0741
Elevated oxygen extraction fraction is a tissue biomarker of chronic ischemia for cerebral small vessel disease1Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, MO, United States, 2Department of Neurology, Washington University School of Medicine, St. Louis, MO, United States
Synopsis
Cerebral small vessel disease (CSVD) increases stroke risk and often leads to vascular cognitive impairment. We hypothesized that elevated oxygen extraction fraction (OEF) is a tissue biomarker of chronic ischemia in patients with CSVD. We found that reduction of cerebral blood flow (CBF) in gray matter depends on age, but not on CSVD. In contrast, OEF is increased in watershed and white matter in patients with CSVD and watershed OEF is significantly associated with white matter hyperintensities (WMH) lesion volumes after adjusting for age.
Introduction
Cerebral small vessel disease (CSVD) increases stroke risk and often leads to vascular cognitive impairment, the 2nd leading cause of dementia and a major contributor to Alzheimer’s disease.1 It has been postulated that exposure to risk factors, including hypertension, diabetes, and smoking over years injures small arterioles, impairs autoregulation, and lead to chronic hypoxia/ischemia.2-4 We hypothesized that elevated oxygen extraction fraction (OEF) is a tissue biomarker of chronic ischemia in patients with CSVD. To test this hypothesis, we compared cerebral blood flow (CBF) and OEF among young control, older control, and patients with CSVD. In addition, we examined whether OEF is associated with white matter hyperintensities (WMH) volume.Methods
A prospective MRI study enrolled three cohorts of subjects: (1) young healthy control (N=22, 13 females, age: 32 [27, 38] (Median [IQR]); (2) older healthy control (N=16, 10 females, age: 54 [52, 58] (Median [IQR]); and (3) patients with CSVD risk factors and WMH (N=28, 11 females, age: 70 [64, 77] (Median [IQR]). T1w and FLAIR images were acquired. CBF maps were obtained using pseudo-continuous arterial spin labelling (pCASL).5 OEF maps were obtained using an asymmetric spin echo sequence.6 WMH lesions were manually segmented by a board-certified vascular neurologist on FLAIR images to create FLAIR lesion masks. Absolute WMH lesion volumes (VWMH) were measured using the FLAIR lesion masks. To account for variations in brain volume across patients, relative WMH volume (rVWMH) was computed as a ratio of VWMH to total brain volume. Relative OEF (rOEF) maps were computed by normalizing OEF with respect to gray matter median OEF for each subject. All maps were then aligned to the symmetric International Consortium of Brain Mapping (ICBM) brain atlas.
T1w images were used to segmented tissue into gray matter, white matter and CSF. A watershed ROI was defined as a region within the lowest 10th percentile CBF within white matter using a separate young healthy adult cohort (N=38, 25 females, age: 49.5 [31, 54] (Median [IQR])). This watershed ROI was applied to CBF and OEF maps for all subjects in this study. Mean CBF and rOEF values were calculated in gray matter (GM), white matter (WM) and watershed (WS) ROIs respectively for all three cohorts. Group comparison was performed across all three groups with one-way analysis of variance (ANOVA) and post-hoc pairwise comparisons after adjusting for multiple comparison. In addition, linear regression were performed to evaluate the correlation between rVWMH and age and watershed rOEF in subjects with non-zero WMH.
Results
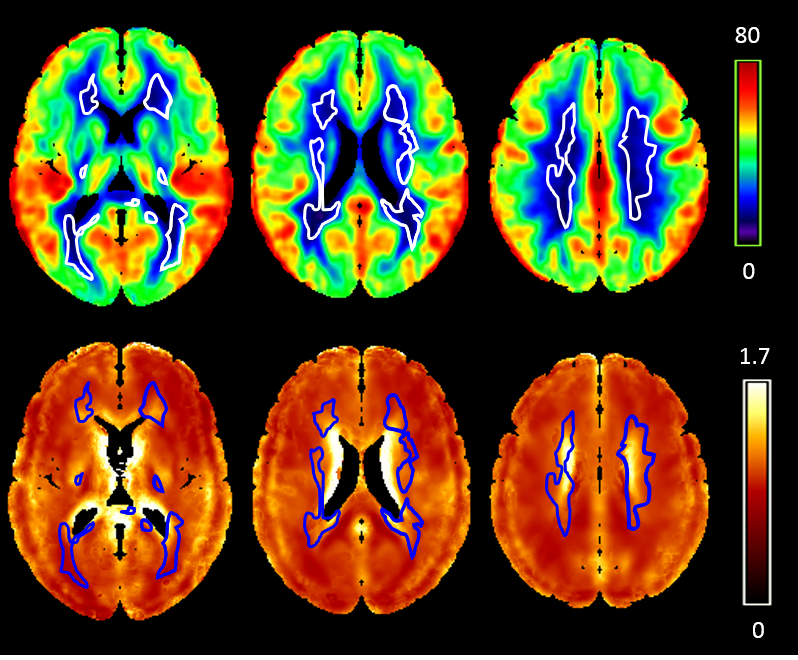
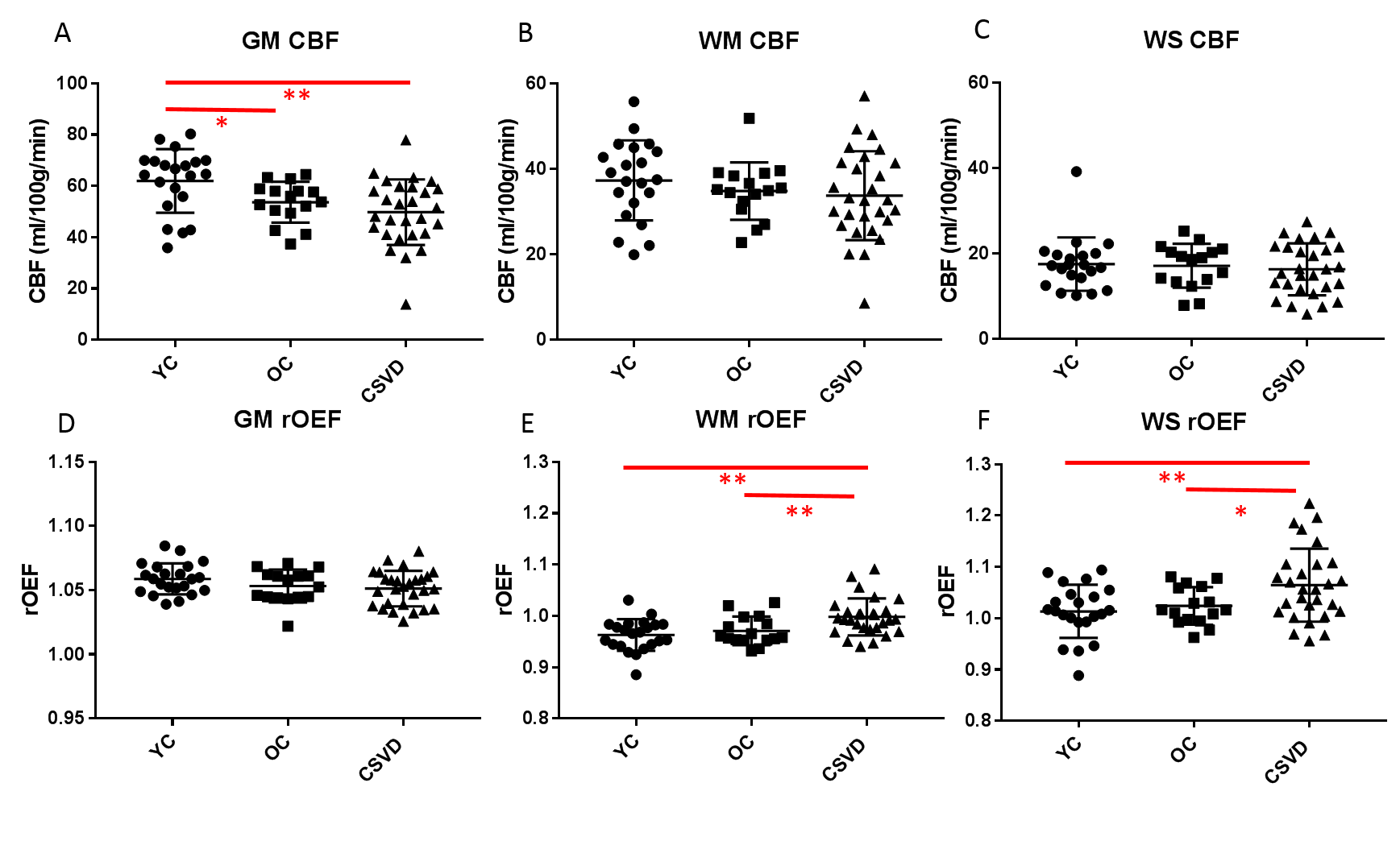
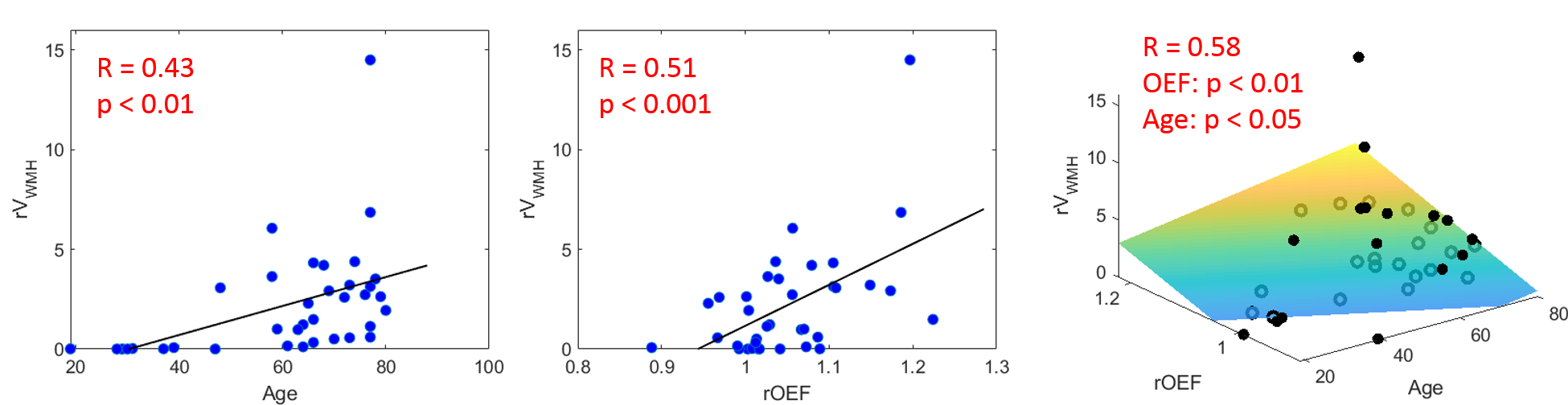
Figure 1 shows the watershed ROI overlaid on average CBF and rOEF maps of the WMH cohort. Low CBF and high rOEF were observed in the watershed. CBF is significantly higher in gray matter in young control group (p<0.01), while it is not different between the CSVD patient and age matched old control groups (Figure 2). There is no difference in CBF in either white matter or watershed among three groups. This result suggests that gray matter CBF reduction depends on age, but not on CSVD. In contrast, OEF is significantly higher in white matter and the watershed between CSVD patients and young controls (p<0.01 in both white matter and watershed), and between CSVD patients and old controls (p<0.01 in white matter, p<0.05 in watershed). Using uni-variate regression, rVWMH is significantly associated with both age (p<0.01) and watershed rOEF (p<0.001) (Figure 3). Moreover, rVWMH is significantly correlated with watershed rOEF (p < 0.01), after adjusting for age in a bi-variate regression (Figure 3).Discussion
In vivo markers of CSVD promise to identify individuals at increased risk of vascular cognitive impairment.7 Despite a high spatial overlap between regions of low CBF and regions with high WMH burden, CBF is not different between older subjects with and without WMH. Our results suggest that the gray matter CBF reduction may be the outcome of normal aging but not CSVD, thus limiting its use as an age-independent biomarker of CSVD. In contrast, we have demonstrated that watershed rOEF is elevated in patients with WMH. In addition, watershed rOEF is highly associated with rVWMH even after adjusting for age. In summary, CBF shows intrinsic regional vulnerability, but its reduction is impacted more by aging than by CSVD impairment. In contrast, our results support elevated watershed OEF as a tissue biomarker of chronic ischemia in patients with CSVD.Conclusion
Watershed rOEF is selectively elevated in adults with WMH compared to young and older healthy adults. Moreover, it is significantly correlated with rVWMH after adjusting for age. Our results demonstrate that watershed rOEF provide a tissue biomarker of chronic ischemia for CSVD.Acknowledgements
This study was supported by grant from the National Institute of Health NIH 1R01NS082561, R01HL129241References
1. Kalaria, Raj N., and Timo Erkinjuntti. "Small vessel disease and subcortical vascular dementia." Journal of clinical neurology 2.1 (2006): 1-11.
2. Schmidt, Reinhold, Stephan Seiler, and Marisa Loitfelder. "Longitudinal change of small-vessel disease-related brain abnormalities." Journal of Cerebral Blood Flow & Metabolism36.1 (2016): 26-39.
3. Dickie, David Alexander, et al. "Vascular risk factors and progression of white matter hyperintensities in the Lothian Birth Cohort 1936." Neurobiology of aging 42 (2016): 116-123.
4. Walker, Keenan A., et al. "The association of mid-to late-life systemic inflammation with white matter structure in older adults: The Atherosclerosis Risk in Communities Study." Neurobiology of Aging 68 (2018): 26-33.
5. Floyd, Thomas F., et al. "Precision of the CASL‐perfusion MRI technique for the measurement of cerebral blood flow in whole brain and vascular territories." Journal of Magnetic Resonance Imaging 18.6 (2003): 649-655.
6. An, Hongyu, and Lin, Weili. "Cerebral oxygen extraction fraction and cerebral venous blood volume measurements using MRI: effects of magnetic field variation." Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 47.5 (2002): 958-966.
7. De Silva, T. Michael, and Alyson A. Miller. "Cerebral small vessel disease: targeting oxidative stress as a novel therapeutic strategy." Frontiers in pharmacology 7 (2016): 61.
Figures