0731
Predicting In Vivo MRI Gradient-Induced Voltage Levels on Deep Brain Stimulation Systems Using Artificial Neural Networks1Restorative Therapies Group, Medtronic, Minneapolis, MN, United States
Synopsis
MRI gradient-fields may cause unintended interactions due to induced voltage potential along elongated conductive components of active implanted medical devices, therefore devices must be tested at clinically-relevant exposure levels. In vivo gradient-induced voltage levels on implanted deep brain stimulation (DBS) systems are simulated in adult human anatomical models. Then, artificial neural network (ANN) models are trained to predict gradient-induced voltages on DBS systems. Predictive ANN models demonstrated good accuracy (RMSE<0.180V). Leave-one-model-out cross-validation results demonstrate that ANN models can perform accurate predictions in general population if a variety of anatomical models representative of the population are included in the training dataset.
Introduction
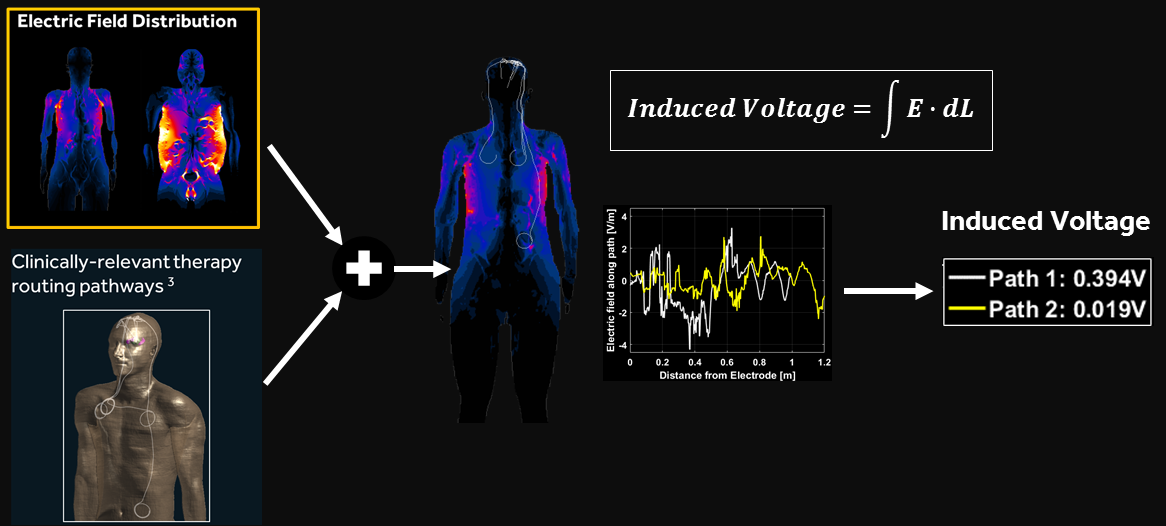
Time-varying MRI gradient-fields may induce voltage potential along elongated conductive structures of active implanted medical device (AIMD) components such as therapy leads. MRI gradient-induced extrinsic voltage levels may cause unintended tissue stimulation and/or device malfunction, therefore AIMDs need to be thoroughly evaluated to assess potential unintended interactions due to induced voltages on therapy leads. To avoid conservative estimations that could limit patient access, accurate and clinically relevant gradient-induced voltage levels are required for testing AIMDs. Anatomically accurate human models such as Virtual Population models [1] are commonly used in the industry to simulate in vivo Electric-field (E-field) exposure due to MRI gradient coils. Then, tangential component of the E-field along clinically relevant AIMD implant pathways are integrated to calculate gradient-induced extrinsic voltage levels as described in Annex A.3.4 “Tier 3 electromagnetic simulation method” in ISO/TS 10974 [2] (Figure 1).
Adding new accurate human body models into the electromagnetic (EM) simulation library can help to reduce conservative assumptions and to determine more clinically relevant test levels, instead of employing conservative assumptions. On the other hand, adding new models into the EM library is time-consuming, expensive and not always feasible.
The goal of this work is to develop a predictive model using artificial neural networks (ANN) to determine in vivo MRI gradient-induced extrinsic voltage levels on implanted Deep Brain Stimulation (DBS) lead-extension components.
Methods
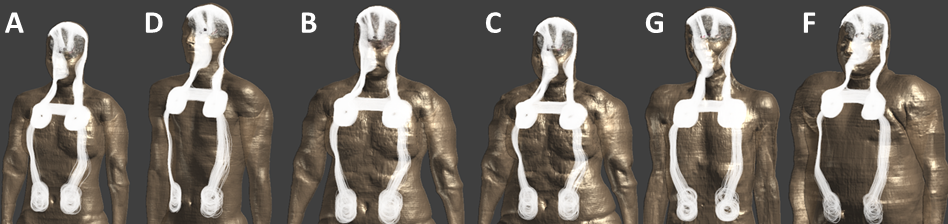
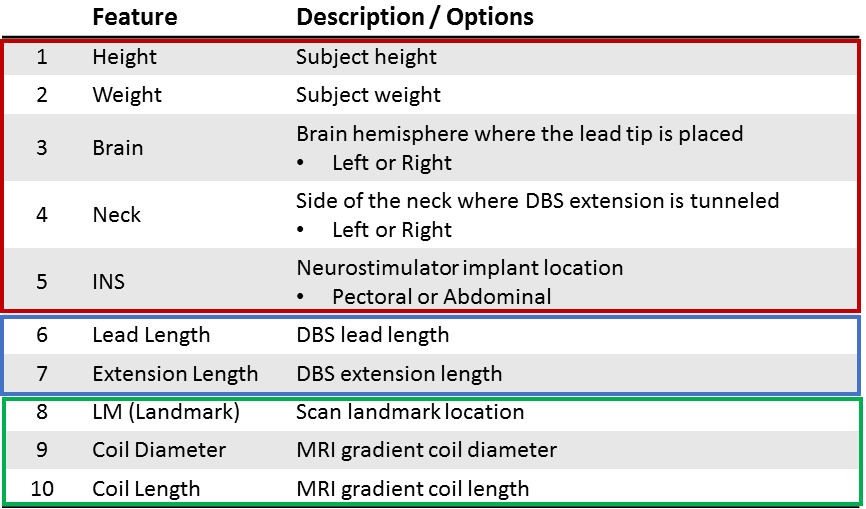
Induced voltage levels along clinically relevant DBS therapy routing pathways (Figure 2) are simulated using a finite-difference time-domain solver (Sim4Life, Zurich MedTech, Zurich, Switzerland) in six anatomically relevant adult human body models [1], inside five different MRI gradient coil models, at scan locations spanning human models from head to ankles at 10 cm increments. More than 100,000 unique induced voltage values are simulated to form the dataset. Induced voltage values are represented using ten features listed in Figure 3, that includes subject-related, implant-related and MRI/scan-related features.
First, the entire dataset was randomly partitioned into training, test and cross-validation sets. An ANN was trained to predict MRI induced voltage values from ten features. ANN hyperparameters were tuned using the test set and ANN performance was evaluated on the cross-validation dataset. Performance of the ANN was compared against multiple linear regression with all first order and selected second order features (second order features used in multiple linear regression were selected using ANOVA, analysis-of-variance method). Model development and evaluations were performed using Python 3.6 and several Python libraries including Keras and Scikit-Learn.
Secondly, leave-one-model-out cross-validation was performed to evaluate the predictive performance of the method on previously unseen body models. This was accomplished by removing one of the human body models from the training set, training the ANN on the remaining five models, then predicting induced voltage values of the body model that was left out from the training set and comparing against true values. This approach was repeated for every unique human body model.
Root-mean-squared error (RMSE) and coefficient of determination (R2) metrics are used to evaluate the performance of linear regression and ANN models.
Results
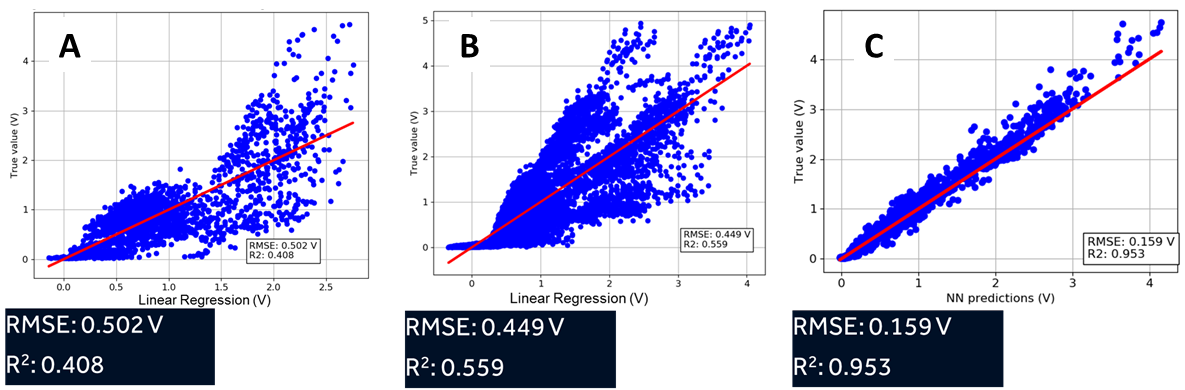
Two-layer ANNs with 80 and 60 units in first and second hidden layers respectively with rectified linear unit (ReLU) activation functions and mean-squared-error cost function are used after hyperparameter tuning. ANN model significantly outperformed multiple linear regression models (Figure 4), with RMSE < 0.16V and R2 > 95%.
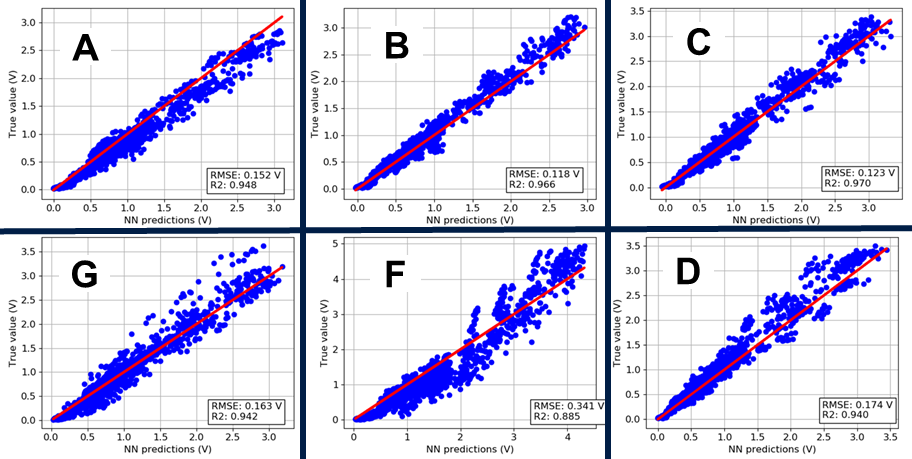
Leave-one-model-out cross-validation results are plotted in Figure 5 for all six body models. ANNs performed exceptionally well with RMSE <0.180V and R2 > 94% for five out of six evaluated human body models. Size of the body model ‘F’ is significantly larger than remainder of the models (weight: 120kg, next heaviest model: 80kg) therefore remainder of the body models are not sufficient to train the ANN for better accuracy in an ‘outlier’ model such as ‘F’. Cross-validation RMSE for model ‘F’ is >0.340V.
Discussion/Conclusion
The ANN model developed herein can be used to predict in vivo MRI gradient-induced extrinsic voltage levels on implanted DBS systems, and to determine AIMD test levels per ISO/TS 10974. Leave-one-model-out cross-validation results suggest that the ANN model can perform accurate predictions in general population as long as a variety of human body models that are representative of the population are included in the training dataset. General methodology described here may be extended to other problems such as RF safety and MRI coil evaluations where EM simulations with human body models are extensively used.Acknowledgements
No acknowledgement found.References
1. Gosselin, Marie-Christine, et al. "Development of a new generation of high-resolution anatomical models for medical device evaluation: the Virtual Population 3.0." Physics in Medicine and Biology. 2014 Aug 21; 59(18): 5287.
2. ISO/TS 10974:2018, “Assessment of the safety of magnetic resonance imaging for patients with an active implantable medical device”.
Figures