all four sequences. Similarly, low-res SPACE also had significantly higher enhancement score (SPACE-0.9, 1.76±1.42; SPACE-0.5, 1.29±1.38; MSDE-SPACE 1.15±1.37; DANTE-SPACE 1.09±1.40; p<0.001, Figure 1B). SPACE-0.9 had significantly lower image quality (2.5±0.5) than other sequences (SPACE-0.6, 3.7±0.5; MSDE 3.9±0.4; DANTE 3.8±0.4, p<0.001, Figure 2A). SPACE-0.9 and SPACE-0.6 had significantly higher lumen contrast ratio than MSDE and DANTE (0.62±0.35, 0.43±0.26; 0.27±0.09; 0.27±0.08, p=0.001, Figure 2B). Patient images are shown in Figure 3-5. DANTE-SPACE had the best image quality with good blood suppression and SNR. Low-resolution SPACE shows thicker walls and more enhancement.Discussion
To our knowledge, this is the first study comparing black blood sequences with variable resolution and advanced blood suppression techniques for AWE assessment. The low-resolution (~1mm) SPACE sequence is widely used clinically because of its short (<5 minutes) scan time, but it can significantly overestimate AWE. The high-resolution SPACE (0.5-0.6mm isotropic) has only been used in a few research centers, as it normally takes 8-10 minutes. Advanced blood suppression techniques including MSDE and DANTE for vessel wall imaging are not widely available. However, our results highlight the importance of using high resolution imaging or MSDE/DANTE, as the clinical low-resolution protocol may misclassify 1/3 of aneurysms (7/20). High-resolution SPACE may have better blood suppression because of stronger readout gradients, longer acquisition times and different intra-voxel phase dispersion, although this is not yet fully determined. To reduce the long scan time of the high-resolution protocols, compressed sensing methods can be used without sacrificing image quality. Although both MSDE and DANTE achieve excellent blood suppression, DANTE-SPACE was chosen as the optimal sequence for 2 reasons: 1) MSDE induces T2 weighting into the T1-weighted imaging due to its T2-prep nature3 , so it may also suppress the wall enhancement, as concentrated Gd has reduced T2 values; DANTE has minimal added weightings. 2) T2 decay from MSDE also reduces the image SNR, while this is less significant for DANTE.Conclusion
Low-resolution 3D black blood MRI significantly overestimated AWE. DANTE-SPACE with 0.6mm isotropic resolution provides the best image quality for AWE assessment among the four sequences.Acknowledgements
Supported by NIH grant K99-HL136883.References
1. Edjlali M, Guedon A, Ben Hassen W, Boulouis G, Benzakoun J, Rodriguez-Regent C, et al. Circumferential thick enhancement at vessel wall mri has high specificity for intracranial aneurysm instability. Radiology. 2018;289:181-187
2. Kalsoum E, Chabernaud Negrier A, Tuilier T, Benaissa A, Blanc R, Gallas S, et al. Blood flow mimicking aneurysmal wall enhancement: A diagnostic pitfall of vessel wall mri using the postcontrast 3d turbo spin-echo mr imaging sequence. AJNR. American journal of neuroradiology. 2018;39:1065-1067
3. Zhu C, Graves MJ, Yuan J, Sadat U, Gillard JH, Patterson AJ. Optimization of improved motion-sensitized driven-equilibrium (imsde) blood suppression for carotid artery wall imaging. Journal of cardiovascular magnetic resonance : official journal of the Society for Cardiovascular Magnetic Resonance. 2014;16:61
4. Li L, Chai JT, Biasiolli L, Robson MD, Choudhury RP, Handa AI, et al. Black-blood multicontrast imaging of carotid arteries with dante-prepared 2d and 3d mr imaging. Radiology. 2014;273:560-569
5. Zhu C, Haraldsson H, Tian B, Meisel K, Ko N, Lawton M, et al. High resolution imaging of the intracranial vessel wall at 3 and 7 t using 3d fast spin echo mri. MAGMA. 2016;29:559-570
6. Tian B, Toossi S, Eisenmenger L, Faraji F, Ballweber MK, Josephson SA, et al. Visualizing wall enhancement over time in unruptured intracranial aneurysms using 3d vessel wall imaging. Journal of magnetic resonance imaging : JMRI. 2018
Figures