0706
Motion-robust pediatric abdominal angiography using dynamic 3D image self-navigator with 3D cones1Electrical Engineering, Stanford University, Stanford, CA, United States, 2Electrical Engineering and Computer Science, University of California, Berkeley, Berkeley, CA, United States, 3Radiology, Stanford University, Stanford, CA, United States
Synopsis
Respiratory motion detection using the k-space center (DC signal) can be problematic in pediatric subjects exhibiting highly irregular breathing patterns. To address this problem, we extract respiratory motion information from high frame rate (3.3 Hz), low-resolution (7.7 mm) 3D self-navigators derived from the imaging data (i.e., central portion of 3D cones k-space data) and reconstructed with a multi-scale low-rank framework. Localized motion estimates are obtained from the 3D self-navigators using optical flow registration. We demonstrate that region-specific motion information from 3D self-navigators better mitigates motion artifacts compared to the low-pass filtered DC signal in pediatric abdominal angiography exams.
Introduction
Respiratory motion is a major impediment to the acquisition of high quality abdominal images. For effective respiratory motion compensation, accurate motion estimates must first be obtained. Respiratory bellows and k-space center (DC) are common strategies to derive breathing patterns1,2,3. Recent studies, however, have shown superior image sharpness when leveraging localized motion information from image-based self-navigators4. The purpose of this work is two-fold: (1) demonstrate a new method to reconstruct low spatial resolution 3D self-navigators (3D SNs) with high temporal resolution from 3D cones central k-space data and (2) present a technique to track complex respiration patterns in pediatric abdominal scans using 3D SNs for improved motion-suppressed reconstructions.Methods
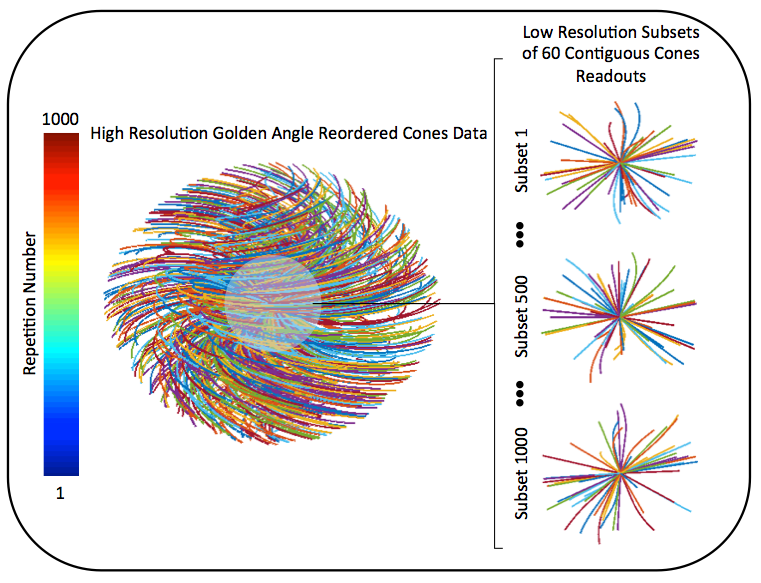
Acquisition and Reordering: Free-breathing pediatric abdominal examinations are performed with an RF-spoiled GRE sequence with a 3D cones k-space sampling trajectory5. To enable a sliding window reconstruction of 3D SNs, we utilize 2D golden angle acquisition ordering, which places each cone interleaf in a way that any subset of contiguously collected readouts provides distributed k-space coverage6 (Figure 1).
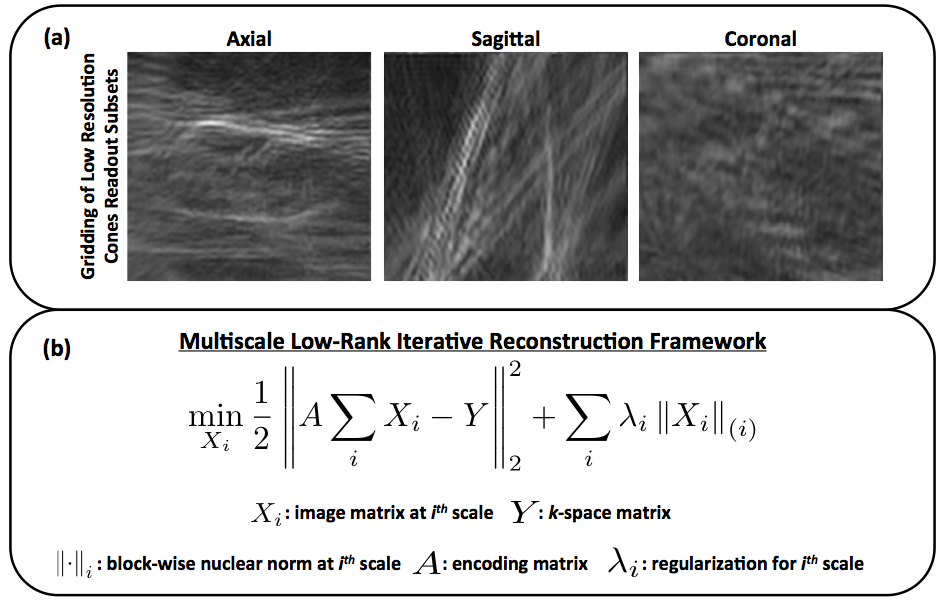
3D Self-Navigator (3D SN) Reconstruction: With a window width of 60 readouts, corresponding to a temporal resolution of approximately 300 ms (depends on TR), we reconstruct high frame rate 3D SNs at an isotropic spatial resolution of 7 mm. The acceleration factor corresponding to this temporal and spatial resolution yields significant aliasing artifacts with a gridding reconstruction alone (Figure 2(a)). Therefore, we propose to iteratively solve for the low resolution 3D SN images by exploiting parallel imaging and spatiotemporal correlations with multiscale low-rank constraints (Figure 2(b)).
Motion Extraction: To derive region-specific motion estimates from the 3D SNs, we follow a three-step methodology: (1) identification of an end-expiration reference frame, (2) prescription of a mask over the structure of interest (e.g., liver), and (3) optical flow registration of each 3D SN to the reference frame. The voxel-by-voxel nonrigid motion information is then spatially averaged to yield localized SI, AP, and RL displacements.
Image Reconstruction: The direction of largest displacement is used in l1-ESPIRiT (with spatial wavelet) to suppress respiratory motion artifacts by assigning lower weights to motion-corrupted readouts in the data consistency term (soft-gating)7,8. For comparison, we determine respiratory motion from the low pass filtered (cutoff at 0.67 Hz) DC signal, and reconstruct the imaging data with l1-ESPIRiT using this information as well.
Experiments: With informed consent and IRB approval, free-breathing pediatric subjects were scanned after administration of contrast on a 3T scanner (GE MR750, Waukesha, WI) with a 32-channel cardiac coil. Scan parameters included a flip angle of 15 degrees, bandwidth of ±125 kHz, echo time of 32 us, TR ranging between 4.7–9.8 ms, and scan durations of 2.5–5.2 min. For each subject, reconstruction with respiratory waveforms determined using 3D SNs was compared with the corresponding reconstruction based on the DC signal.
Results and Discussion
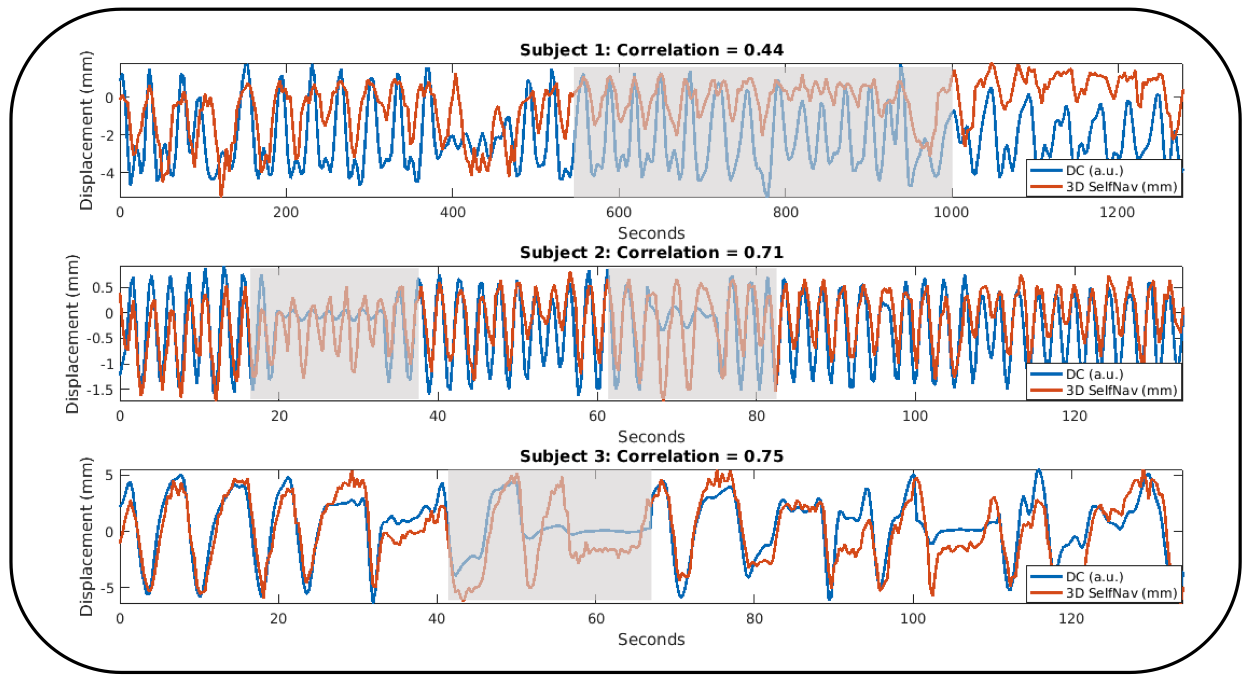
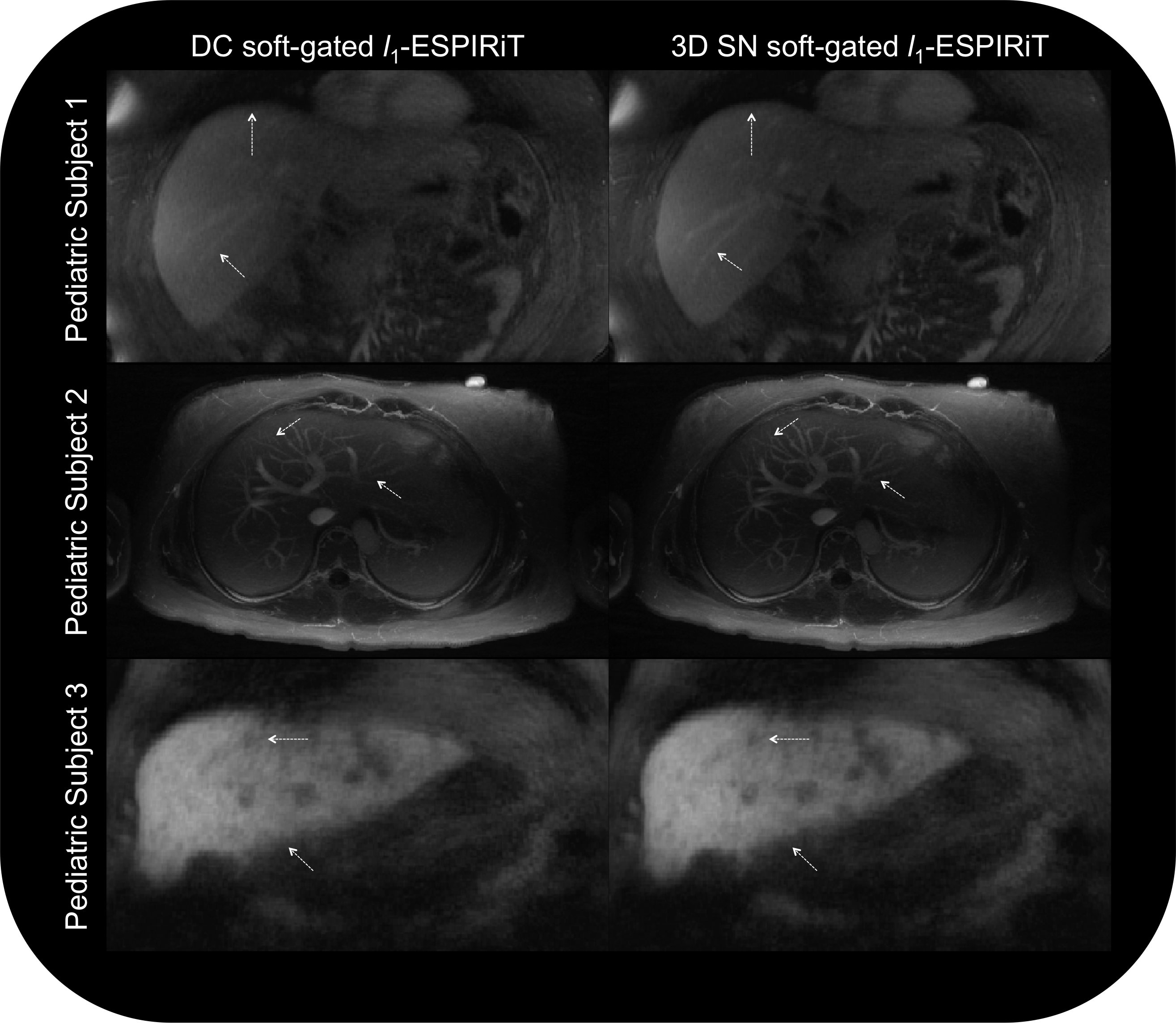
Videos of example 3D SNs for three different pediatric studies present a mixture of deep and shallow breathing patterns at varying rates (Figure 3). Corresponding respiratory motion estimates, as well as the low pass filtered DC signal, are presented in Figure 4. The DC signal does not effectively capture irregular trends, resulting in poor Pearson correlation coefficients with the 3D SN respiratory motion information. Improved depiction of vessels is seen in soft-gated l1-ESPIRiT reconstructions when utilizing 3D SN motion estimates instead of the DC signal (Figure 5).
While 3D SNs yield better image quality, they are more computationally expensive to reconstruct and process than simply filtering the DC signal. With parallel processing on two GPUs (NVIDIA Titan Xp), we can reconstruct 1000 3D SN frames in approximately 7 minutes. The extraction of motion information requires an additional minute. The overall computing time can be significantly reduced with a greater number of GPUs, and optimization of the temporal and spatial resolutions of 3D SNs.
Conclusion
Here, we presented a technique to extract high frame rate, low spatial resolution 3D abdominal self-navigators in a free-breathing, ungated cones acquisition scheme for pediatric imaging. Furthermore, we highlighted a strategy to compute localized motion estimates from the 3D self-navigators. Through several pediatric subject studies, we demonstrated that integration of this motion information into soft-gated l1-ESPIRiT reconstructions yields improved image quality compared to using the DC signal alone. While we have primarily focused on monitoring the movement of the liver using 3D SNs, the proposed motion tracking methodology can be applied in other parts of the body, including, for example, the kidneys.Acknowledgements
We gratefully acknowledge the support of NIH grants R01HL127039, R01EB009690, R01EB026136, R01HL136965, T32HL007846, and T32EB009653. This work was also supported by the Hsi-Fong Ho Stanford Graduate Fellowship, the Ruth L. Kirschstein National Research Award, and the National Science Foundation Graduate Research Fellowship under grant DGE-114747.References
[1] Brau et al. MRM 55.2 (2006): 263-270.
[2] Larson et al. MRM 51.1 (2004): 93-102.
[3] Crowe et al. MRM 52.4 (2004): 782-788.
[4] Jiang et al. MRM 79.6 (2018): 2954-2967.
[5] Gurney et al. MRM 55.3 (2006): 575-582.
[6] Malavé et al. MRM 00.0 (2018): 1-12.
[7] Uecker et al. MRM 71.3 (2014): 990-1001
[8] Cheng et al. JMRM 43.6 (2016): 1355-68.
Figures