0708
Hyperpolarized 13C MRI of Patients with Metastatic Prostate Cancer to Bone and Liver1Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 2School of Medicine, University of California, San Francisco, San Francisco, CA, United States
Synopsis
In this feasibility study, hyperpolarized 13C-pyruvate MR exams were conducted on 5 patients who had metastatic prostate cancer to bone or liver. In one man with liver metastasis, serial scans showed a decrease of pyruvate-to-lactate conversion kPL (0.026 to 0.015 s-1) at 2 months after initiation of chemotherapy that was consistent with response based on PSA and RECIST criteria. High kPL was found in patients with bone lesions comparable to that in high-grade primary prostate cancer. Overall, HP-13C MR imaging showed great promise as a biomarker to evaluating treatment responses in metastatic prostate cancer.
Purpose
Prostate cancer is a major health concern in the United States with more than 160,000 new diagnoses and 30,000 deaths per year1. More than 90% of patients with advanced disease have bone metastases with a median survival of one year2. Patients with metastatic bone disease suffer from bone pain, fractures, low blood counts, and ultimately death3. The goal of project was to investigate the feasibility of hyperpolarized 13C-pyruvate(HP-13C) MRI techniques to quantitatively monitor lactate dehydrogenase (LDH) catalyzed pyruvate-to-lactate metabolism in prostate cancer bone metastases. This metabolic imaging approach could enable rapid monitoring of treatment response and development of therapeutic resistance, as well assess on-target treatment effects for new targeted drug development, thus addressing current unmet clinical needs4. This research is important because current imaging modalities for bone metastases are inadequate in assessing response to therapeutic interventions.Methods
Sequences: The HP-13C images were acquired using a 2D dynamic MRSI sequence with a slice-selective spectral-spatial excitation, followed by phase-encode and echo-planar spectroscopic imaging readout5. Some sequence parameter are as follows, TR/TE = 130ms/3.5ms, 3s temporal resolution, constant flip angle Pyr 10°, Lac 20°. LAVA and SSFSE series were acquired as references.
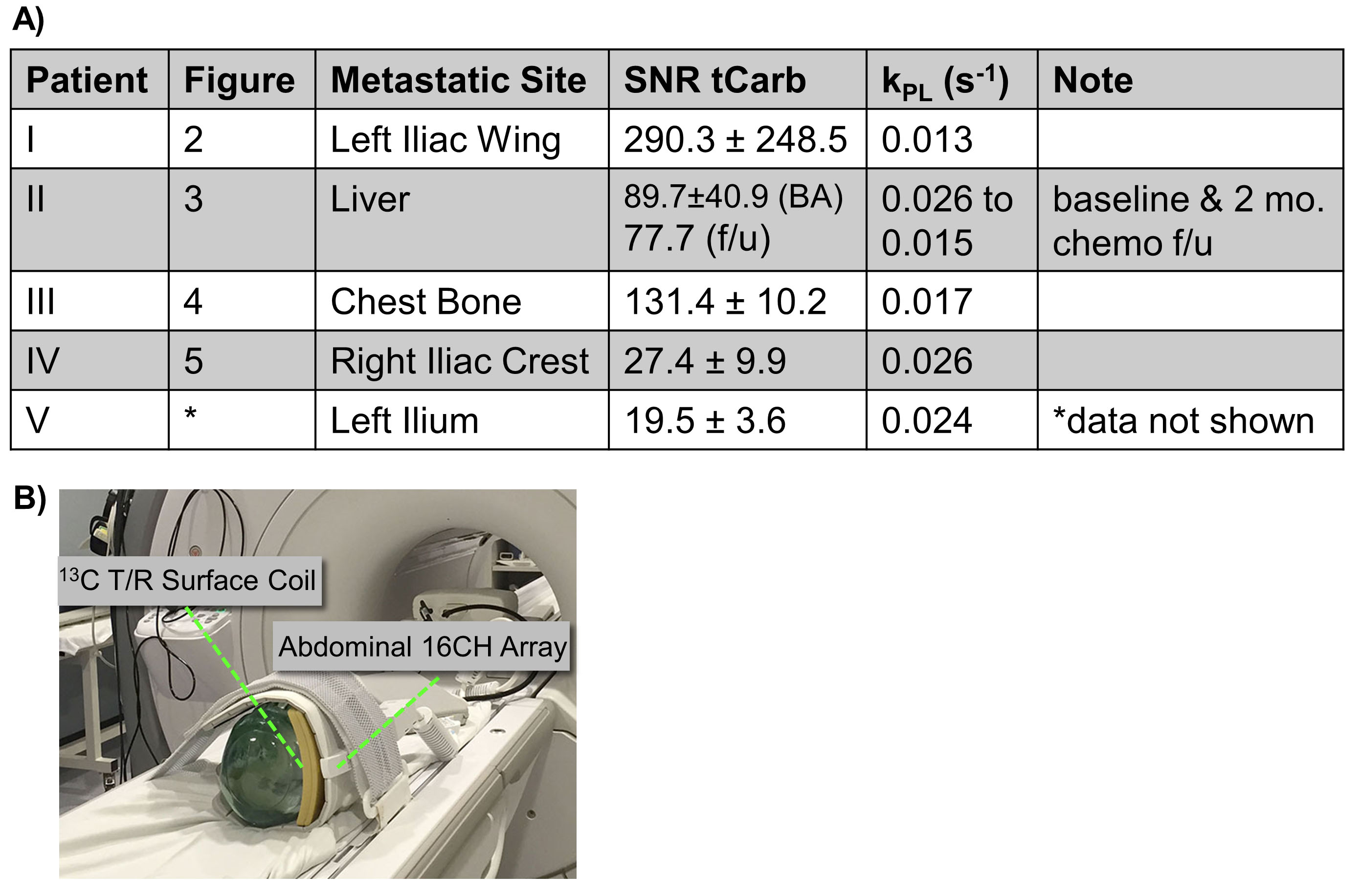
Patient Studies: A cohort of 5 patients with metastatic prostate cancer were examined in this study, targeting either pelvic or chest bone lesions on 4 of them. One patient with liver metastasis was scanned prior to and 2-month after initiation of chemotherapy. GMP [1-13C] pyruvic acid was polarized in a 5T SPINLab polarizer for 2-3 hours, and dissolutions yielded 235±10 mM sterile pyruvate with 37.4±3.5% polarization, 0.6±0.4μM radical and 30.9±0.5°C temperature. A 13C transmit-receive surface coil targets the bone and liver lesions, and proton imaging was conducted using a 16-channel receiver array (Fig.1B). All studies were approved by IRB at UCSF.
Data Processing: The 2D dynamic MRSI datasets were processed by applying even-odd lobe phasing, B0-shift correction, tensor-low-rank denoising6, baseline correction, followed by a phase-sensitive peak quantification. The pyruvate-to-lactate conversion kPL was evaluated using an inputless single-compartment two-site exchange model7.
Results and Discussions
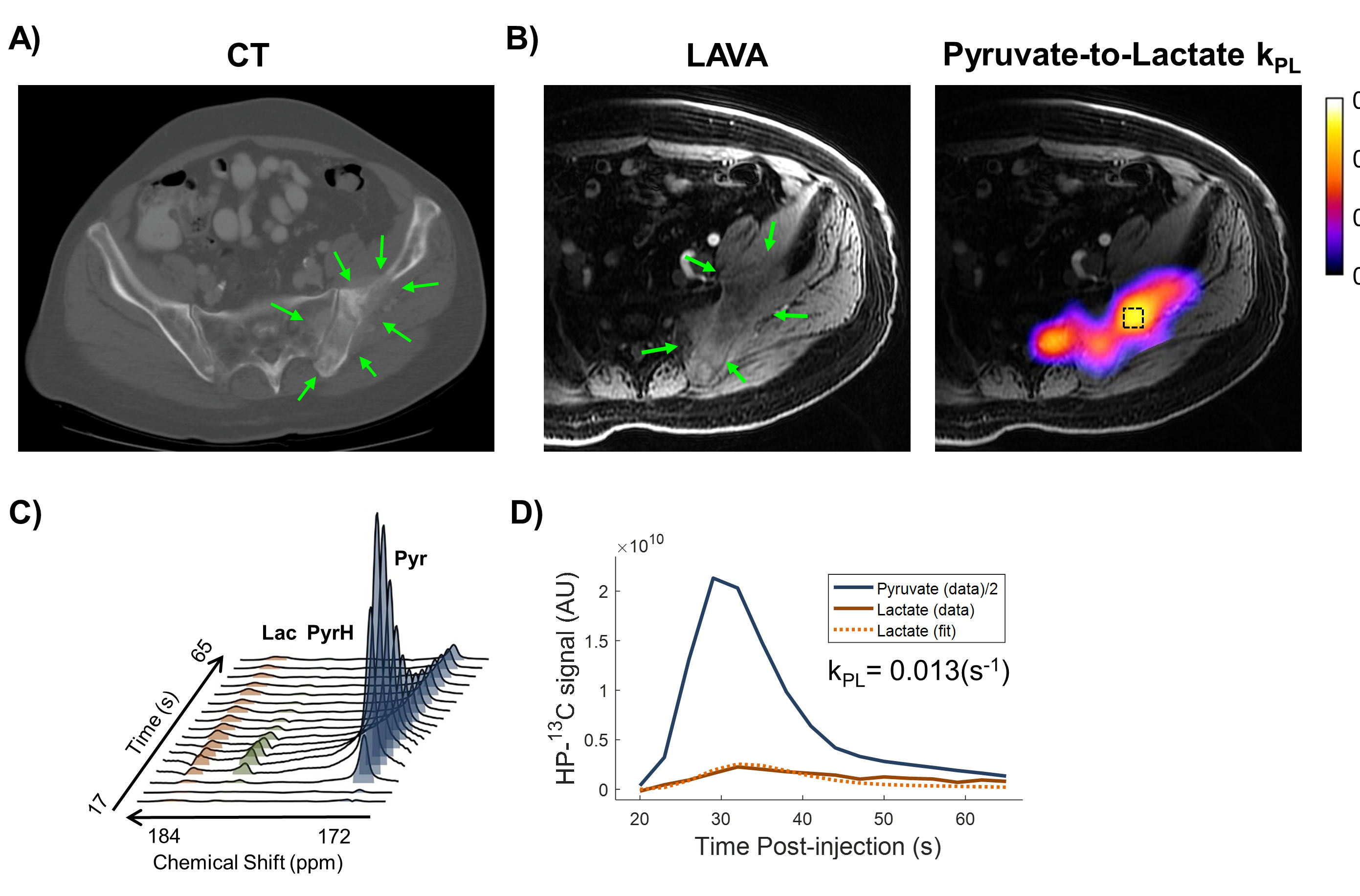
The patient cohort is summarized in the table in Figure.1A. Figure.2 showed a 75 y/o patient with mCRPC who had several large osteoblastic lesions throughout the left hemipelvis and involving left femur. CT identified a relatively osteolytic lesion in left ilium. Regions of high pyruvate-to-lactate conversion rate (kPL) correlated with the osseous lesion on both CT and MR (Fig.2A,B). kPL was calculated 0.013(s-1) at the targeted lesion, where Fig.2C,D showed the spectra over time and the inputless two-site kinetic fit, respectively.
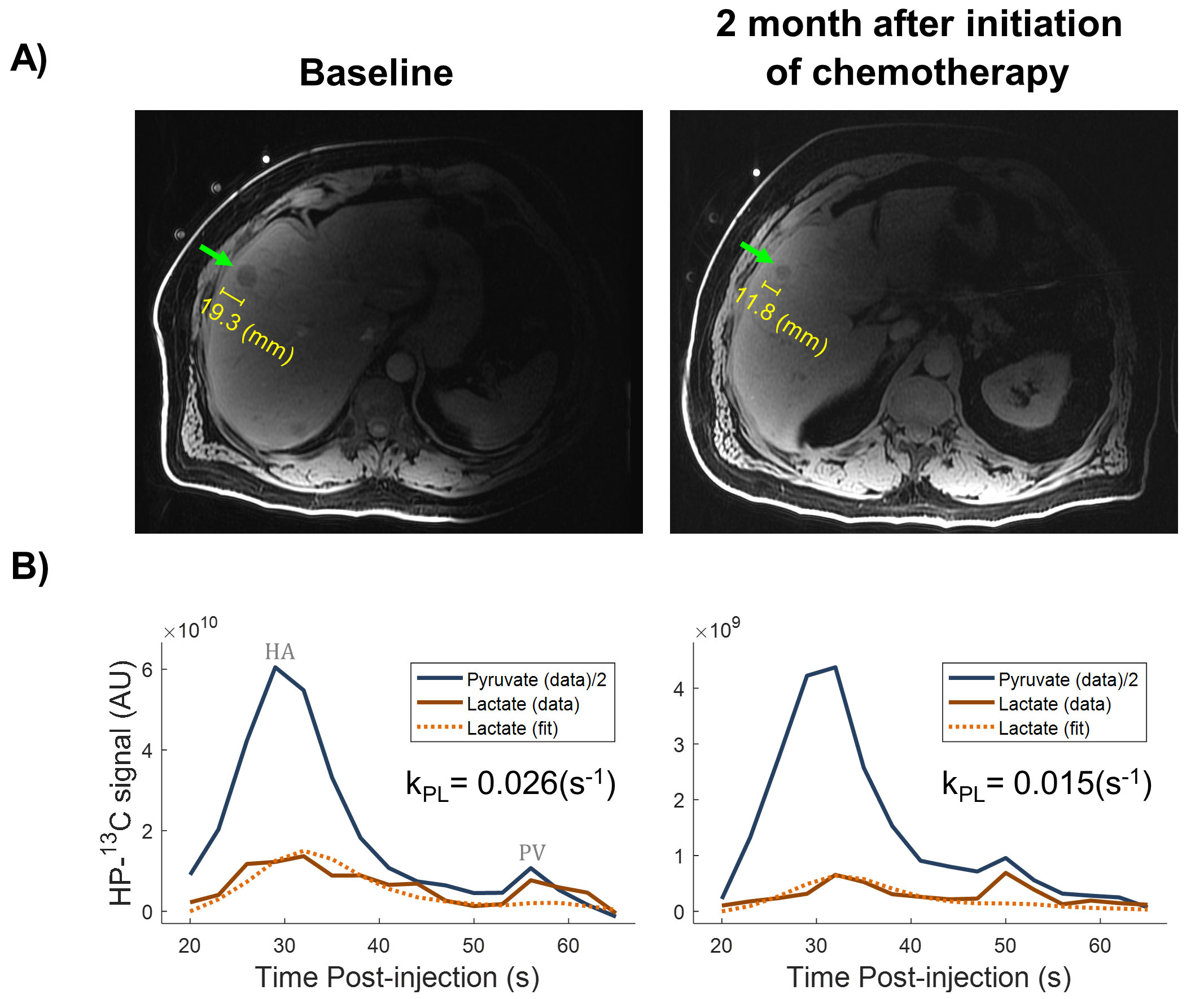
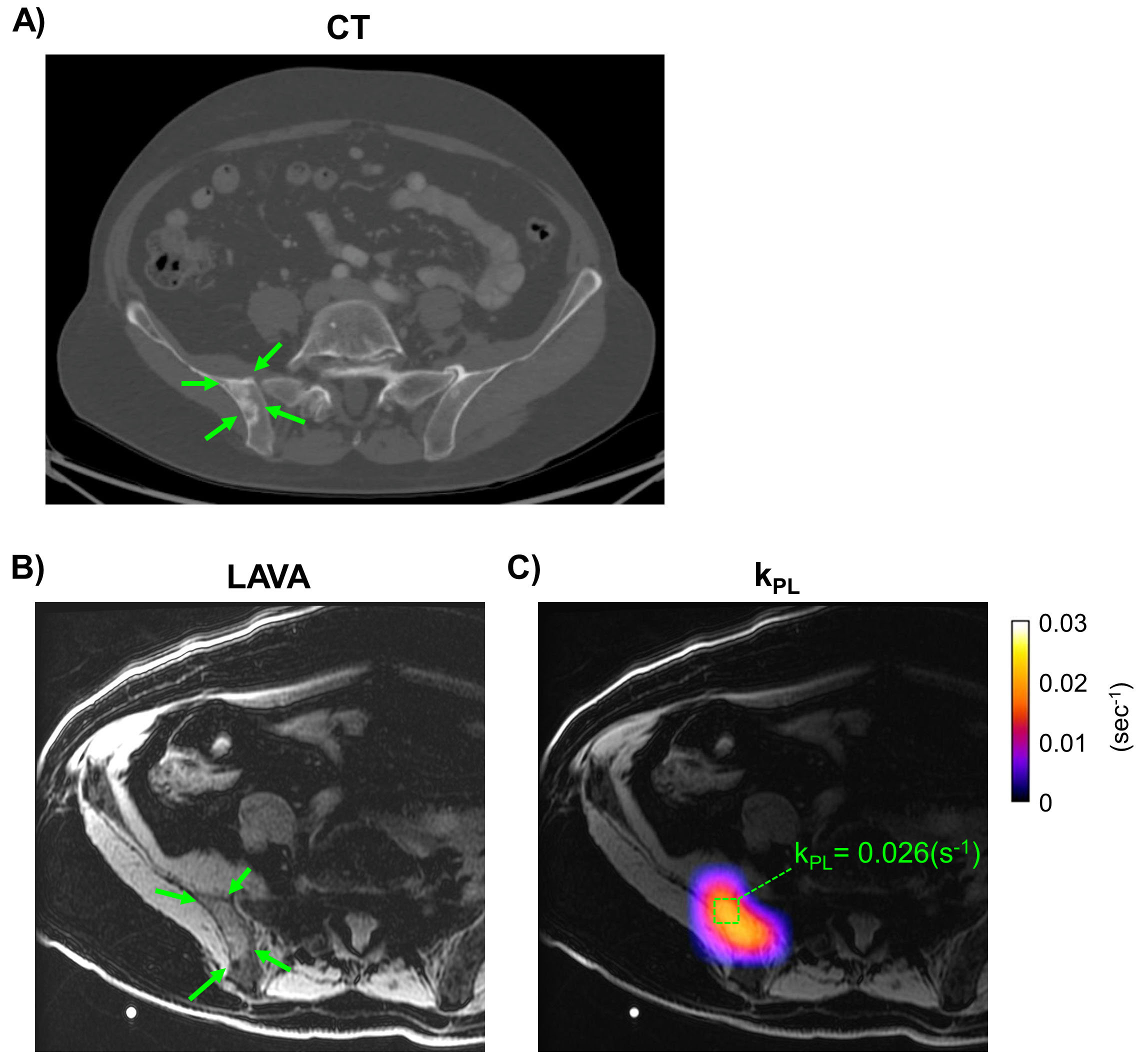
Figure.3 illustrated a 57 y/o individual with mCRPC to the liver. Chemotherapy of carboplatin+docetaxel started ~1 month post- baseline scan. Follow-up 2 months after initiation of therapy found interval decrease of lesion size (19.3mm to 11.8mm) that indicated response based on RECIST criteria (Fig.3A), accompanied by PSA decrease (25 to 13.4 ng/ml). Between the baseline and follow-up HP-13C exam, interval decrease of pyruvate-to-lactate conversion rate kPL was observed from 0.026(s-1) to 0.015(s-1) that correlated to response (Fig.3B). Partial volumes increase as tumor shrinks, meaning the actual kPL decrease could be more prominent than measured. Note the portal venous bolus around 50-60s post-injection. The lactate there could be largely vascular, coming from intestines.
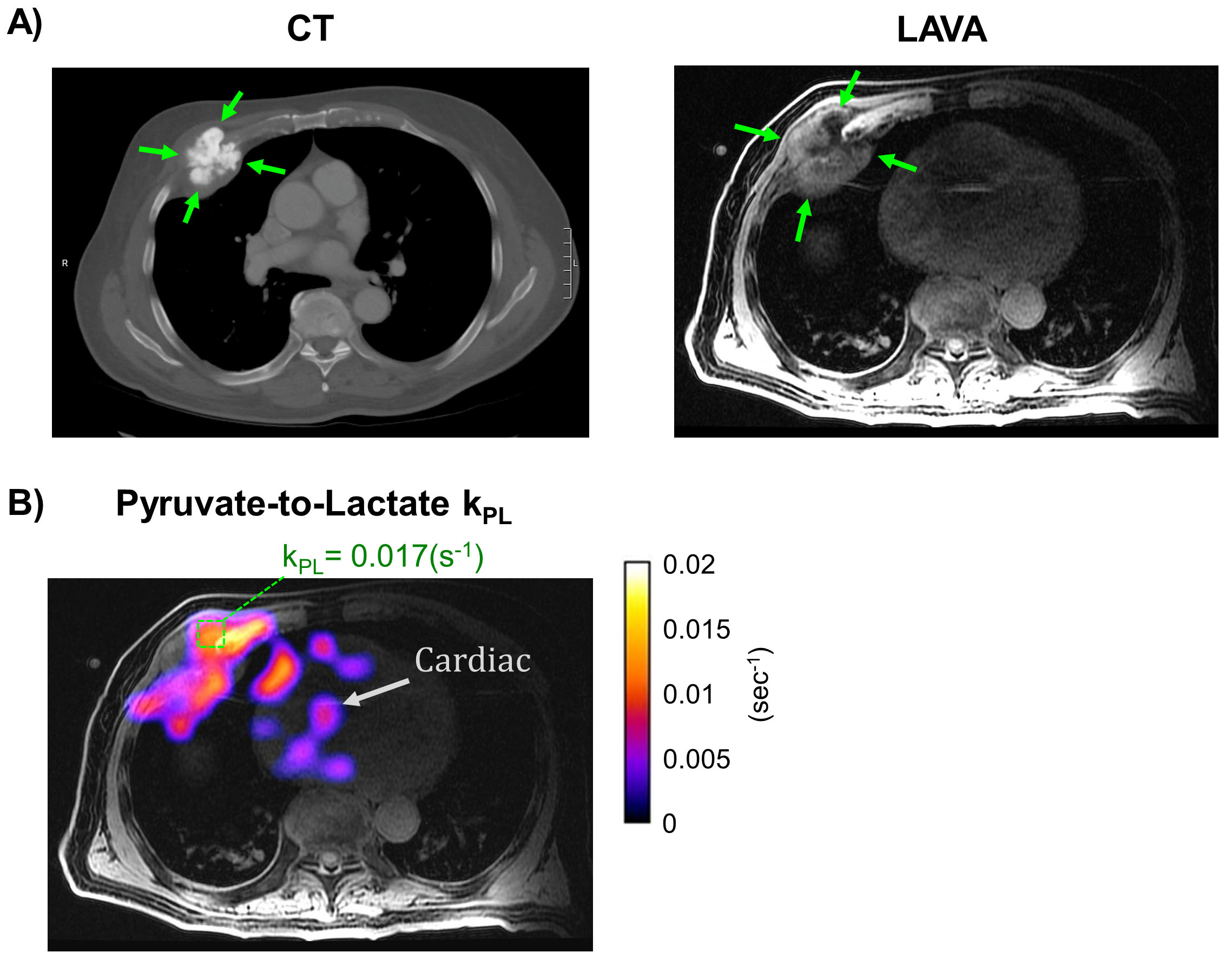
Figure.4 showed an 83 y/o patient with osteoblastic metastatic disease throughout rib cage, spine and pelvis. CT and LAVA images identified osseous lesions on right anterior 4 and 5th rib, measuring 5.1x4.0cm, with soft tissue components (Fig.4A). In vivo biodistribution of HP-13C biomarkers was illustrated by pyruvate and lactate signals maps summed over time (Fig.4B). kPL of 0.017(s-1) was found in the targeted lesion. Coincidentally, this kPL value was comparable to those observed in aggressive primary prostate adenocarcinoma of a patient cohort prior to radical prostatectomy8.
Figure.5 showed a 72 y/o man who had extensive disease in rib cage, spine and pelvis. CT identified an osteoblastic lesion at right iliac crest (Fig.5A) As illustrated in Fig.5C, kPL at the iliac crest lesion was calculated 0.026(s-1).
In summary, kPL decrease was found on one patient indicating response to chemotherapy, which agreed with PSA and RECIST criteria. On patients with bone metastases, high kPL values were observed comparable to aggressive primary prostate cancer.
Conclusions
This study investigated the feasibility of imaging metabolism and therapeutic responses using HP-13C MR in patients with metastatic prostate cancer. The findings suggest that these metastases are highly metabolically active, and demonstrated the potential of kPL as a quantitative in vivo marker to monitor systemic drug delivery and treatment of bone-tropic advanced prostate cancer.Acknowledgements
This work was supported by grants from the NIH (R01EB017449, R01CA166655, R01 CA215694, and P41EB013598).References
[1] American Cancer Society: Cancer Facts and Figures 2018; https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2018/cancer-facts-and-figures-2018.pdf
[2] Cheville, JC et al., Metastatic prostate carcinoma to bone: clinical and pathologic features associated with cancer-specific survival. Cancer 2001; 95(5), 1028-1036.
[3] Todenhöfer T et al., Targeting bone metabolism in patients with advanced prostate cancer: current options and controversies. Int J Endocrinol 2015;
[4] Fizazi K et al., Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study. Lancet 2011;
[5] Nelson SJ et al., Metabolic Imaging of Patients with Prostate Cancer Using Hyperpolarized [1-13C]Pyruvate. Sci Transl Med. 2013;5(198)
[6] Brender JR et al., PET by MRI: Glucose Imaging by 13C-MRS without Dynamic Nuclear Polarization by Noise Suppression through Tensor Decomposition Rank Reduction; bioRxiv. 2018;
[7] Larson PEZ et al., Investigation of Analysis Methods for Hyperpolarized 13C-pyruvate Metabolic MRI in Prostate Cancer Patients; NMR in Biomed. 2018; DOI:10.1002/nbm.3997
[8] Korn et al., The Rate of Hyperpolarized [1-13C] Pyruvate to [1-13C] Lactate Conversion Distinguishes High-Grade Prostate Cancer from Low-Grade Prostate Cancer and Normal Peripheral Zone Tissue in Patients, Proceedings of ISMRM. 2018;
Figures