0742
Cerebral Perfusion Territory Changes after Direct Revascularization Surgery in Moyamoya Disease: A Super Selective Arterial Spin Labeling Study1Radiology Department, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 2MR Research, GE Healthcare, China, Beijing, China
Synopsis
The super selective arterial spin labeling (ssASL) was used in the early postoperative period to evaluate the revascularization area (RA) obtained by a bypass from the superficial temporal artery to the middle cerebral artery in Moyamoya disease, and the perfusion territory changes of the major cerebral arteries were evaluated. The results indicated the postoperative perfusion territory changes of the major cerebral arteries differed between the RA-positive group and the RA-negative group. The incidence of preoperative external carotid artery compensation was significantly higher in the RA-negative group than the RA-positive group. There was good intermodality agreement between ssASL and CT angiography.
Introduction
Moyamoya disease is generally treated by revascularization surgery. Currently, there is no imaging modality used in clinical practice that can evaluate the perfusion territory of individual arteries postoperatively. In the present study, the super selective arterial spin labeling (ssASL) technique was used in the early postoperative period to evaluate the revascularization area (RA) obtained through superficial temporal artery (STA) to middle cerebral artery (MCA) bypass in patients with Moyamoya disease.Methods
Thirty patients with Moyamoya disease treated via unilateral STA-to-MCA bypass were included. ssASL was performed preoperatively and within 1 week postoperatively. ssASL was performed on a 3.0T whole body system (GE Discovery 750) equipped with an 8 channel head coil. TOF-MRA was acquired and used for locating the target arteries to be labeled. Bilateral internal carotid artery (ICA), bilateral external carotid artery (ECA) and vertebrobasilar artery (VBA) were individually labelled via super-selective scheme. The corresponding perfusion territory maps were acquired with 3D stack of spiral fast spin echo sequence and the parameters were as follows: labeling duration 1450ms, post labeling delay 2025ms, 4 arms, 512 points per arm, NEX 2, slice thickness 4mm. A circle labeling region of radius 20mm was used. The RA was examined by labeling the STA-to-MCA bypass postoperatively. The pre- and postoperative perfusion territories of the bilateral internal carotid arteries, bilateral external carotid arteries, and the basilar artery were also examined and compared. Postoperative CT angiography was performed and compared with the ssASL results.
Results
In 14 of 30 patients (46.7%), ssASL demonstrated the presence of a RA (RA-positive), while 16 patients (53.3%) had no RA (RA-negative). In the RA-positive group, the mean volume of the RA was 80.32±8.13 ml (range 34.95–142.50 ml). The postoperative perfusion territory changes of the major cerebral arteries differed between the RA-positive group and the RA-negative group. The incidence of preoperative external carotid artery compensation was significantly higher in the RA-negative group than the RA-positive group (F=0.011, P<0.05). There was good intermodality agreement between ssASL and CT angiography (κ=0.780).Discussion
Revascularization surgery is expected to cause a change in cerebral vascular supply. Our study indicated that the RA-positive group had more a favorable surgical outcome in the early postoperative stage than the RA-negative group. Firstly, the presence of a RA indicated the presence of an increased blood supply from the ECA through the bypass. Secondly, the decrease in the perfusion territory of a single artery was attributed to the reduction of the hemodynamic load. In the RA-negative group, the perfusion territories of the ipsilateral ICA and/or BA did not change, as there was no newly-added blood supply, suggesting that there was no reduction in the hemodynamic load of the abovementioned arteries.
Our results showed that preoperative ipsilateral ECA compensation was significantly more common in the RA-negative group than the RA-positive group.This may suggest that preoperative ECA compensation is related to an unfavorable outcome of direct revascularization surgery in the early postoperative stage. Further study involving a large case series and long-term follow-up is needed.
The major limitation of our study was that the presence of a RA demonstrated by ssASL was verified on CTA rather than postoperative DSA, which is the gold standard for demonstrating bypass patency. However, the image quality of CTA has continuously improved with the development of CT scanner technology, and CTA reportedly shows good agreement with DSA in the evaluation of STA-to-MCA bypass surgery
Conclusion
ssASL can demonstrate the RA obtained by direct revascularization, and the postoperative perfusion territory changes of the major cerebral arteries. It is a promising technique for the postoperative evaluation of patients with MMD. The preoperative compensation status in MMD may be a factor influencing the outcome of direct revascularization surgery.Acknowledgements
No acknowledgement found.References
[1] Hartkamp NS, Petersen ET, De Vis JB, Bokkers RP, Hendrikse J. Mapping of cerebral perfusion territories using territorial arterial spin labeling: techniques and clinical application. NMR Biomed. 2013; 26: 901-12.
[2]Saida T, Masumoto T, Nakai Y, Shiigai M, Matsumura A, Minami M. Moyamoya disease: evaluation of postoperative revascularization using multiphase selective arterial spin labeling MRI. J Comput Assist Tomogr. 2012; 36: 143-9.
[3]Kitajima M, Hirai T, Shigematsu Y, Fukuoka H, Sasao A, Okuda T, Morioka M, Kai Y, Yamashita Y. Assessment of cerebral perfusion from bypass arteries using magnetic resonance regional perfusion imaging in patients with moyamoya disease. Jpn J Radiol. 2010; 28:746-53.
Figures
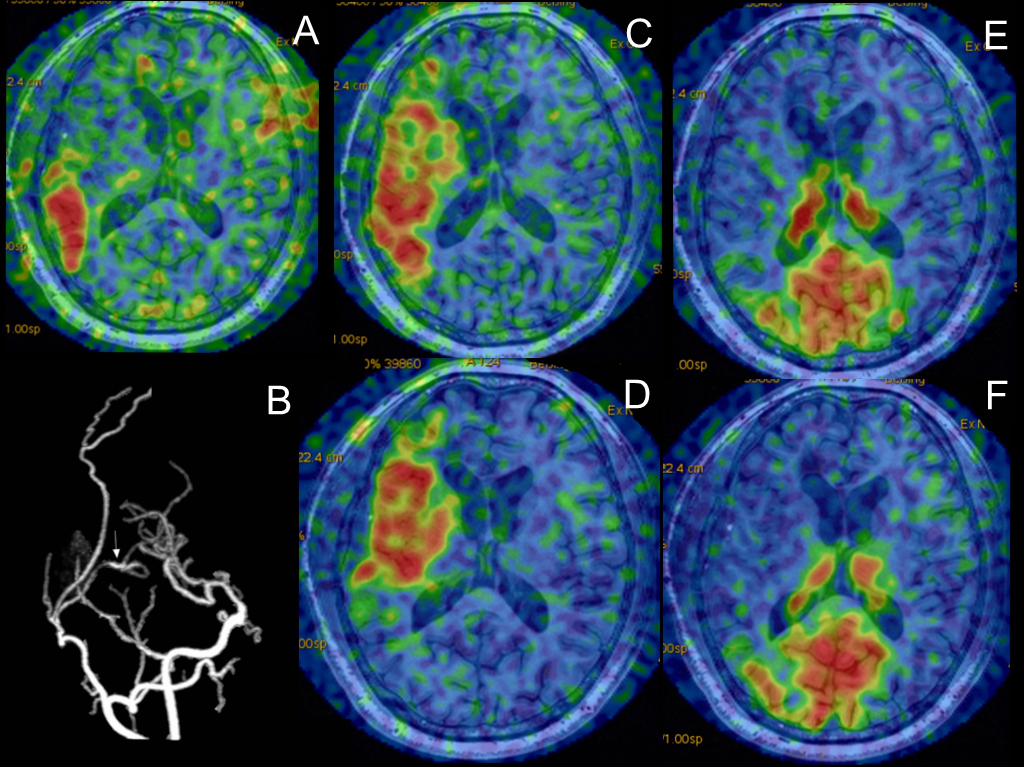
Figure 1. A typical case from the RA-positive group.
(A) Postoperative ssASL imaging of the bypass demonstrating the presence of a RA.
(B) Postoperative CTA showing that the STA and MCA branches were connected, thus confirming the bypass patency.
(C and D) Pre- and postoperative ssASL images of the right ICA demonstrating that the perfusion territory of the right ICA was reduced due to the presence of the RA.
(E and F) Pre- and postoperative ssASL images of the BA were unchanged. RA-positive group: patients in whom a revascularization area was visualized on territory arterial spin labeling after bypass surgery;
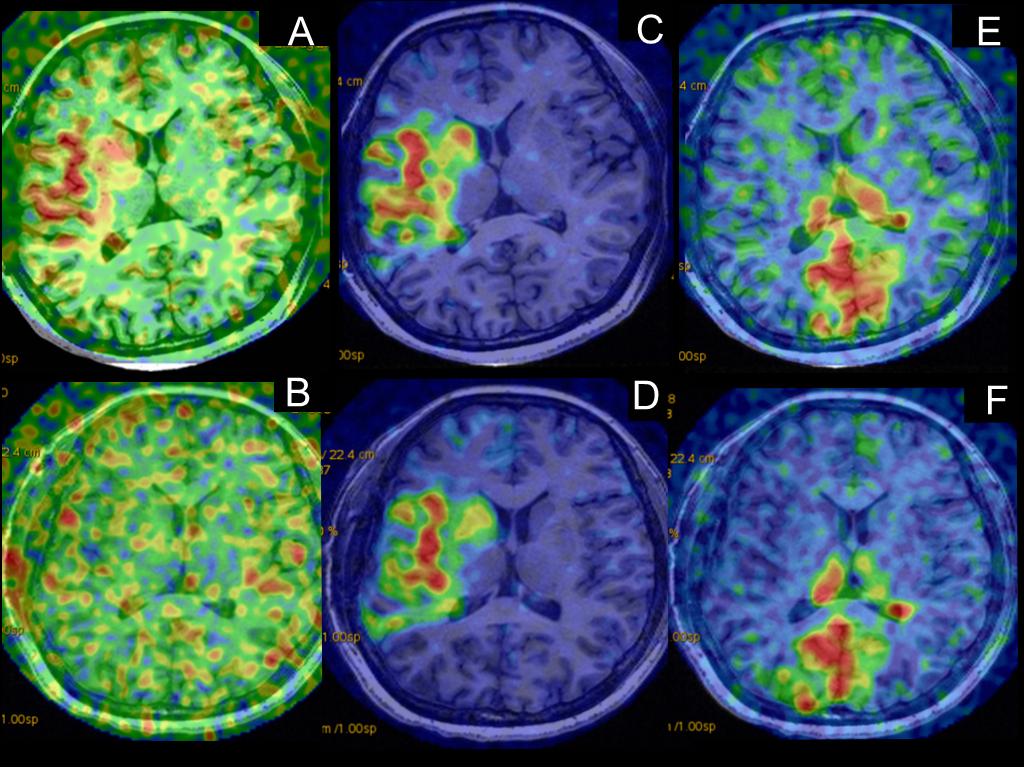
Figure 2. A typical case from the RA-negative group.
(A) Preoperative ssASL image of the right ECA demonstrating compensatory blood supply to the brain.
(B) Postoperative ssASL image of the bypass demonstrating the absence of a RA. The preoperative compensatory blood supply disappeared after bypass surgery.
(C and D) Pre- and postoperative ssASL images of the right ICA were unchanged.
(E and F) Pre- and postoperative T-ASL images of the BA were unchanged. RA-negative group: patients in whom a revascularization area was not visualized on territory arterial spin labeling after bypass surgery.