0713
Total suicide attempts associated with distinct functional neuroimaging correlates in bipolar disorder1Radiology, University of Iowa, Iowa City, IA, United States, 2Psychiatry, University of Iowa, Iowa City, IA, United States, 3Electrical and Computer Engineering, University of Iowa, Iowa City, IA, United States
Synopsis
Suicidal behavior is a major cause of injury and death in bipolar disorder. We measured the relationship between a history of suicide attempt and brain activation to a flashing checkerboard task in bipolar disorder using functional magnetic resonance imaging (fMRI). We compared activity between suicide attempters and non-attempters and we separately tested the relationship between brain activity and the number of past suicide attempts. These two analyses produced distinct patterns of results that indicated a mood-state independent relationship between suicide attempts and prefrontal and cerebellar activity. These findings suggest that accounting for multiple attempters may strengthen studies of suicidal behavior.
Introduction
Suicidal behavior is a significant elevated in people with bipolar disorder (BD). As many as 40% of people with bipolar disorder attempt suicide and multiple suicide attempts are common.1 Suicide is the cause of death for 15-20% of people with BD. 2 Suicidal behavior is thought to arise as a result of suicidal ideation, which occurs frequently in bipolar disorder combined with other independent factors such as increased impulsive aggression. 3,4 Neuroimaging studies have found reduced prefrontal grey and white matter volume, 5–7 structural changes in corpus callosum, 8–10 reduced volume in limbic structures, 7 reduced prefrontal activity,11 and reduced functional connectivity between limbic, salience, and executive networks in suicide attempters 12 relative to those without a history of suicide attempts.
One of the difficulties in studying suicidal behavior in bipolar
disorder is accounting for the effects of mood state. Here we extend previous
findings using a sample of participants in different mood states in order to identify
mood-state independent biological risk factors for suicidal behavior. Furthermore,
we investigate differences between the use of a contrast between previous
suicide attempters vs. non-attempters and the use of total previous suicide
attempts as a continuous variable.
Methods
39 participants with bipolar disorder underwent functional magnetic resonance imaging (fMRI) during a flashing checkerboard paradigm using a 3T Siemens Tim Trio system. Imaging parameters have been previously reported.13,14 Participants’ history of suicidal behavior and ideation was assessed through clinical interview and with relevant items from the Schedule for Affective Disorders and Schizophrenia. fMRI pre-processing was performed including skull stripping, despiking, smoothing, and anatomical image co-registration using Analysis of Functional Neuroimages (AFNI) software.15 Percent signal change maps were generated for the contrast between flashing checkerboard and rest blocks in common atlas space.
Multiple regression was used to compare functional activity between participants with at least one suicide attempt and non-attempters and to test the relationship between functional activity and total suicide attempts. Age, sex, and current mood state were included as covariates and voxels where there was no significant difference between the experimental and null regression models were excluded. Multiple comparisons correction was performed using a false discovery rate of 0.05.
Results
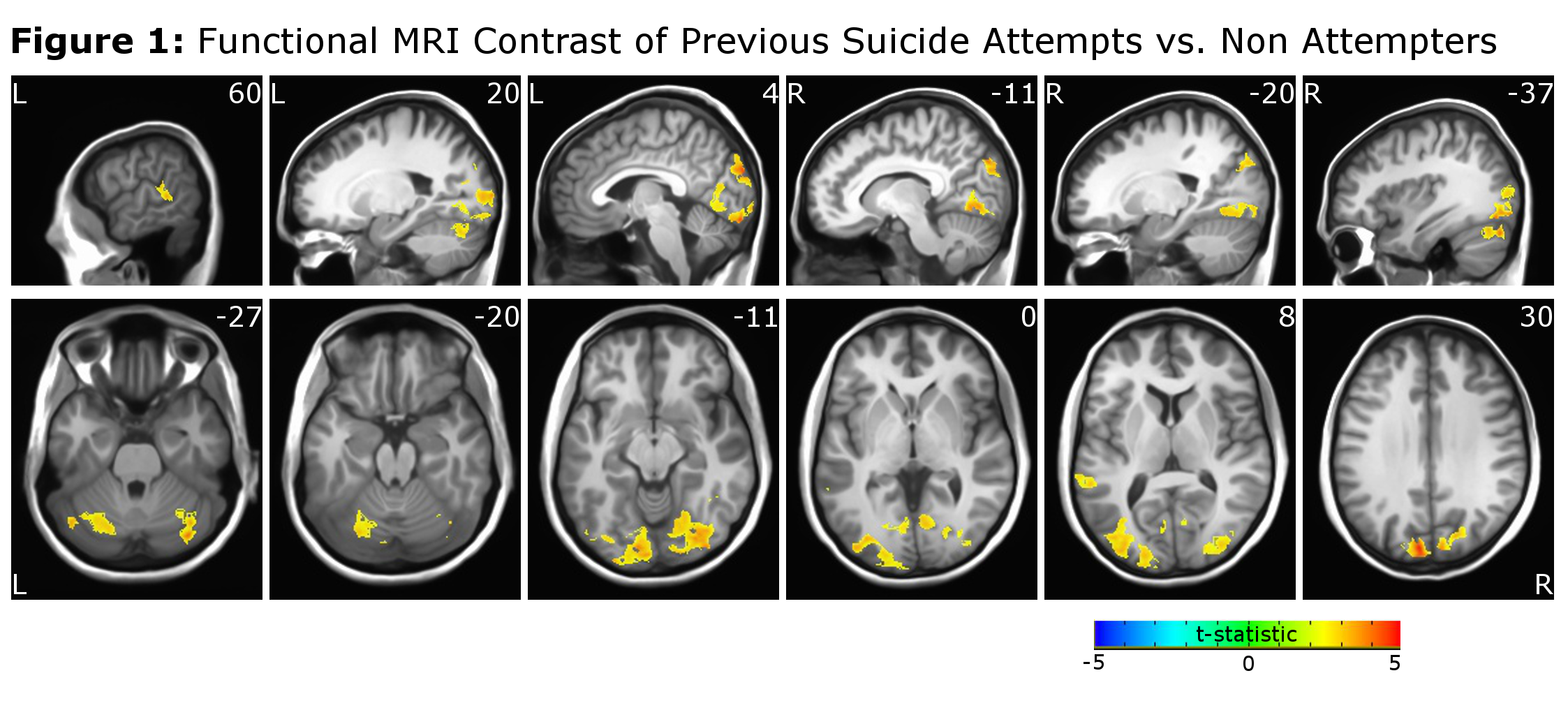
Previous suicide attempters had an increased functional response to the flashing checkerboard in visual areas, left superior temporal cortex, and cerebellum (Figure 1).
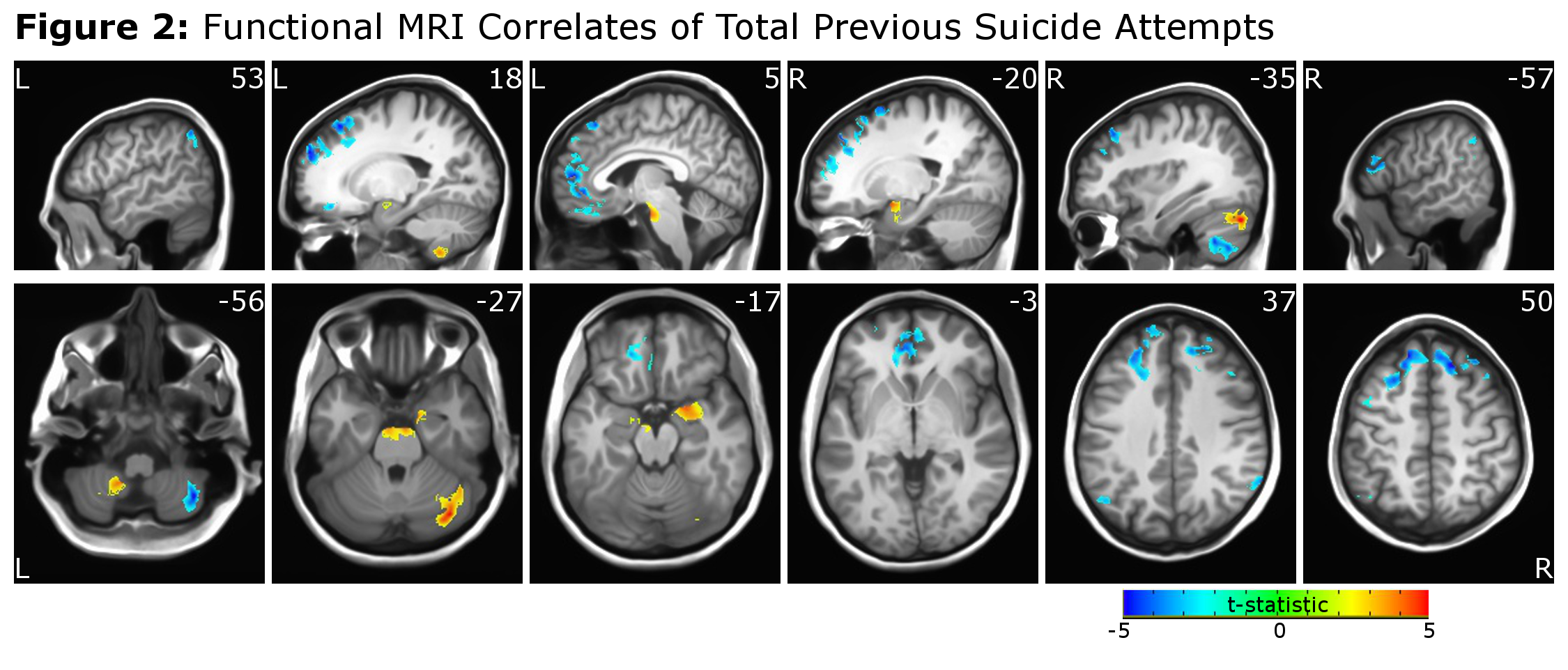
When total previous suicide attempts was treated as a continuous variable, a greater number of suicide attempts was associated with an increased functional response to the flashing checkerboard stimulus in right amygdala, bilateral cerebellum, and superior pontine nuclei. A reduced functional response was also present in medial and dorsolateral prefrontal cortex, lateral parietal cortex, and portions of the right cerebellum (Figure 2).
Discussion
Despite the relatively simple nature of the flashing checkerboard paradigm, functional activity differences were present in participants with a history of suicide attempt in brain regions involved in executive function,16 attention,17 and emotional control 18,19 in a manner suggesting trait differences (i.e. unrelated to mood state) may be associated with a history of suicide attempt in bipolar disorder. Functional differences in these regions have been previously reported in bipolar disorder 20 and have been shown to be related to suicidal behavior;7,11 however our findings add a role for the cerebellum. This novel finding supports prior literature of an important role for the cerebellum in emotional regulation. 21,22
We also found that the use of total previous attempts as a continuous variable revealed a pattern of functional alterations that was distinct from when we compared suicide attempters with non-attempters. These distinct patterns suggest that the contrast between previous attempters and non-attempters may not fully capture the spectrum of vulnerability to suicidal behavior and that the use of either additional groups (e.g. multiple attempters, single attempters, non-attempters) or the use of total previous attempts as a continuous variable may be more useful to test the relationship between functional imaging and suicide history.
Conclusion
Our findings suggest that a history of suicide attempt in bipolar disorder is associated with trait alterations in functional activity, however the measurement of these differences is strongly affected by whether suicide history is treated as a binary (attempters vs. non-attempters) or continuous variable (total attempts). This finding may complicate the interpretation of previous studies of suicidal behavior in bipolar disorder and also informs future research. Investigators should consider whether prior suicidal behavior is best conceptualized as a distinct group of individuals or a dimensional measure of vulnerability to these behaviors and suicide risk.Acknowledgements
No acknowledgement found.References
1. MacKinnon, D. F. et al. Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord. (2005). doi:10.1111/j.1399-5618.2005.00236.x
2. Latalova, K., Kamaradova, D. & Prasko, J. Suicide in bipolar disorder: A review. Psychiatria Danubina (2014).
3. Mann, J. J., Waternaux, C., Haas, G. L. & Malone, K. M. Toward a clinical model of suicidal behavior in psychiatric patients. Am. J. Psychiatry (1999). doi:10.1176/ajp.156.2.181;pageGroup:string:Publication
4. Brent, D. A. & Mann, J. J. Family genetic studies, suicide, and suicidal behavior. American Journal of Medical Genetics - Seminars in Medical Genetics (2005). doi:10.1002/ajmg.c.30042
5. Lijffijt, M., Rourke, E. D., Swann, A. C., Zunta-Soares, G. B. & Soares, J. C. Illness-course modulates suicidality-related prefrontal gray matter reduction in women with bipolar disorder. Acta Psychiatr. Scand. (2014). doi:10.1111/acps.12314 6. Benedetti, F. et al. Opposite effects of suicidality and lithium on gray matter volumes in bipolar depression. J. Affect. Disord. (2011). doi:10.1016/j.jad.2011.07.006
7. Johnston, J. A. Y. et al. Multimodal neuroimaging of frontolimbic structure and function associated with suicide attempts in adolescents and young adults with bipolar disorder. Am. J. Psychiatry 174, 667–675 (2017).
8. Matsuo, K. et al. Anterior genu corpus callosum and impulsivity in suicidal patients with bipolar disorder. Neurosci. Lett. (2010). doi:10.1016/j.neulet.2009.11.047
9. Gifuni, A. J. et al. Corpus callosum volumes in bipolar disorders and suicidal vulnerability. Psychiatry Res. - Neuroimaging (2017). doi:10.1016/j.pscychresns.2017.02.002
10. Cyprien, F. et al. Corpus callosum integrity is affected by mood disorders and also by the suicide attempt history: A diffusion tensor imaging study. J. Affect. Disord. (2016). doi:10.1016/j.jad.2016.07.026
11. Hirose, T., Tsujii, N., Mikawa, W. & Shirakawa, O. Delayed hemodynamic responses associated with a history of suicide attempts in bipolar disorder: a multichannel near-infrared spectroscopy study. Psychiatry Res. - Neuroimaging (2018). doi:10.1016/j.pscychresns.2018.08.003
12. Cáceda, R., Bush, K., James, G. A., Stowe, Z. N. & Kilts, C. D. Modes of resting functional brain organization differentiate suicidal thoughts and actions: A preliminary study. J. Clin. Psychiatry (2018). doi:10.4088/JCP.17m11901
13. Shaffer, J. J. et al. Impaired sensory processing measured by functional MRI in Bipolar disorder manic and depressed mood states. Brain Imaging Behav. (2017). doi:10.1007/s11682-017-9741-8
14. Shaffer, J. J. et al. Relationship altered between functional T1ρ and BOLD signals in bipolar disorder. Brain Behav. 7, e00802 (2017).
15. Cox, R. W. AFNI: Software for analysis and visualization of functional magnetic resonance neuroimages. Comput. Biomed. Res. (1996). doi:10.1006/cbmr.1996.0014
16. Funahashi, S. & Andreau, J. M. Prefrontal cortex and neural mechanisms of executive function. J. Physiol. Paris (2013). doi:10.1016/j.jphysparis.2013.05.001
17. Posner, M. I. & Petersen, S. E. The attention system of the human brain. Annu. Rev. Neurosci. 13, 25–42 (1990).
18. Banks, S. J., Eddy, K. T., Angstadt, M., Nathan, P. J. & Luan Phan, K. Amygdala-frontal connectivity during emotion regulation. Soc. Cogn. Affect. Neurosci. 2, 303–312 (2007).
19. Strakowski, S. M. et al. The functional neuroanatomy of bipolar disorder: A consensus model. Bipolar Disorders 14, 313–325 (2012).
20. Strakowski, S. M., DelBello, M. P. & Adler, C. M. The functional neuroanatomy of bipolar disorder: A review of neuroimaging findings. Molecular Psychiatry 10, 105–116 (2005).
21. Schmahmann, J. D. & Caplan, D. Cognition, emotion and the cerebellum. Brain : a journal of neurology 129, 290–292 (2006).
22. Stoodley, C. J. & Schmahmann, J. D.
Evidence for topographic organization in the cerebellum of motor control versus
cognitive and affective processing. Cortex 46, 831–844 (2010).
Figures