0710
MRI assessed dysmotility and texture analysis in the terminal ileum and small bowel: A pilot study comparison between Irritable Bowel Syndrome (IBS) patients with bloating and healthy controls1CMI, UCL, London, United Kingdom, 2Department of Gastroenterology, University College London Hospitals, London, United Kingdom
Synopsis
Gastrointestinal symptoms in irritable bowel syndrome (IBS) occur without any obvious structural gut abnormality. This pilot study is based on abnormal ileo-caecal motility function suggested by wireless capsule data, with potential reflux of caecal contents back into the terminal ileum (TI). We compared constipation-predominant IBS (IBS-C) patients with bloating to healthy controls, through texture analysis and motility measures. We found TI temporal variation of motility was significantly higher in healthy controls. There was also a difference in the TI to small bowel texture analysis contrast ratio, but this was only significant in BTFE sequences.
Introduction
Irritable bowel syndrome (IBS) manifests with recurrent gastrointestinal symptoms including abdominal pain, bloating, constipation and/or diarrhoea, in the absence of any demonstrable structural gut abnormality1. Disturbed motility is postulated as a key cause of symptoms. Wireless motility capsule studies suggest abnormal ileo-caecal motility in some IBS patients, with reflux of caecal contents into the terminal ileum2. Anecdotally, radiologists also report “faecalisation” of terminal ileum luminal content on MRI performed in patients with IBS-C.
MRI is increasingly established as a powerful non-invasive tool to study bowel structure, content, and function (motility). It may therefore be a useful biomarker of IBS, aide in phenotyping patients more accurately and increase our understanding of its pathophysiology.
The purpose of this study was to investigate whether MRI can demonstrate differences in enteric motility and terminal ileum luminal content between IBS patients with abdominal bloating (IBS-C) and healthy controls (HCs). Specifically, we investigated texture analysis and motility derived measures.
Methods
Subjects: 15 IBS patients with abdominal bloating and 20 HCs underwent MR enterography.
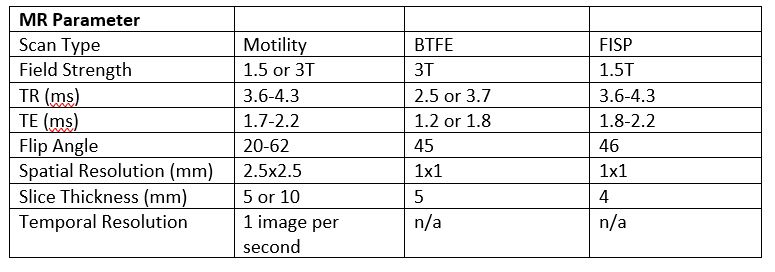
Scanning: Motility was imaged using a cine series of 2D coronal, balanced gradient sequences acquired during breath-holds to cover the whole small bowel (SB) volume using routine motility imaging parameters3. Anatomical images were also acquired using balanced sequences at a higher spatial resolution (figure 1).
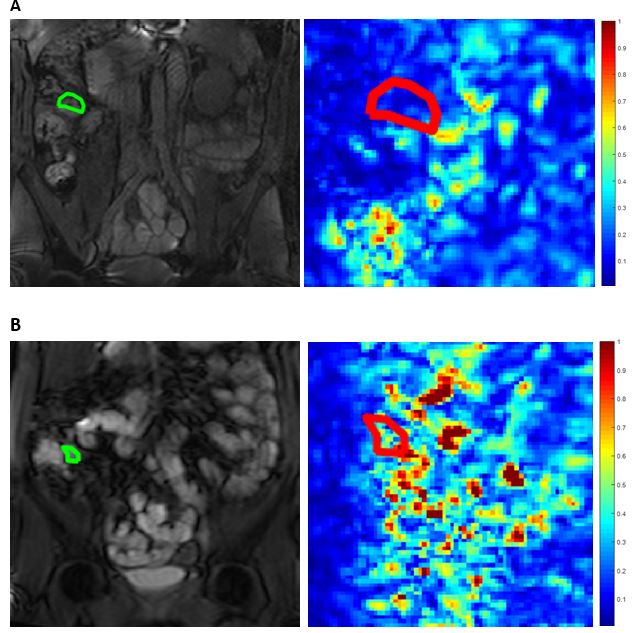
Motility Analysis: For each 2D cine sequence the frames were registered using an optic-flow based registration technique4. A motility map and a temporal variation map (figure 2) both summarising the variations in local expansion and contraction on a per pixel basis were calculated from the standard deviation of the Jacobian determinant of the deformation fields.
A total of 4 motility metrics were developed for the TI; 1) mean motility, 2) spatial variation (variability across ROI), 3) temporal variation (variability over time), 4) area of motile bowel.
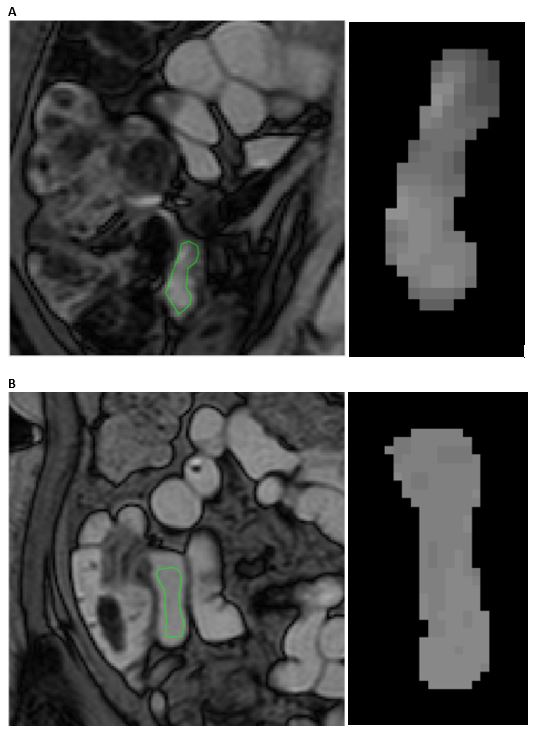
Texture Analysis: 2 ROIs of identical shape and size were drawn on anatomical images: 1) in the TI and 2) in an oral contrast filled region of small bowel.
Gray level co-occurrence matrices (GLCMs) were calculated in 4 directions and for pixel distances from 1-4 using 32 gray levels. 3 summary measures were derived for each GLCM: 1) contrast, 2) energy and 3) homogeneity and then averaged for the 4 directions, providing 12 texture analysis measures per subject.
For each summary measure, the ratio between the TI and the SB was calculated at each of the 4 pixel distances.
Statistical analysis: For both motility and texture analysis, a Student’s t-test was used to compare IBS patients and HCs.
Results
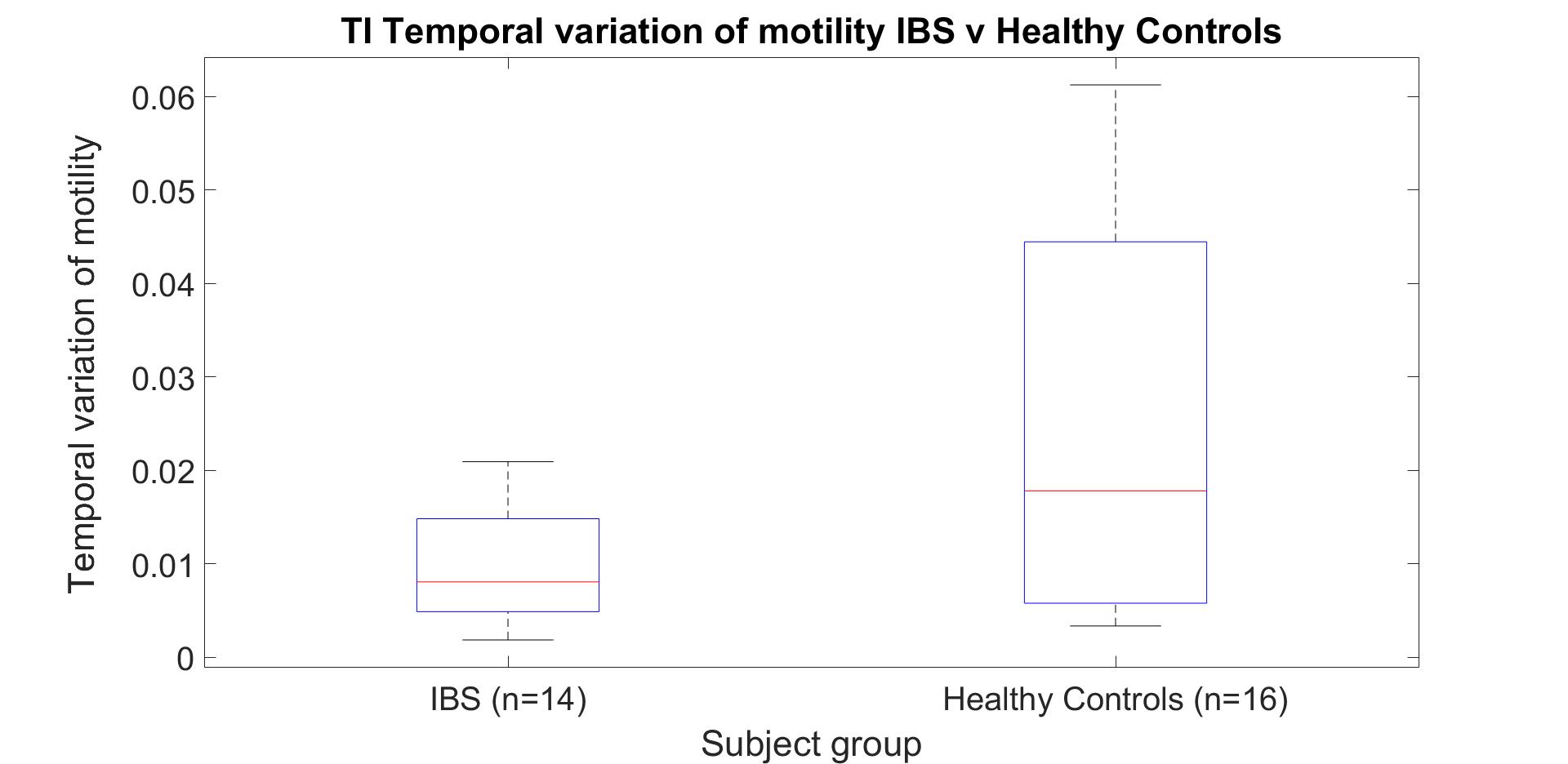
The TI temporal variation (metric 3) was significantly higher (P= 0.02) in HCs (mean = 0.024, n=16) than IBS patients (mean = 0.010, n=14) (figure 3). There were no significant differences for metric 1 (P = 0.10), metric 2 (P = 0.14) or metric 4 (P=0.36).
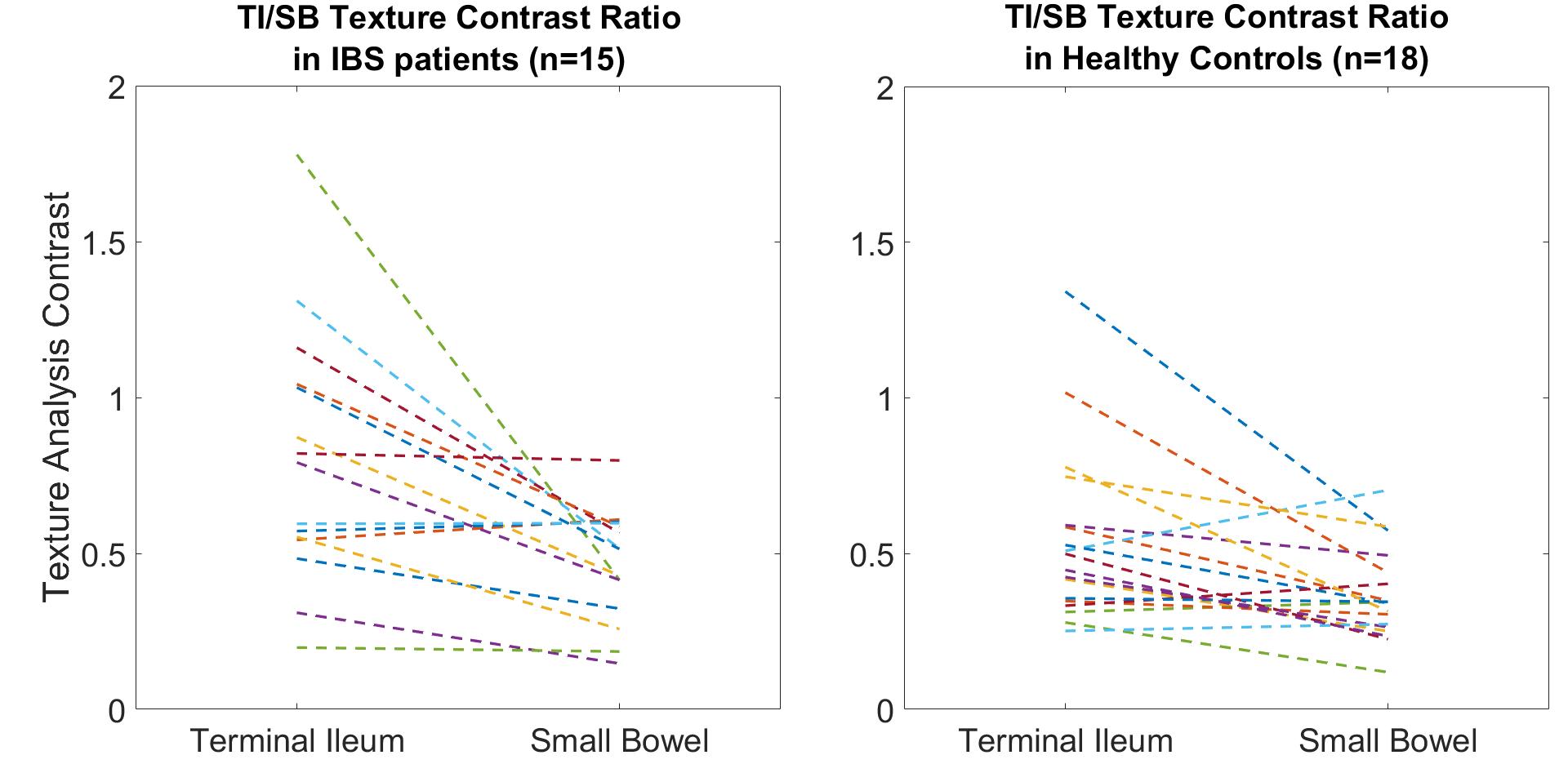
The best texture analysis measure to discriminate between the two subject groups was contrast at a pixel distance of 1 pixel (figure 4). The ratio of TI to SB (TI/SB ratio) was higher in IBS patients (mean ratio = 1.82, n=15) than HCs (mean ratio = 1.56, n=18), but this did not reach significance (P = 0.32) (figure 5).
Discussion
In this pilot study we demonstrated higher temporal variability of motility in healthy controls. This suggests that symptoms in IBS could in part be caused by aberrant terminal ileum motility, being consistently switched “on” or “off”. This would affect transit of luminal contents from the terminal ileum into the colon and is a plausible explanation for the observation of caecal-ileal reflux using wireless motility capsule. Altered motility and TI filling may cause aberrant viscero-somatic reflexes, resulting in abdominal bloating.
A higher TI/SB contrast ratio in IBS suggests a mixture of bowel contents in the TI, including possible faecal reflux from the colon compared to more homogeneous SB mannitol filling as part of MRE protocols in healthy controls. In this small pilot study we were unable to detect a significance difference between HCs and IBS. Data were acquired from multiple scanners and a significant contrast-ratio difference was observed in a sub-set of 4 patients from one scanner. Further investigation is required to optimise scan parameters for differentiating between intestinal contents.
Conclusion
Low motility temporal variation in the terminal ileum could potentially be a biomarker for bloated IBS patients. Texture analysis shows promise in its ability to differentiate between various luminal contents. Optimisation of sequences to increase sensitivity to luminal contents may lead to a more robust detection of differences using texture analysis.Acknowledgements
This work is supported by the EPSRC-funded UCL Centre for Doctoral Training in Medical Imaging (EP/L016478/1) and the Department of Health’s NIHR-funded Biomedical Research Centre at (University College London Hospital)
References
- Drossman, D. A. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features, and Rome IV. Gastroenterology 150, 1262–1279.e2 (2016).
- Camilleri, M. et al. Wireless pH-motility capsule for colonic transit: prospective comparison with radiopaque markers in chronic constipation. Neurogastroenterol. Motil. 22, 874-e233 (2010).
- Naziroglu, R. E. et al. Semi-automatic bowel wall thickness measurements on MR enterography in patients with Crohn’s disease. Br. J. Radiol. 90, 20160654 (2017).
- Odille, F. et al. Quantitative assessment of small bowel motility by nonrigid registration of dynamic MR images. Magn. Reson. Med. 68, 783–793 (2012).
Figures