0707
Imaging wound-healing related fibrosis using short inversion time ultra-short TE (STIR-UTE)1Medicine (Cardiology), The Johns Hopkins University, Baltimore, MD, United States, 2Radiology, Brigham and Womens Hospital, Boston, MA, United States, 3Application Development, Siemens Healthcare GmbH, Erlangen, Germany, 4MRI, Siemens Healthineers, Boston, MA, United States, 5Medicine (Cardiology), Johns Hopkins University, Baltimore, MD, United States, 6Radiation Oncology, Johns Hopkins University, Baltimore, MD, United States
Synopsis
Collagen deposition occurs during wound-healing processes in several diseases, and following therapy (acute myocardium infarction, radiation induced fibrosis). There is interest in intervening during wound-healing, since chronic scar leads to complications (ventricular tachycardia, gastrointestinal bleeding), with novel medications possibly reducing fibrosis. Intervention requires early detection of diffuse fibrosis (<50% content/voxel) during acute wound-healing. Fibrosis detection with gadolinium-perfusion (LGE, T1 mapping) is problematic during acute disease, due to irregular vascularity. Ultrashort-Time-to-Echo’s (UTE’s) collagen-sensitivity is reduced by fat’s masking signal. With STIR-UTE, we utilize collagen’s short TE and short T1 to suppress fat and map fibrosis in the pelvis, in normal and in post-infarction hearts.
Introduction
Collagen deposition, followed by scar formation, occurs during the process of wound healing1. It follows other acute processes, such as inflammation. Collagen deposition is clinically important due to the ensuing clinical complications. In the heart, ventricular tachycardia and persistent atrial fibrillation result from deposition of dense (scar) or diffuse fibrosis, disrupting currents in the heart, and leading to reduced cardiac function. Radiation therapy is followed by radiation induced fibrosis (RIF), which forms scar tissue that causes, in cervical cancer patients, gastrointestinal bleeding and vaginal stenosis. Due to these negative effects, there is growing interest in early detection of collagen deposition, when there is still an opportunity for intervention2. MRI methods to image diffuse or dense fibrosis are primarily T1 mapping3 and Late Gadolinium Enhancement4, which rely on changes in Gd-contrast-perfusion, which is complicated during acute disease, due to inflammatory-caused changes in perfusion. Specific MRI contrast agents for type-I collagen5 are no longer available. Ultrashort Time-to-Echo (UTE) imaging has been investigated for detecting diffuse fibrosis6-8. A recent study of 0-50% collagen-aqueous MnCl2 solutions, approximating muscle tissue8, used multiple-TE UTE to separate out the collagen fraction at 7T, finding a ~750µsec T2*, a -3.56ppm chemical shift, and a signal amplitude directly related to collagen concentration. Despite UTE’s promise of direct collagen detection, lipids present a problem9, since they frequently occur in adjacent regions, have short T2* components10, have similar chemical shifts, and therefore can mask diffuse collagen signals. A prototype stack-of-spirals UTE sequence11, equipped with an adiabiatic inversion-recovery pulse, allowed high-resolution imaging without the streaking artifacts previously encountered with UTE. We attempted to use a very short inversion time (TI~100ms)10,11 to attenuate the lipid signal (T1fat=250-370ms at 1.5T), and multiple TE acquisitions to map the fibrosis fraction.Methods
Methods: Collagen fraction imaging. Assume j (j=1..N) material components in each voxel, with amplitudes Aj, each with its T1j and T2J* relaxation times, and select j=1 to be collagen-bound-water. The Transverse Magnetization MTrans observed following an IR UTE acquisition will be, allowing for spin recovery time after data acquisition, and assuming a low flip angle readout, which does not perturb spin relaxation: $$M_{Trans}(TE_{i},TI,Trel)=\sum_j(1-2\times e^{-\frac{TI}{T1_{j}}})\times e^{-\frac{TE_{j}}{T2^{*}_{j}}} \times (1- e^{-(\frac{T_{rel}+T_{sample}}{T1_{j}})})$$
where TI, Tsample, Trel and TEi are the selected inversion time, the sampling (data collection) time, the allowed spin recovery time after data acquisition, and the echo-times (i=1,…N), respectively, and $$$\sum_A^j=A_{total}$$$, where $$$\frac{A_{1}}{A_{total}}=F_{fibrosis}$$$ is the fibrosis fraction in each voxel.
Choosing $$$(\frac{T_{rel}+T_{sample}}{T1_{j}})\ll1$$$ for j>1 (i.e. for all species, excluding collagen), will attenuate the longer T1 signal components, which are mainly composed of soft tissues (at 1.5T, muscle T1 is 870msec).
If we further select $$$(1-2 \times e^{-\frac{TI}{T1_{fat}}})\sim 0 $$$ ,fat is largely-suppressed, and we primarily sample the fibrosis fraction in each voxel. However, we still image other very short T1 and T2* species (para-magnetic stool) that are present, which must later be segmented out using information from additional MRI contrasts (T2-weighted imaging, diffusion weighted imaging).
MR Imaging. We imaged on a 1.5T Aera scanner (Siemens Healthcare, Erlangen, Germany). Multiple TE STIR-UTE parameters: TRel/Tsample/TI/flip-angle=400/560/100msec/100, TEj=50,100,300µsec (non-interleaved echoes), 80-88sl/vol, 50% slice-encode, 6/8 in-plane encode, resolution=1.3x1.3x1.6-2.0mm3,1 avg, SPIRIT13,14 reconstruction, 3:30min/echo. Conventional UTE (same parameters, no IR pulse, 2:30min/echo) was acquired for comparison and 2D FSE (TR/TE=3000/101ms, resolution=1.2x1.2x2.0mm3, 50sl/vol, 1:40min/vol) for anatomic correlation. Cardiac STIR-UTE imaging utilized prospective self-navigation (~100msec between spiral navigators), requiring 16:30-18:00min/echo).
Image processing. The multi-echo STIR-UTE images were processed using custom Matlab (Needham, MA) software. Before fitting using Matlab's NLINFIT, a 9x9 neighborhood Gaussian smoothing-filter, to improve the fit convergence, and a masking threshold-filter, to remove air pixels, were applied. Three-echo data were fit to a single exponential decay, providing A1, and T21*.
Subjects. (A) Ex-vivo infarcted swine heart in saline .(B) Healthy 30- and 65- yr old female volunteers.
Results
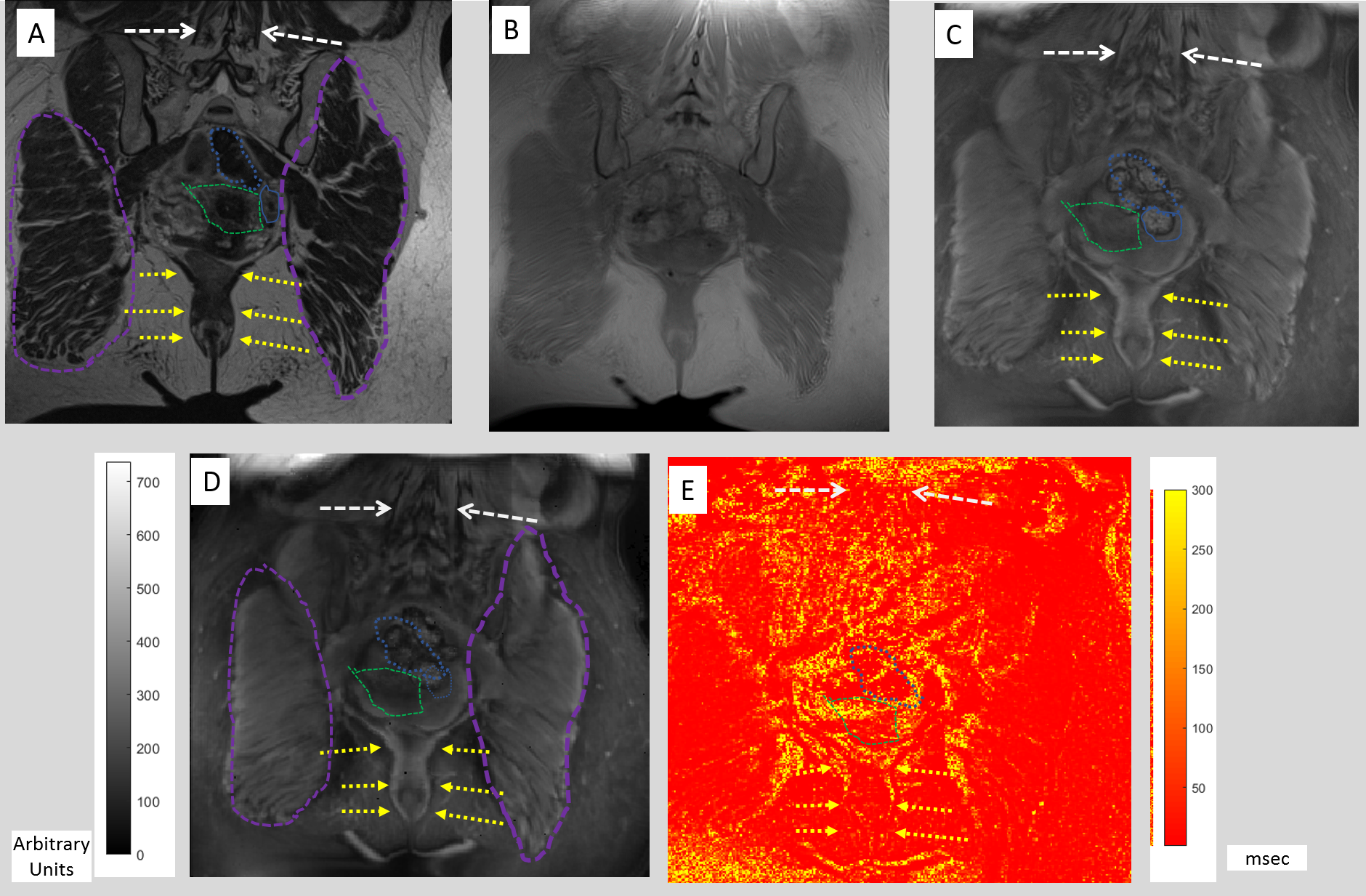
Pelvis of 65-yr old volunteer: Figure 1 compares T2, UTE, and STIR-UTE images in the pelvis, demonstrating improved visualization of short-TE components with STIR-UTE. The processed multiple-TE STIR-UTE images provide maps of short T2* components, which are primarily fibrotic tissues.
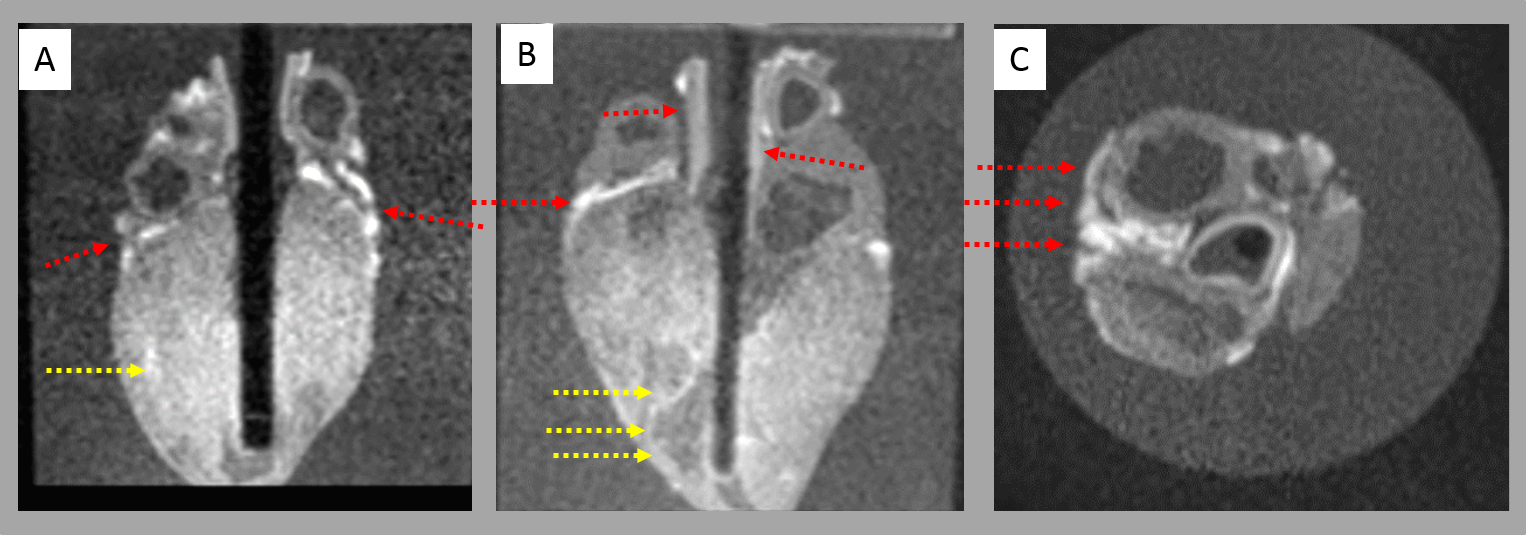
Ex-vivo infarcted heart: Figure 2 shows STIR-UTE images of a swine heart. The infarct borders, as well as fibrotic blood-vessel walls are visualized.
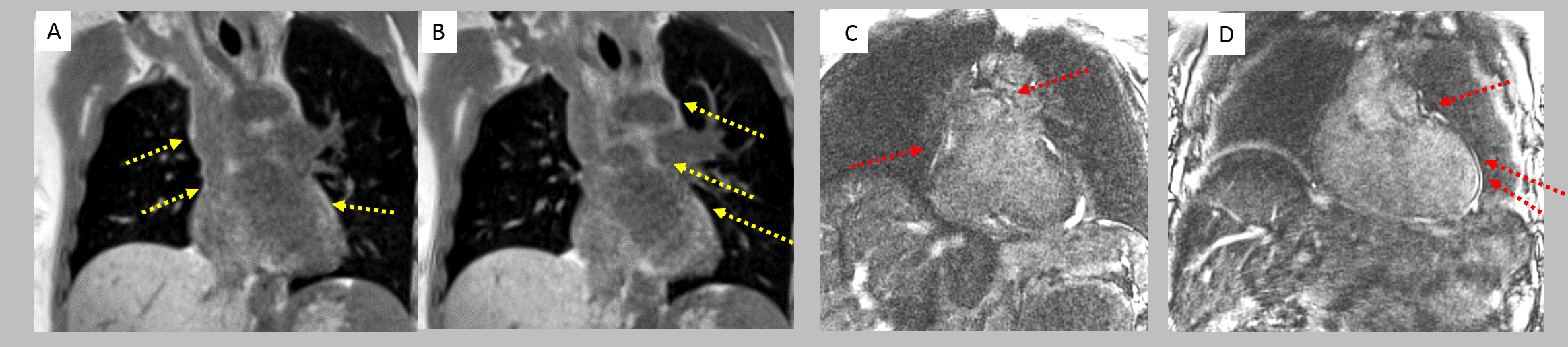
Self-Navigated volunteer hearts: Figure 3 compares UTE and STIR-UTE, demonstrating that STIR-UTE differentiates fibrosis from fat in blood-vessel walls.
Conclusions
STIR-UTE images provide collagen maps in several body regions, providing a means to monitor wound-healing.Acknowledgements
We acknowledge Josef Pfeuffer (Siemens Healthcare), John Mugler and Craig Meyer (University of Virginia) for their valuable contributions to the development of the UTE Spiral VIBE method and NIH R21CA167800, R01HL094610 fundingReferences
[1] Straub JM, New J, Hamilton CD, Lominska C, Shnayder Y, Thomas SM. Radiation-induced fibrosis: mechanisms and implications for therapy Cancer Res Clin Oncol. 2015; 141: 1985–1994.
[2] Pohlers D, Brenmoehl J, Löffler I, Müller CK, Leipner C, Schultze-Mosgau S, Stallmach A, Kinne RW, Gunter Wolf. TGF-β and fibrosis in different organs — molecular pathway imprints. Biochimica et Biophysica Acta 2009; 1792: 746–756
[3] Messroghli DR, Radjenovic A, Kozerke S, Higgins DM, Sivananthan MU Modified Look‐Locker inversion recovery (MOLLI) for high‐resolution T1 mapping of the heart. Magn Reson Med 2004; 52:141–146.
[4] Kim RJ, Fieno DS, Parrish TB, Harris K, Chen EL, Simonetti O, Bundy J, Finn JP, Klocke FJ, Judd RM. Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation 1999; 100: 1992–2002.
[5] Caravan P, Das B, Dumas S, Epstein FH, , Helm PA, Jacques V, Kolodziej A, Shen L, Sun W-C, Zhang Z. Collagen‐Targeted MRI Contrast Agent for Molecular Imaging of Fibrosis. Angewandte Chemie 2007;119, 8319-8321
[6] de Jong S, Zwanenburg JJ, Visser F, der Nagel RV, van Rijen HV, Vos MA, de Bakker JM, Luijten PR. Direct detection of myocardial fibrosis by MRI. J. Mol. Cell. Cardiol. 2011; 51: 974–979.
[7] Deligianni X, Kawel‐Boehm N, Dellas Buser T, Bremerich J, Bieri O, Santini F. In vivo detection of cardiac fibrotic tissue without contrast agent. Proceedings of the 21st Annual Meeting ISMRM, Salt Lake City: UT, USA; 2013; 4553
[8] Ramadeen A, Hu X, Morikawa L, Zhang L, Lau JYC, Liu G, Pop M, Connelly KA, Dorian P, Wright GA. Characterization of the ultrashort‐TE (UTE) MR collagen signal, NMR in Biomedicine 2015;28, 1236-1244
[9] Motaal AG, Noorman N, de Graaf WL, Hoerr V, Florack LMJ, Nicolay K, Strijkers GJ. Functional imaging of murine hearts using accelerated self‐gated UTE cine MRI. Int. J. Cardiovasc. Imaging, 2014; 31: 83–94
[10] Du J, Bydder M, Takahashi AM, Carl M, Chung CB, Bydder GM. Short T2 contrast with three-dimensional ultrashort echo time imaging, MRI 2011; 29:470-482
[11] Mugler JP III, Fielden SW, Meyer CH, Altes TA, Miller GW, Stemmer A, Kiefer B. Breath-hold UTE lung imaging using a stack-of-spirals acquisition. Proceedings of the 23rd Annual Meeting of ISMRM, Toronto, Canada 2015, p. 1476
[12] Rakow-Penner R, Daniel B, Yu H, Sawyer-Glover A, Glover GH. Relaxation Times of Breast Tissue at 1.5T and 3T Measured Using IDEAL. J. Magn Reson Imaging 2006; 23:87–91
[13] Lustig M, Pauly JM. SPIRIT: Iterative self‐consistent parallel imaging reconstruction from arbitrary k‐space Magn Reson Med 2010; 64:457-471
[14] SPIRIT-accelerated stack of spirals imaging: Mugler JP III, Meyer CH, Pfeuffer J, Stemmer A, Kiefer B, Accelerated Stack-of-Spirals Breath-hold UTE Lung Imaging Proceedings of the 25th Annual meeting of ISMRM, 2017, Abstract #4904
Figures