0705
Time-efficient fully 3D non-Cartesian dynamic contrast-enhanced free-breathing MRI of the pelvis with an ultrashort TE cones trajectory1Radiology, Stanford University, Stanford, CA, United States, 2Electrical Engineering and Computer Sciences, University of California, Berkeley, Berkeley, CA, United States, 3Applied Science Laboratory, GE Healthcare, San Diego, CA, United States, 4Electrical Engineering, Stanford University, Stanford, CA, United States
Synopsis
A 3D cones k-space trajectory with golden angle ordering was developed along with a multiscale low rank reconstruction for dynamic contrast enhancement with ultrashort echo time (DCE-UTE) and with fast image reconstruction time. With IRB approval and informed consent the sequence was tested in 21 consecutive subjects referred for 3T contrast-enhanced pelvic MRI. For comparison, a Cartesian DCE SPGR sequence with golden angle radial k-space ordering, soft-gated self navigation, and low rank reconstruction (DCE-SPGR) served as case controls. DCE-UTE performed significantly better than DCE-SPGR in delineation of anatomic structures (p=0.004) and overall perceived image quality (p=0.003). These results indicate a 3D fully noncartesian DCE-UTE sequence and reconstruction improves image quality in pelvic DCE.
Introduction
Dynamic contrast enhanced (DCE) imaging plays a key role in the diagnosis and delineation of multiple pelvic pathologies including prostate cancer, rectal cancer and fibroid vascular supply1-3. Challenges in pelvic DCE include low spatiotemporal resolution, motion artifacts, and susceptibility from bowel gas. Standard approaches include use of parallel imaging, compressed sensing, and other forms of undersampling. These approaches have been extended to semi-non-Cartesian methods, such a stack of stars4. For even further motion robustness and reduced susceptibility artifact, fully non-Cartesian approaches which utilize a fully 3D radial trajectory have been deployed5. However, these methods have relatively low data sampling efficiency. Thus, we develop a 3D cones trajectory with golden-angle ordering for higher sampling efficiency6-8 and couple it to a multiscale low rank reconstruction.
Our goal is to demonstrate feasibility of conical DCE-UTE imaging in the pelvis and compare the resulting image quality with optimized Cartesian DCE imaging.
Methods
This was a prospective study with IRB approval with informed consent. Inclusion criteria were adult age and referral for 3T contrast-enhanced pelvic imaging. Exclusion criteria were musculoskeletal and prostatic indications. 21 sequential patients were included.
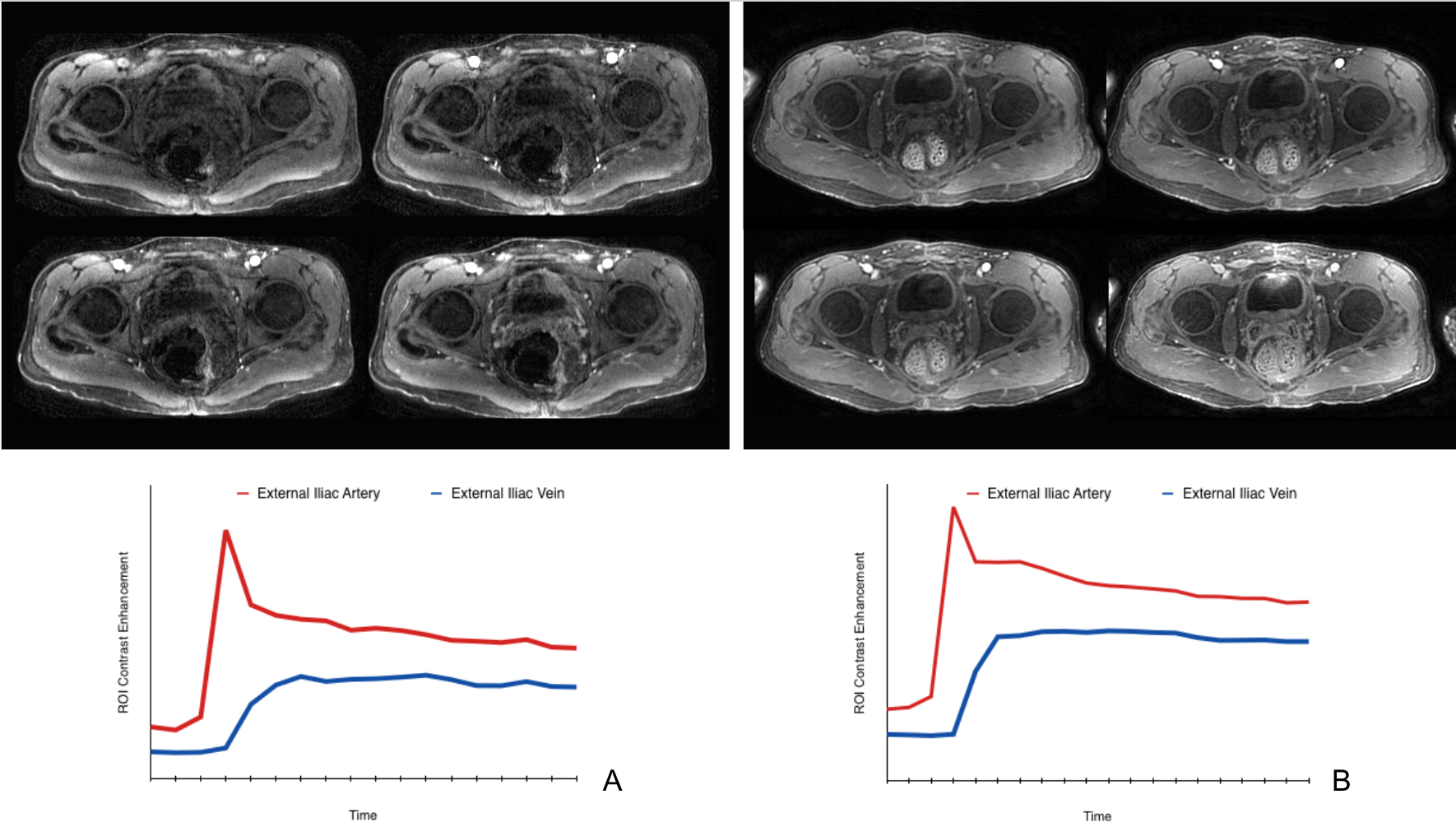
We compared a Cartesian DCE free breathing spoiled gradient echo sequence (SPGR) that was optimized for spatiotemporal resolution and motion robustness9 to 3D cones DCE-UTE trajectory (Figure 1). Series parameters are presented in Figure 2. Case controls were retrospectively identified in a stepwise process: (1) if available, the most recent prior local pelvic MRI including DCE-SPGR imaging within the past 3 years (n=7); (2) if no recent local examinations, the most recent qualifying study performed for a patient of the same sex, +/- 2 years age-matched, for the same general indication (n=14).
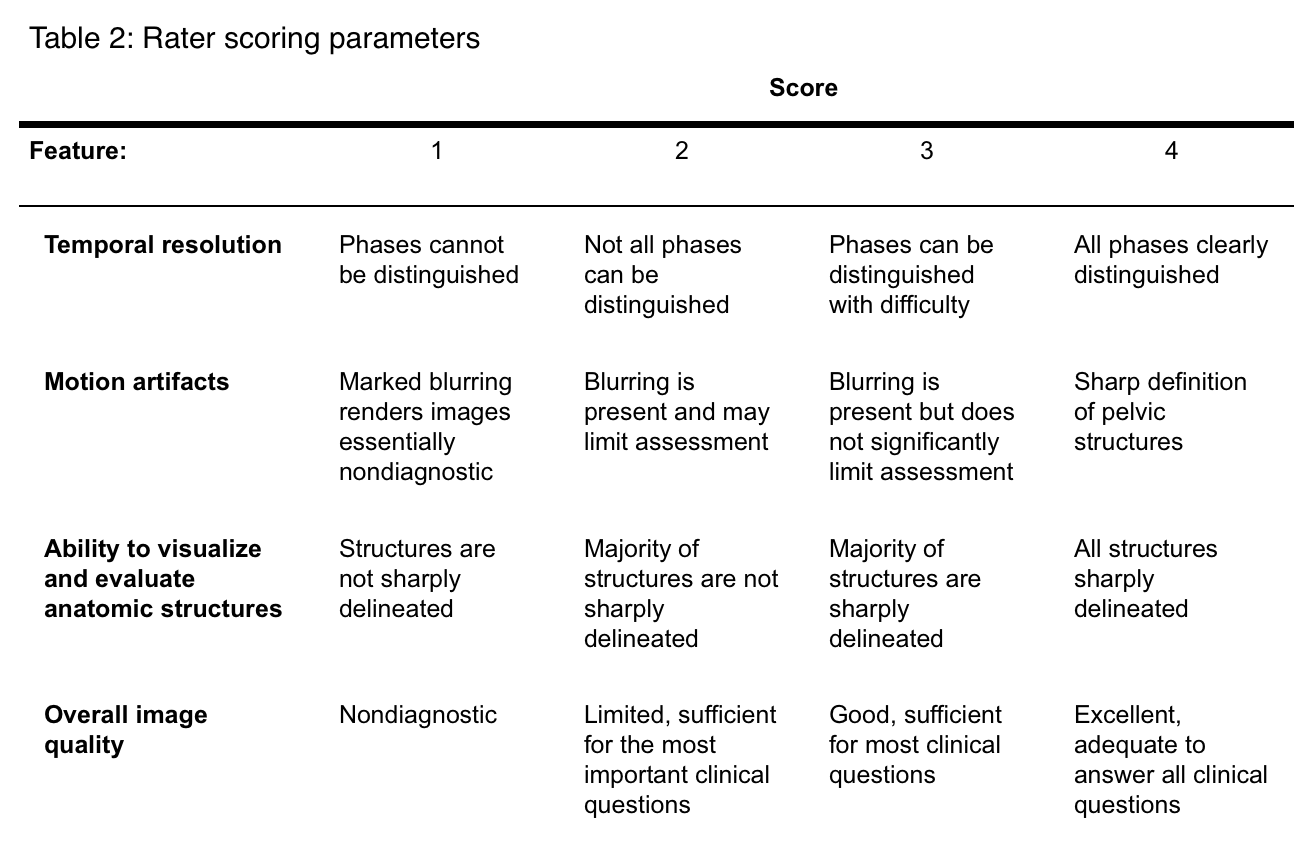
A multiscale low rank matrix decomposition was used for DCE-UTE image reconstruction (Figure 1b)10. The reconstruction was implemented in Python and CUDA, and run on workstations with an NVIDIA Titan Xp GPU. Multiphase images from equivalent anatomic levels were selected as shown in Figure 2. Images were graded according to predetermined criteria (Table 2). Two readers (RB and VS, both with five years experience interpreting body MRI) independently scored the 42 sets of images in a blinded, randomized fashion. Inter-reader agreement was assessed using the linear weighted Cohen’s kappa statistic. Image quality scores between pulse sequences were assessed using the two-tailed Wilcoxon signed rank test. P value less than .05 following Holm-Bonferroni correction for multiple comparisons was considered significant11.
Results
Image construction was successfully completed on all cases (reconstruction time 42-100 minutes). The 42 MRIs included 21 DCE-UTE (11 female, 10 male; mean age 54, 33-81 years) and 21 DCE-SPGRg case controls (11 female, 10 male; mean age 54, 32-81 years). Clinical indications included perianal fistula (n=5), anorectal malignancy (n=5), urinary tract malignancy (n=1), cervical/endometrial malignancy (n=5), benign uterine pathology (n=2) and scrotal pathology (n=2). The weighted Cohen’s kappa statistic for all observations was 0.51 (95%CI 0.40-0.61), indicating fair agreement between the two readers10. DCE-UTE performed significantly better than DCE-SPGR in delineation of anatomic structures (mean difference 0.67, p=0.004).and overall perceived image quality (mean difference 0.62, p=0.003). There was no significant difference in composite scores for phase resolution (mean difference -0.36, p=0.165) or presence of imaging artifacts (mean difference 0.21, p=0.208).
Discussion
This work addresses the combined challenges of spatiotemporal resolution, motion artifacts, and susceptibility in pelvic DCE. We extend prior work in fully 3D radial MRI by seeking greater sampling efficiency with a cones trajectory and developing computational methods to reconstruct images despite the greater sampling and reconstruction complexity. Conical DCE-UTE not only demonstrated noninferiority to existing Cartesian DCE-SPGR, but was superior in delineation of anatomic structures and overall perceived image quality, which are critical for assessment of complex pelvic pathologies.
This study did not account for the additional advantages of 3D conical UTE imaging over traditional Cartesian methods, including the ability to retrospectively reconstruct over an arbitrary time window or reduced through-plane motion artifacts on multiplanar reformations. We were limited by a small sample size and did not assess all possible parameters of image quality. This study was also limited by lack of quantitative quality metrics, and future assessment of lesion detection and characterization would provide further insight.
Conclusion
Conical DCE-UTE imaging has multiple advantages over Cartesian imaging, including improved image quality and higher sampling efficiency. In pelvic imaging, DCE-UTE is not only noninferior to optimized DCE-SPGR, but superior in delineation of anatomic structures and overall perceived image quality. These results show that conical DCE-UTE can be used effectively in the pelvis and merits further development.Acknowledgements
Grant support of NIH R01EB009690, R01 EB026136, R01HL136965, and GE Healthcare.References
1. Maciel C, Tang YZ, Sahdev A, Madureira AM, Vilares Morgado P. Preprocedural MRI and MRA in planning fibroid embolization. Diagn Interv Radiol. 2017 Mar-Apr;23(2):163-171.
2. Corines MJ, Nougaret S, Weiser MR, Khan M, Gollub MJ. Gadolinium-Based Contrast Agent During Pelvic MRI: Contribution to Patient Management in Rectal Cancer. Dis Colon Rectum. 2018 Feb;61(2):193-201.
3. Yeo DM, Oh SN, Jung CK, Lee MA, Oh ST, Rha SE, Jung SE, Byun JY, Gall P, Son Y. Correlation of dynamic contrast-enhanced MRI perfusion parameters with angiogenesis and biologic aggressiveness of rectal cancer: Preliminary results. J Magn Reson Imaging. 2015 Feb;41(2):474-80.
4. Wu Y, Korosec FR, Mistretta CA, Wieben O. CE-MRA of the Lower Extremities using HYPR Stack-of-Stars. J Magn Reson Imaging. 2009 Apr; 29(4): 917–923.
5. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD-GRASP: Golden-Angle Radial MRI with Reconstruction of Extra Motion-State Dimensions Using Compressed Sensing. Magn Reson Med. 2016 Feb; 75(2): 775–788.
6. Gurney PT, Hargreaves BA, Nishimura DG. Design and analysis of a practical 3D cones trajectory. Magn Reson Med. 2006 Mar;55(3):575-82.
7. Roh AT, Xiao Z, Cheng JY, Vasanawala SS, Loening AM. Conical ultrashort echo time (UTE) MRI in the evaluation of pediatric acute appendicitis. Abdom Radiol (NY). 2018 Jul 31 [epub ahead of print].
8. Zucker EJ, Cheng JY, Haldipur A, Carl M, Vasanawala SS. Free-breathing pediatric chest MRI: Performance of self-navigated golden-angle ordered conical ultrashort echo time acquisition. J Magn Reson Imaging. 2018 Jan;47(1):200-209.
9. Zhang T, Cheng JY, Potnick AG, Barth RA, Alley MT, Uecker M, Lustig M, Pauly JM, Vasanawala SS. Fast pediatric 3D free-breathing abdominal dynamic contrast enhanced MRI with high spatiotemporal resolution. J Magn Reson Imaging. 2015 Feb;41(2):460-73.
10. Ong F, Lustig M. IEEE J Sel Top Signal Process. 2016 Jun;10(4):672-687. Beyond Low Rank + Sparse: Multi-scale Low Rank Matrix Decomposition.
10. Holm S. A simple sequentially rejective multiple test procedure. Scand J Stat 1979;6(2):65–70.
11. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–174.
Figures
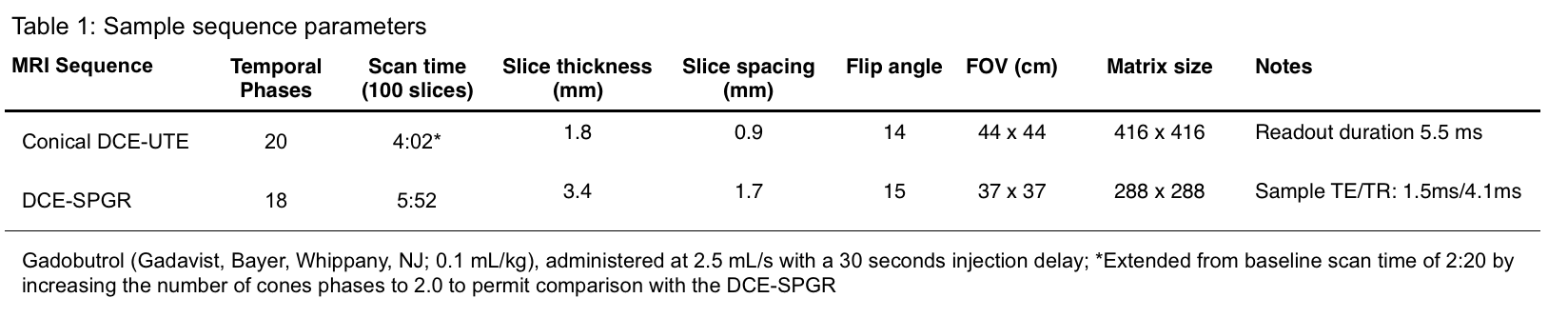
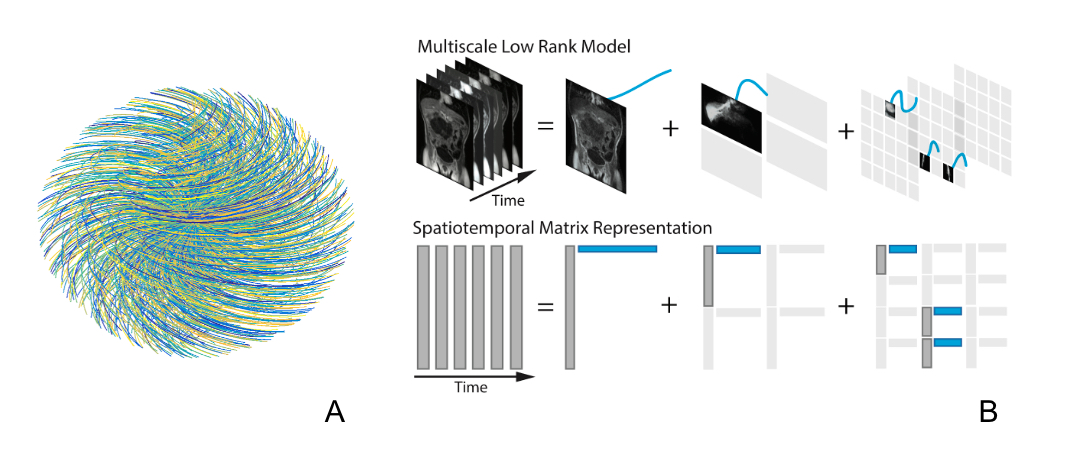
Figure 1. (A) An RF-spoiled GRE sequence with UTE is designed with a 3D cones k-space sampling trajectory. The data collection of each cone interleaf is ordered using the golden-ratio increment. (B) The spatiotemporal matrix is represented. We model our spatiotemporal matrix as a sum of block-wise low rank matrices with increasing scales of block sizes. The additional multi-scale structure permits a more accurate and compact signal representation than conventional low rank methods.