0740
Intracranial vessel wall thickness measurements: A post-mortem comparison between hypertensive patients and controls1Center for Image Sciences, University Medical Center Utrecht, Utrecht, Netherlands, 2Image Sciences Institute, University Medical Center Utrecht, Utrecht, Netherlands, 3Department of Radiology, University Medical Center Utrecht, Utrecht, Netherlands
Synopsis
For the intracranial arteries, only a few studies have investigated arterial wall thickening. In this post-mortem, explorative study we investigated the effect of hypertension on vascular remodeling in the Circle of Willis in male and female groups using 7T MRI. Circle of Willis specimens were scanned at ultra-high resolution(0.11mm isotropic). Vessel wall thickness and vessel wall area were measured at 21 locations across the major arterial branches. Results showed a larger vessel wall thickness and area in the female hypertension subgroup in four different arteries as compared to the control group(p<0.05). Male hypertension and control groups showed no significant difference.
Purpose
Hypertension is one of the largest risk factors for cardiovascular disease, contributing to 54% of all strokes worldwide.1,2 The effect of hypertension on the vessel wall morphology has been well described for the extracranial vasculature3–6, showing that arterial remodeling due to hypertension is different between men and women.7,8 Until now, only a few studies have investigated wall thickening in the intracranial arteries.9–11
This explorative study aims to measure the extent and location of vascular remodeling due to hypertension from high resolution 7T MR acquisitions of post-mortem specimens in male and female subgroups.
Materials and methods
In this study, a total of 50 post-mortem circle of Willis specimens were used. Twenty-five circles originated from healthy controls and 25 circles from hypertensive patients. Patients were included in the hypertension group when they had a systolic or diastolic blood pressure above 140 mmHg or 90 mmHg respectively, or were using antihypertensive drugs, in the last year of their life.12 In each group 15 male and 10 female patients were included. Male hypertension and control groups had similar age ranges (68.8±9.4 and 66.7±8.9 years, respectively (mean ± standard deviation)), which was also the case for the female hypertension and control subgroups (69.6±8.6 and 69.1±11.1 years, respectively).
An ultra-high resolution sequence (3D gradient echo, isotropic acquired voxel size: 0.11 mm, described elsewhere9) was performed at 7T MRI (Philips, Best, The Netherlands). Vessel wall measurements were performed at 21 locations in the circle of Willis, and were grouped into 9 anatomical locations (Figure 1).
For each specimen, the mean vessel wall thickness and mean vessel wall area were estimated per anatomical location, as measure for the arterial remodeling.13 The centerline of the lumen was automatically traced per measurement location for roughly 1-2 mm and was visually inspected on accuracy. A multiplanar reconstruction (MPR) was performed along this centerline. Slices in the MPR stack that did not correctly follow the centerline were removed from further analysis.
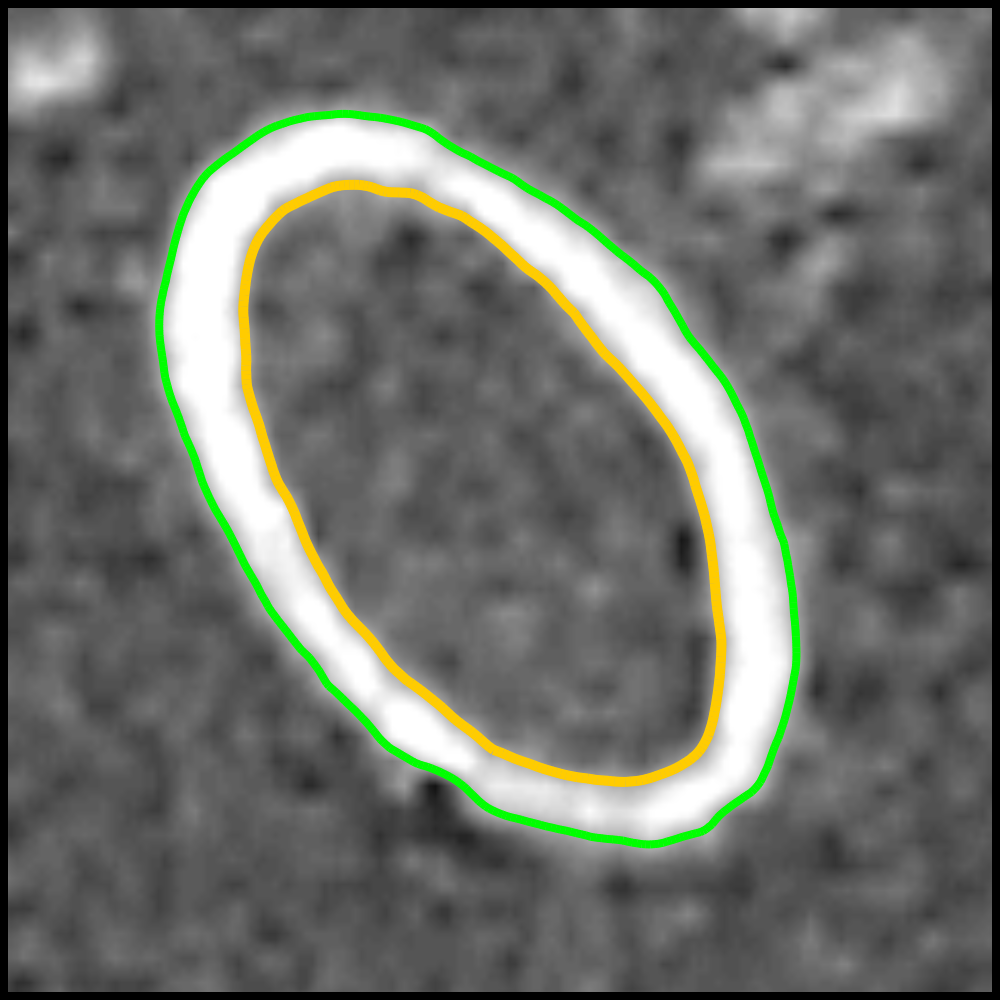
Next, for each slice in the MPR stack an isocontour was computed at the inner and outer boundary of the vessel wall, at the full width at half maximum (FWHM) intensity value. Example contours for a single slice are given in Figure 2. Subtracting the area of the outer contour (green) from the area of the inner contour (yellow) yields the vessel wall area. The vessel wall area was averaged over all used slices in the MPR stack per location.
A nearest neighbour search was employed for all points on the inner contour, to find the distance to the closest point on the outer contour, and vice versa. The mean vessel wall thickness was defined as the median contour-contour distance between the inner and outer contours, over all used slices in the MPR stack.
A Mann-Whitney U test was used to test for statistically significant differences in the vessel wall thickness measurements between the hypertension and control groups.
Results
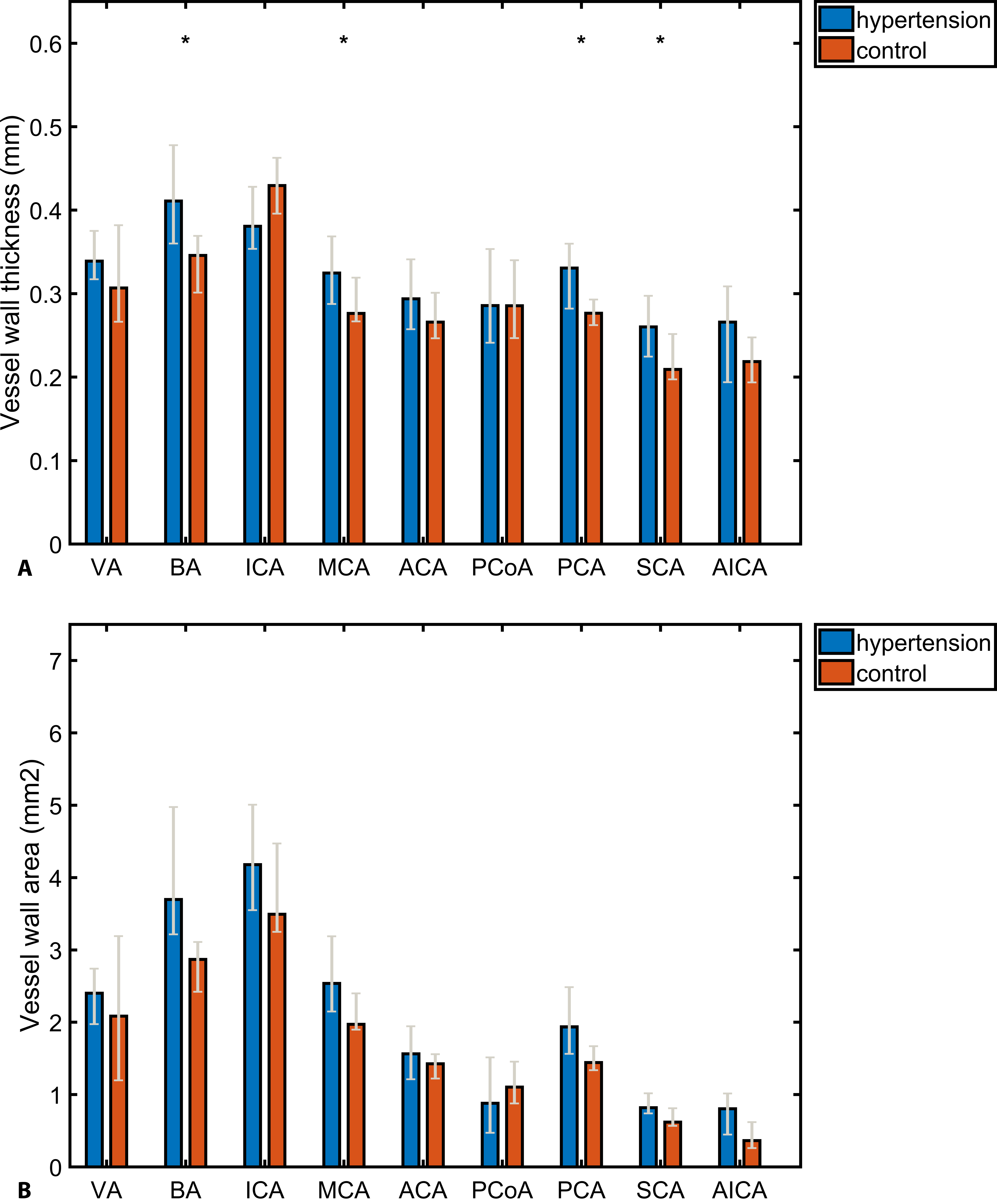
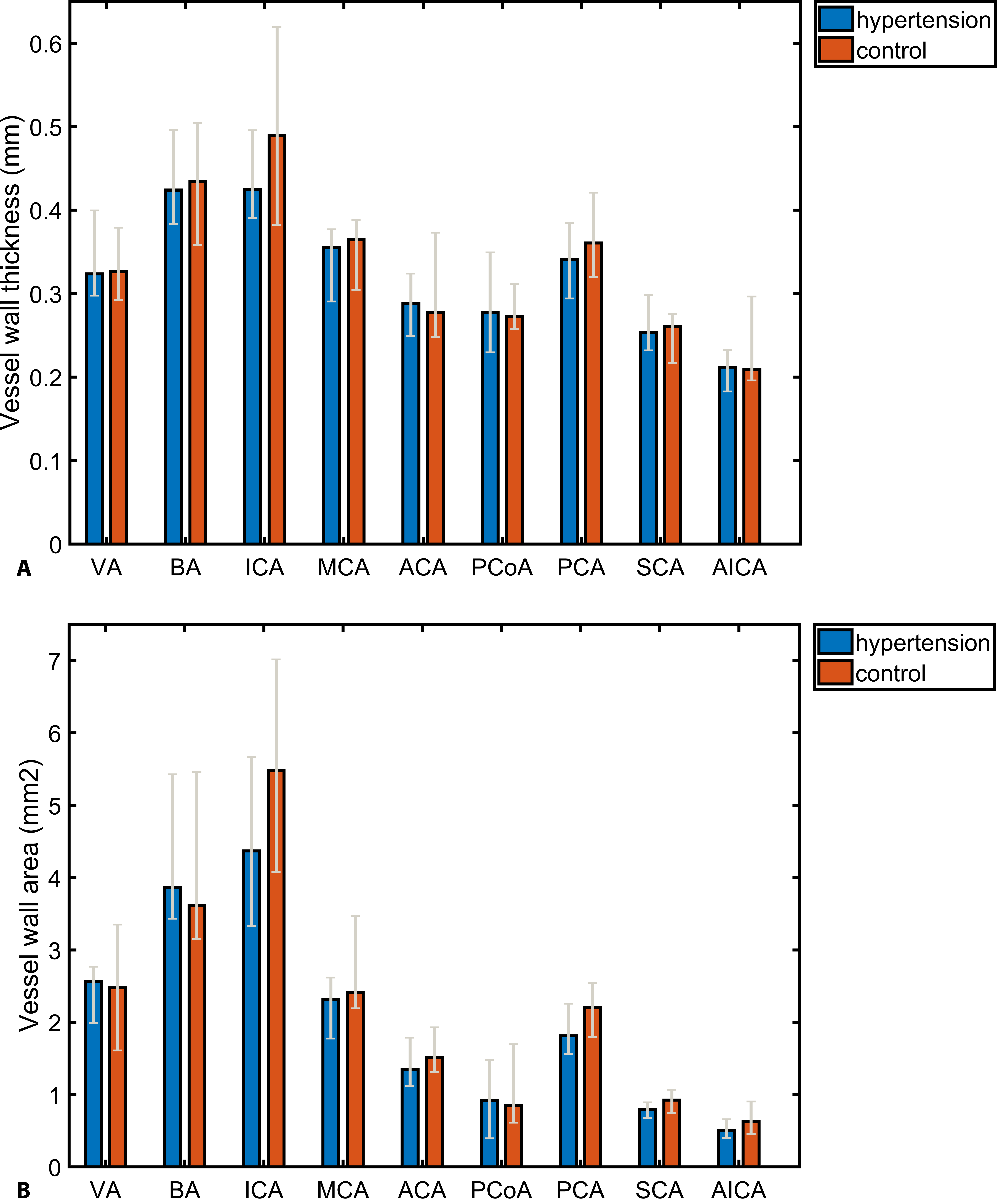
The results of our female and male analyses are given in Figures 3 and 4, respectively. The vessel wall thickness for the female hypertension group was larger than that of the female control group for almost all anatomical locations (Figure 3). This difference was significant for the BA, MCA, PCA and SCA locations (p<0.05), where the vessel wall was respectively 18.8%, 17.5%, 19.6% and 24.3% thicker (average: 20%). The vessel wall area was 28.8%, 28.6%, 34.1% and 31.7% larger for the BA, MCA, PCA and SCA locations respectively (average: 31%). For the male subgroup, no significant differences were found between hypertension and control groups (Figure 4).Discussion/Conclusion
Hypertrophic remodeling was observed in the female hypertension subgroup at the BA MCA, SCA, and PCA locations, where on average the vessel wall was 20% thicker and the vessel wall area was 31% larger than that of controls. The male subgroup showed no significant effect of hypertension on the vessel wall thickness.
The vessel wall thickness and vessel wall area were comparable between male and female hypertension subgroups, whereas the male control group showed thicker walls and a larger vessel wall area than the female control group. Research has shown that male gender is associated with a larger vessel wall thickness, possibly explaining differences in control group measurements.14 Confounding variables linked to vessel wall thickening, such as smoking15, BMI16, and presence of advanced atherosclerotic plaques17, could have impacted the observed results for all locations.
The preliminary results of our explorative study warrant additional analyses. Stratifying for the described variables can clarify the underlying effect and extent of hypertension on the intracranial vessel wall morphology in males and females.
Acknowledgements
No acknowledgement found.References
1. Lawes CM, Hoorn S Van der, Rodgers A. Global burden of blood-pressure-related disease, 2001. Lancet. 2008 May 3;371(9623):1513–8.
2. Dahlöf B. Prevention of Stroke in Patients with Hypertension. Am J Cardiol. 2007;100(3 SUPPL.).
3. Litwin M, Niemirska A, Śladowska J, et al. Left ventricular hypertrophy and arterial wall thickening in children with essential hypertension. Pediatr Nephrol. 2006;21(6):811–9.
4. Park JB, Schiffrin EL. Small artery remodeling is the most prevalent (earliest?) form of target organ damage in mild essential hypertension. J Hypertens. 2001;19(5):921–30.
5. Suurküla M, Fagerberg B, Wendelhag I, et al. Atherosclerotic disease in the femoral artery in hypertensive patients at high cardiovascular risk. The value of ultrasonographic assessment of intima-media thickness and plaque occurrence. Risk Intervention Study (RIS) Group. Arterioscler Thromb Vasc Biol. 1996 Aug;16(8):971–7.
6. Chironi G, Gariepy J, Denarie N, et al. Influence of hypertension on early carotid artery remodeling. Arterioscler Thromb Vasc Biol. 2003;23(8):1460–4.
7. Batton KA, Austin CO, Bruno KA, et al. Sex differences in pulmonary arterial hypertension: role of infection and autoimmunity in the pathogenesis of disease. Biol Sex Differ. 2018 Dec 18;9(1):15.
8. Chien CY, Liu CC, Po HL, et al. The relationship among carotid artery remodeling, cardiac geometry, and serum N-terminal Pro-B-Type natriuretic peptide level in asymptomatic Asians: Sex-differences and longitudinal GEE study. PLoS One. 2015;10(7):1–13.
9. Harteveld AA, Denswil NP, Van Hecke W, et al. Ex vivo vessel wall thickness measurements of the human circle of Willis using 7T MRI. Atherosclerosis. 2018 Jun 1;273:106–14.
10. Kontzialis M, Wasserman BA. Intracranial vessel wall imaging: current applications and clinical implications. Neurovascular Imaging. 2016;2(1):4.
11. Qiao Y, Steinman DA, Qin Q, et al. Intracranial arterial wall imaging using three-dimensional high isotropic resolution black blood MRI at 3.0 Tesla. J Magn Reson Imaging. 2011;34(1):22–30.
12. Chobanian A V, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 Report. JAMA. 2003 May 21;289(19):2560.
13. Mulvany MJ, Baumbach GL, Aalkjaer C, et al. Vascular remodeling. Hypertens (Dallas, Tex 1979). 1996 Sep;28(3):505–6.
14. Rosero EB, Peshock RM, Khera A, et al. Sex, race, and age distributions of mean aortic wall thickness in a multiethnic population-based sample. J Vasc Surg. 2011 Apr 1;53(4):950–7.
15. Rahman M, Laher I. Structural and Functional Alteration of Blood Vessels Caused by Cigarette Smoking: An Overview of Molecular Mechanisms. Curr Vasc Pharmacol. 2007;
16. Rashid SA, Mahmud SA. Correlation between carotid artery intima-media thickness and luminal diameter with body mass index and other cardiovascular risk factors in adults. Sultan Qaboos Univ Med J. 2015;
17. Bang OY. Intracranial Atherosclerosis: Current Understanding and perspectives. J stroke. 2014;16(1):27–35.
Figures