0738
Impaired blood-brain barrier function in pediatric sickle cell disease1Department of Radiology, Johns Hopkins University, Baltimore, MD, United States, 2Department of Biomedical Engineering, Johns Hopkins University, Baltimore, MD, United States, 3Kennedy Krieger Institute, Baltimore, MD, United States, 4Department of Pediatric Hematology, Johns Hopkins University, Baltimore, MD, United States
Synopsis
Sickle cell disease (SCD) is associated with endothelium dysfunction, but the role of the blood-brain barrier (BBB) in SCD has not been evaluated. We evaluated BBB function in pediatric SCD using a novel non-invasive method, water-extraction-with-phase-contrast-arterial-spin-tagging (WEPCAST) MRI. Children with SCD showed lower water extraction compared with healthy individuals. Higher permeability-surface-area-product (PS), i.e. leaky BBB, was associated with a number of known abnormalities in SCD, including lower hematocrit, lower hemoglobin, higher HbS fraction, impaired cognition, and a higher risk for silent cerebral infarction. Collectively, these findings support a potential role for BBB dysfunction in SCD pathogenesis.
INTRODUCTION
Sickle cell disease (SCD) comprises a group of inherited red blood cell (RBC) disorders, in which deoxygenated hemoglobin S (HbS) molecules form polymers and deform RBCs1. SCD has been associated with higher stroke rate2,3 and increased risk of neurodevelopmental disorders4. Previous studies have shown inflammation and endothelium dysfunction in SCD5,6, which suggests a potential role of blood-brain-barrier (BBB) permeability in the pathogenesis of brain injury in SCD; however, human studies of BBB function in SCD are scarce, due to a lack of non-invasive techniques, especially for SCD children, in whom hypertonic contrast-agent administration is not desirable. Recently, a water-extraction-with-phase-contrast-arterial-spin-tagging (WEPCAST) MRI technique was developed for the assessment of BBB permeability without contrast agents7. In this study, we applied this novel technique to evaluate BBB function in SCD children. The relationships between BBB permeability and hematological measures, presence of silent cerebral infarction (SCI), and neuropsychological scores were examined.METHODS
Participants
Eight participants with SCD were recruited (10.3±0.9years, 5F/3M). Five of them have SCD subtype Hemoglobin SS, two have Hemoglobin Sβ+ and one has Hemoglobin SC. Six of the subjects receive hydroxyurea treatment and none receive chronic transfusions.
MRI Experiments
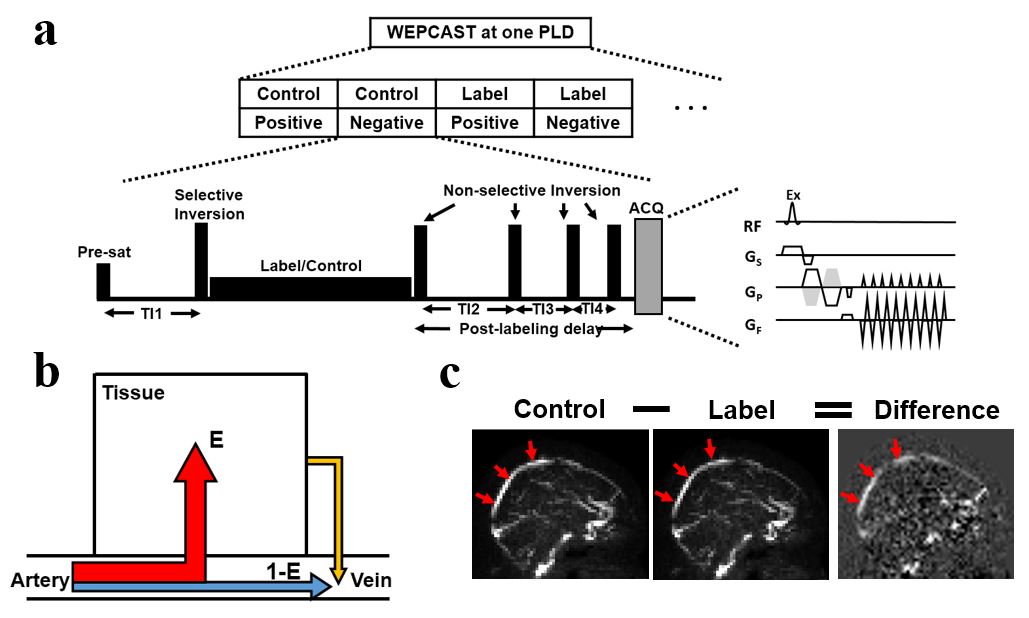
WEPCAST MRI (figure 1) is a novel MRI technique which estimates water extraction fraction (E) by selectively measuring ASL signal in large veins, e.g. superior-sagittal-sinus (SSS)7. Together with global cerebral blood flow (CBF, f), BBB permeability can be estimated in terms of permeability-surface-area product (PS): $$$PS=-ln(1-E)\times f$$$.
All subjects were studied on a 3T Philips System. WEPCAST MRI was performed in mid-sagittal plane, with a labeling duration of 2000ms, post-labeling delay of 3000ms and encoding velocity of 15cm/s. ROIs were drawn in SSS and E was calculated based on the resulting signal. Global CBF was obtained by phase-contrast MRI, and then PS was quantified. Details of WEPCAST analysis are described in Lin et al7.
T2-FLAIR images were acquired and evaluated by a board-certified radiologist, from which an index of SCI was obtained.
Hematological and neuropsychological evaluations
Hematocrit, hemoglobin concentration, and hemoglobin S fraction were determined. A battery of neuropsychological tests was performed, including Wechsler Intelligence Scale for Children (WISC-V), Conners’ Continuous Performance Test (CPT-III), Behavior Rating Inventory of Executive Function (BRIEF-2) and Vineland Adaptive Behavior Scales (Vineland-II).
Statistical analysis
WECPAST results from six healthy young adults (23.2±2.9years, 3F/3M) were used as control data. Two sample t-test was performed to compare E and PS between SCD children and healthy adults.
Within the SCD patients, we further examined the relationship between BBB permeability measures (E and PS) and hematological parameters, presence of SCI, and neuropsychological scores. Age and sex were covariates and included in the model in a step-wise manner, if significant.
RESULTS AND DISCUSSION
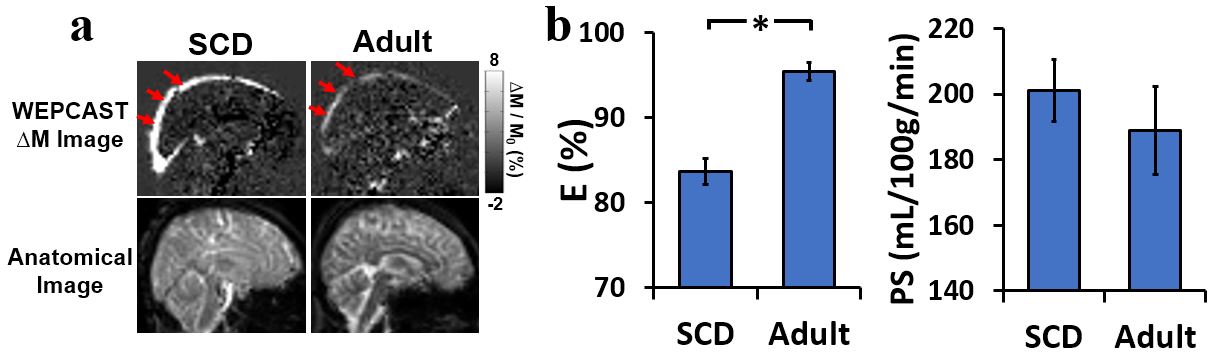
Figure 2a shows representative WEPCAST images for a SCD child. Compared with healthy adult, SCD child revealed significant higher signal in SSS. Group-level comparisons of quantitative WEPCAST indices (Figure 2b) revealed that SCD children had significantly lower water extraction fraction (SCD E: 83.7±4.4%, adults E: 95.5±2.6%, p<0.001) and slightly higher, but not statistically significant, PS (SCD: 201.0±26.8mL/100g/min, adults: 188.9±32.7mL/100g/min, p>0.05), compared to healthy adults.
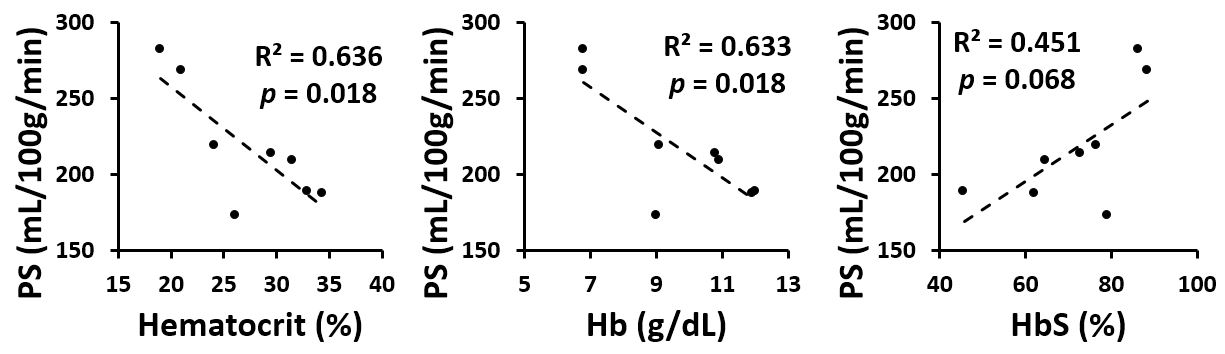
Among SCD patients, higher PS was associated with significantly lower hematocrit level (p=0.018) and lower hemoglobin (p=0.018) (Figure 3). There was also a trend of positive association between PS and hemoglobin S level (p=0.068). These findings suggest that BBB disruption was more significant in more severe SCD subtypes.
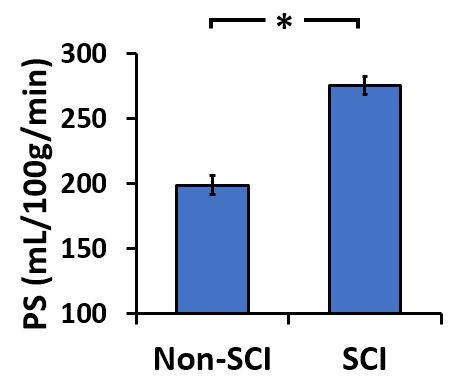
Furthermore, higher PS was significantly associated with a greater risk of SCI (PS in non-SCI: 198.5±7.4mL/100g/min, PS in SCI: 275.3±7.1mL/100g/min, p=0.002, Figure 4). BBB disruption has been associated with vessel disorganization and ischemia8, consistent with our observation that SCD patients with a leaky BBB tend to have a high risk of infarction.
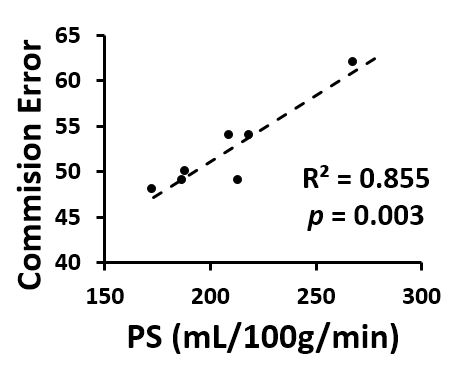
Finally, regression analysis showed that PS had a positive association with commission error t-score in CPT-III (p=0.003, Figure 5), suggesting that BBB leakage in SCD may lead to attention deficits.
CONCLUSION
To our knowledge, this study is the first to examine BBB permeability in pediatric SCD. Our findings support two recent reports that SCD patients showed a lower global water extraction fraction compared to healthy individuals9,10; however, our data suggest that this is primarily due to a higher CBF in these patients, and not attributable to a lower global PS. In contrast, our data suggest that PS in SCD patients is greater compared to healthy individuals. Furthermore, higher PS was associated a number of known abnormalities in SCD, including lower hematocrit, lower hemoglobin, higher HbS fraction, worse cognition, and a higher risk for silent infarction. Collectively, these findings support a potential role for BBB dysfunction in SCD pathogenesis.Acknowledgements
No acknowledgement found.References
1. Kassim AA, DeBaun MR. Sickle cell disease, vasculopathy, and therapeutics. Annu Rev Med 2013;64:451-466.
2. Lance EI, Comi AM, Johnston MV, Casella JF, Shapiro BK. Risk Factors for Attention and Behavioral Issues in Pediatric Sickle Cell Disease. Clin Pediatr (Phila) 2015;54:1087-1093.
3. Fullerton HJ, Wu YW, Zhao S, Johnston SC. Risk of stroke in children: ethnic and gender disparities. Neurology 2003;61:189-194.
4. Berkelhammer LD, Williamson AL, Sanford SD, Dirksen CL, Sharp WG, Margulies AS, Prengler RA. Neurocognitive sequelae of pediatric sickle cell disease: a review of the literature. Child Neuropsychol 2007;13:120-131.
5. Hebbel RP, Osarogiagbon R, Kaul D. The endothelial biology of sickle cell disease: inflammation and a chronic vasculopathy. Microcirculation 2004;11:129-151.
6. Ghosh S, Tan F, Ofori-Acquah SF. Spatiotemporal dysfunction of the vascular permeability barrier in transgenic mice with sickle cell disease. Anemia 2012;2012:582018.
7. Lin Z, Li Y, Su P, Mao D, Wei Z, Pillai JJ, Moghekar A, van Osch M, Ge Y, Lu H. Non-contrast MR imaging of blood-brain barrier permeability to water. Magn Reson Med 2018;80:1507-1520.
8. Wardlaw JM. Blood-brain barrier and cerebral small vessel disease. J Neurol Sci 2010;299:66-71.
9. Bush A, Chai Y, Choi SY, Vaclavu L, Holland S, Nederveen A, Coates T, Wood J. Pseudo continuous arterial spin labeling quantification in anemic subjects with hyperemic cerebral blood flow. Magn Reson Imaging 2018;47:137-146.
10. Juttukonda MR, Donahue MJ, Davis LT, Gindville MC, Lee CA, Patel NJ, Kassim AA, Pruthi S, Hendrikse J, Jordan LC. Preliminary evidence for cerebral capillary shunting in adults with sickle cell anemia. J Cereb Blood Flow Metab 2017. doi: 10.1177/0271678X17746808:271678X17746808.
Figures