0739
Recovery of cerebrovascular reactivity after asymptomatic carotid artery stenosis treatment is assessable by Breathhold-fMRI within global watershed areas1Department of Neuroradiology, Technical University of Munich, Munich, Germany, 2MRRC, Yale University, New Haven, CT, United States, 3Clinic for Radiology, Technical University of Munich, Munich, Germany, 4Institute of Clinical Medicine, Aarhus University, Aarhus, Denmark, 5Philips Healthcare, Hamburg, Germany, 6Clinic for Neurology, Technical University of Munich, Munich, Germany, 7Institute of Radiopharmaceutical Cancer Research, Helmholtz-Zentrum Dresden-Rossendorf, Dresden, Germany
Synopsis
Asymptomatic unilateral internal carotid-artery stenosis (ICAS) causes complex and currently poorly understood hemodynamic impairments which could possibly improve treatment decisions. Cerebrovascular reactivity (CVR) is an important biomarker of vascular health and can potentially serve to evaluate ICAS-treatment efficacy. We present perfusion MRI-data from a longitudinal study in 16 asymptomatic ICAS-patients before and after treatment plus 17 age-matched healthy controls. We hypothesize that CVR impairments in ICAS and their recovery after treatment can be assessed by Breathhold-fMRI analyzed by a data-driven approach. Our results demonstrate statistically significant CVR impairments within global watershed areas before treatment and significant CVR recovery after treatment.
Purpose
Severe internal carotid-artery stenosis (ICAS) is a major public health issue, as it accounts for approximately 10% of all strokes.1 Treatment with carotid artery stenting (CAS) and carotid endarterectomy (CEA) has been associated with significantly reduced stroke risk.2 The treatment is, however, highly invasive3 – stenting relates to a mean 2-year mortality of 32%.4 This creates the need for non-invasive methods to support treatment decisions and evaluate the treatment efficacy. Detection of subtle hemodynamic changes in asymptomatic ICAS has high potential to address this need and identify patients who might benefit from treatment.5 Cerebrovascular reactivity (CVR) is an important biomarker of vascular health.6,7 Previous studies showed impaired CVR in ICAS and its recovery after treatment, however, commonly employed methods are invasive acetazolamide or complicated gas applications.6-11 We therefore propose an easily applicable Breathhold-fMRI (BH-fMRI) scheme for CVR assessment.7 As watershed areas are most vulnerable to hemodynamic impairments in ICAS,12,13 we hypothesize to be especially sensitive to CVR recovery after ICAS-treatment within global watershed areas (gWSA’s).
Methods
Before treatment, thirty-three participants (16 asymptomatic, asymptomatic unilateral ICAS-patients, age=71.4±5.8y and 17 healthy controls [HC], age=70.8±5.3y) underwent MRI on a 3T Philips Ingenia (Philips Healthcare, Best, Netherlands) using a 16-channel head-neck-coil. At minimum three months after treatment, a second MRI-scan was performed (Table1). HC’s were also scanned twice for comparisons. The imaging protocol and derived hemodynamic parameters are summarized in Fig.1. The BH-fMRI scheme comprised of five breathholds of 15 seconds, each. Data-driven analysis16 yielded CVR-maps for ICAS-patients and HC before and after treatment (Fig.1). In addition, DSC-data were acquired in both scans deriving rCBV-maps by parametric modelling14. All parameter-maps were MNI normalized. Processing was performed with SPM1217 and custom Matlab18 programs. Artefact-affected CVR-maps were excluded based on visual ratings (CP, SK, JG). Lateralization was assessed by comparing mean parameter-values within GM of gWSA’s between hemispheres. ICAS-patients were evaluated within hemispheres ipsilateral and contralateral to the stenosis.Results
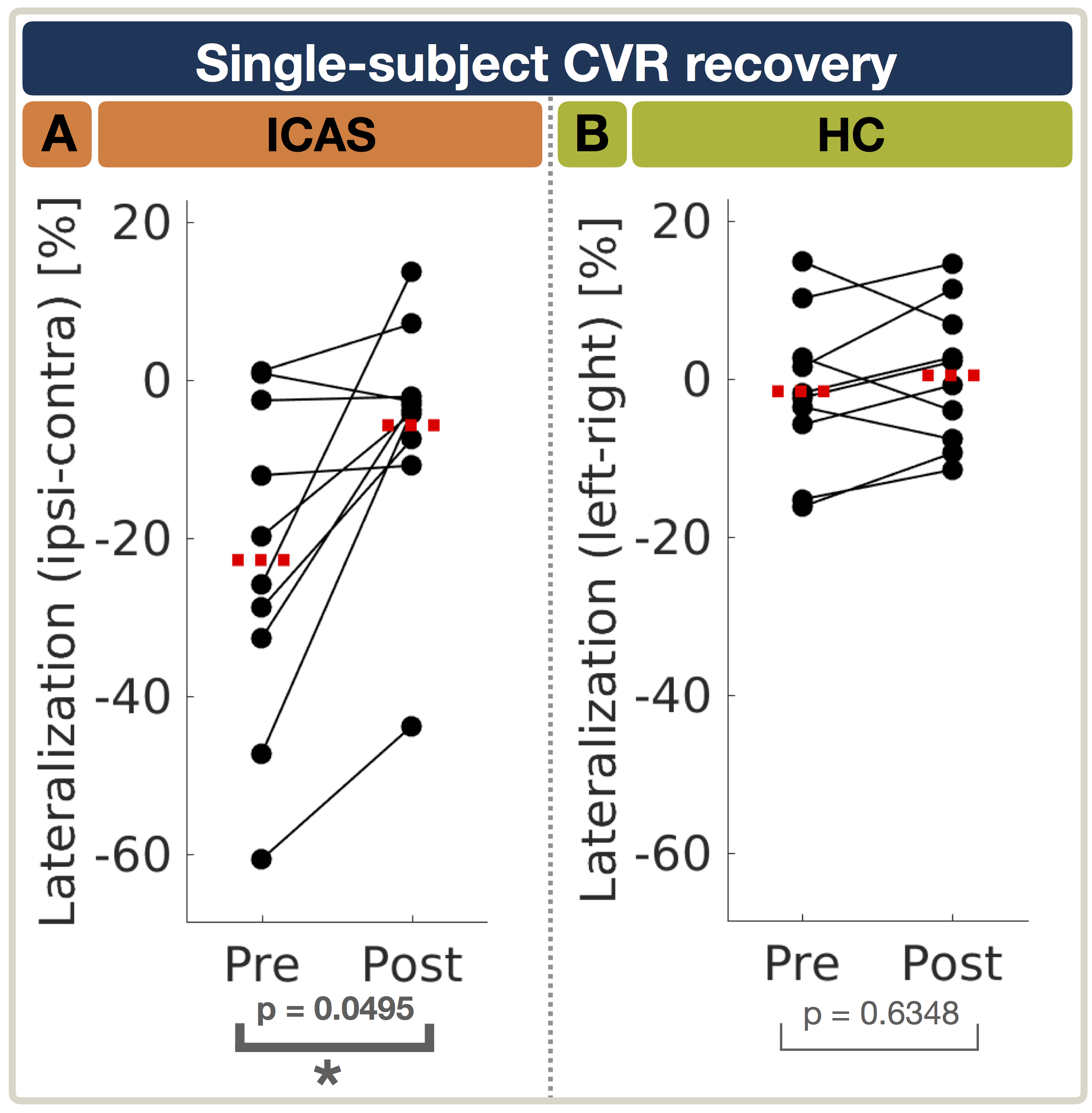
Exemplary data of an ICAS-patient shows decreased CVR before treatment ipsilateral to the stenosis which increases closer to hemispherical symmetry after treatment (Fig.2). On group level of ICAS-patients before treatment, CVR was ipsilaterally decreased within GM-gWSA (Fig.2A) showing a significant lateralization (p=0.0038). After treatment, CVR lateralization recovered and did not significantly differ between hemispheres anymore (p=0.25, Fig.2C). rCBV of ICAS-patients was ipsilaterally increased before treatment. After treatment, rCBV lateralization was closer to zero (p=0.08) meaning more symmetrical rCBV-values between hemispheres (data not shown). For HC, CVR, as well as rCBV (data not shown), were symmetrical on group level in both scans (Fig.3B,D). Evaluation of normalized CVR lateralization in ICAS-patients before and after treatment revealed statistically significant convergence of ipsilateral and contralateral CVR (2-sample T-Test: p=0.0495) towards more symmetrical CVR-values between hemispheres (Fig.4A). HC showed no significant CVR lateralization differences between both scans (Fig.4B, 2-sample T-Test: p=0.6348).Discussion
As hypothesized, the BH-fMRI based evaluation of CVR lateralization within gWSA’s was found to be sensitive to detect subtle CVR impairments of asymptomatic ICAS, without compromising the specificity as affirmed by symmetrical HC results (Fig.3,4). Decreased CVR along with increased rCBV ipsilateral to the stenosis before treatment is assumed to indicate chronic vasodilation.8 Consistent with current literature, CVR recovery was measured after ICAS-treatment.5,8-10 More symmetrical CVR after treatment is thought to be related to improved hemodynamic status. Reversible CVR impairments after treatment together with more symmetrical rCBV might indicate hemodynamic improvements by reduced chronic vasodilation.
On the methodological side, data-driven BH-fMRI was applied in unilateral ICAS-patients assuming benign contralateral regions and only minor changes to the contralateral CVR by the treatment. An advantage of CVR-imaging in comparison with ASL, which was found to be impaired in ICAS, too,20,21 is the applicability to patients after CAS. Gas manipulation with endtidal CO2 measurements are expected to give quantitatively more accurate results and allow lateralization analysis also in case of contralateral CVR changes following treatment.5-7,9-11 However, breath-holds remain a viable alternative as they are much more tolerable and easily applicable at low costs within clinically feasible scan times.7
Conclusion
We have successfully analyzed hemodynamic impairments and their recovery after treatment in ICAS-patients by means of the analysis of non-invasive BH-fMRI in gWSA's. In accordance with current literature, our results show lateralization of CVR before ICAS-treatment and CVR recovery after treatment - pointing to a potential application of BH-fMRI based CVR-imaging. Even deeper insights to CVR recovery could be facilitated by applying individual watershed areas, based on already acquired DSC-data and accounting for individual vascular configurations.13 For the next step, we currently evaluate data from cognitive testing,21 to investigate the link between CVR recovery and clinical outcome5.Acknowledgements
The authors acknowledge support by the Friedrich-Ebert-Stiftung, Dr.-Ing. Leonhard-Lorenz-Stiftung, the German research Foundation (DFG, grant PR 1039/6-1) and Ronja Berg from TUM.References
1. Petty GW et al. (1999). "Ischemic stroke subtypes: a population-based study of incidence and risk factors." Stroke, 30: 2513-6.
2. Demirel SD et al. (2018). "Comparison of long-term results of carotid endarterectomy for asymptomatic carotid artery stenosis. " Gefasschirurgie, 23(Suppl 1): p. 1-7.
3. Alberts MJ (2015). "Carotid stenting—why treating an artery may not treat the patient." JAMA Neurology, 72(3): p. 263-264.
4. Jalbert JJ et al. (2015). "Outcomes after carotid artery stenting in medicare beneficiaries, 2005 to 2009." JAMA Neurology, 72(3): p. 276-286. 8. Alberts MJ (2015). "Carotid stenting—why treating an artery may not treat the patient." JAMA Neurology, 72(3): p. 263-264.
5. Mandell DM et al. (2011). "Quantitative measurement of cerebrovascular reactivity by blood oxygen level-dependent MRimaging in patients with intracranial stenosis: preoperative cerebrovascular reactivity predicts the effect of extracranial-intracranial bypass surgery." AJNR, 32(4):721-7.
6. Liu P et al. (2018). "Cerebrovascular reactivity (CVR) MRI with CO2 challenge: A technical review." Neuroimage, Epub ahead of print.
7. Pillai JJ and Mikulis DJ (2014). "Cerebrovascular Reactivity Mapping: An Evolving Standard for Clinical Functional Imaging." Am J of Neurorad, 36(1):7- 13.
8. Vagal AS et al. (2009). "The Acetazolamide Challenge: Techniques and Applications in the Evaluation of Chronic Cerebral Ischemia." AJNR, 30(5):p. 876-88.
9. Sam K et al. (2015). "Assessing the effect of unilateral cerebral revascularisation on the vascular reactivity of the non-intervened hemisphere: a retrospective observational study." BMJ open, 5(2):e006014.
10. Fierstra J et al. (2011). "Surgical Revascularization Reverses Cerebral Cortical Thinning in Patients With Severe Cerebrovascular Steno-Occlusive Disease". Stroke, 42(6):1631-7.
11. Han JS et al. (2011)."Impact of Extracranial−Intracranial Bypass on Cerebrovascular Reactivity and Clinical Outcome in Patients With Symptomatic Moyamoya Vasculopathy." Stroke, 42(11):3047-54.
12. Momjian-Mayor I. and Baron JC (2005). "The pathophysiology of watershed infarction in internal carotid artery disease: review of cerebral perfusion studies." Stroke, 36(3): p. 567-77.
13. Kaczmarz S et al. (2018). "Increased variability of watershed areas in patients with high-grade carotid stenosis." Neurorad, 60(3): p. 311-323.
14. Jespersen SN and Ostergaard L (2012). "The roles of cerebral blood flow, capillary transit time heterogeneity, and oxygen tension in brain oxygenation and metabolism." JCBFM, 32(2): p. 264-77.
15. Leenders KL (1994). "PET: blood flow and oxygen consumption in brain tumors." J Neurooncol, 22(3): p. 269-73.
16. Vondrácková L et al. (2016). "Data-driven model for evaluation of cerebrovascular-reserve measurement with hypercapnia BOLD." Proc. Intl. Soc. Mag. Reson. Med. 24 (2016): 3801.
17. Statistical Parametric Mapping software (SPM12) Version 6225: www.fil.ion.ucl.ac.uk/spm.
18. MATLAB and Statistics Toolbox Release 2016b, The MathWorks, Inc., Natick, Massachusetts, United States.
19. Vinci software, Max-Planck-Institut für neurologische Forschung, Cologne, Germany: http://www.nf.mpg.de/vinci3/. Accessed 09.Nov 2015.
20. Bouvier J et al. (2015). "Reduced CMRO2 and cerebrovascular reserve in patients with severe intracranial arterial stenosis: A combined multiparametric qBOLD oxygenation and BOLD fMRI study." HBM, 36: 695-706.
21. Goettler J et al. (2018). "The stronger one-sided relative hypoperfusion, the more pronounced ipsilateral spatial attentional bias in patients with asymptomatic carotid stenosis. " JCBFM, in press.
22. Bland-Altman and Correlation Plot software, Ran Klein 2010: http://www.mathworks.com/matlabcentral/fileexchange/45049-bland-altman- and-correlation-plot. Assessed Nov 9th 2015.
Figures