0702
Free-breathing renal perfusion measurement with volumetric ASL using variable-density FSE and 4D Compressed-Sensing1Division of MRI research, Radiology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boson, MA, United States, 2Global MR Applications and Workflow, GE Healthcare, Boston, MA, United States, 3Global MR Applications and Workflow, GE Healthcare, New York, NY, United States
Synopsis
While single or 2D multi-slice body ASL implementations have been shown to be compatible with free-breathing for abdominal perfusion measurement even in uncooperative clinical populations, free-breathing volumetric encoding has not been reported yet. We propose a free-breathing volumetric ASL acquisition relying on a motion-robust variable-density 3D-FSE sequence with redundant k-space center and pseudo-random variable outer k-space sampling and 4D-Parallel-Imaging-Compressed-Sensing reconstruction. High-quality whole kidneys perfusion images were obtained in less than 5 minutes in free-breathing, potentially extending the clinical applications of non-contrast ASL perfusion in the abdomen.
Introduction
Renal ASL with single-slice free-breathing1,2 and volumetric controlled-breathing acquisitions3 has been shown feasible and they both can yield high-quality perfusion images and derived blood-flow. However, free-breathing volumetric acquisitions are still challenging and haven't yet been reported. Such capability would nonetheless be highly desirable for translation into clinical practice, helping non-invasive perfusion measurement in uncooperative and/or patients with spatially spread disease (e.g. metastatic cancer). We propose a free-breathing volumetric ASL acquisition relying on a motion-robust variable-density 3D-FSE sequence with redundant-center and pseudo-random variable outer k-space sampling and 4D-Parallel-Imaging-Compressed-Sensing reconstruction.Material and Methods
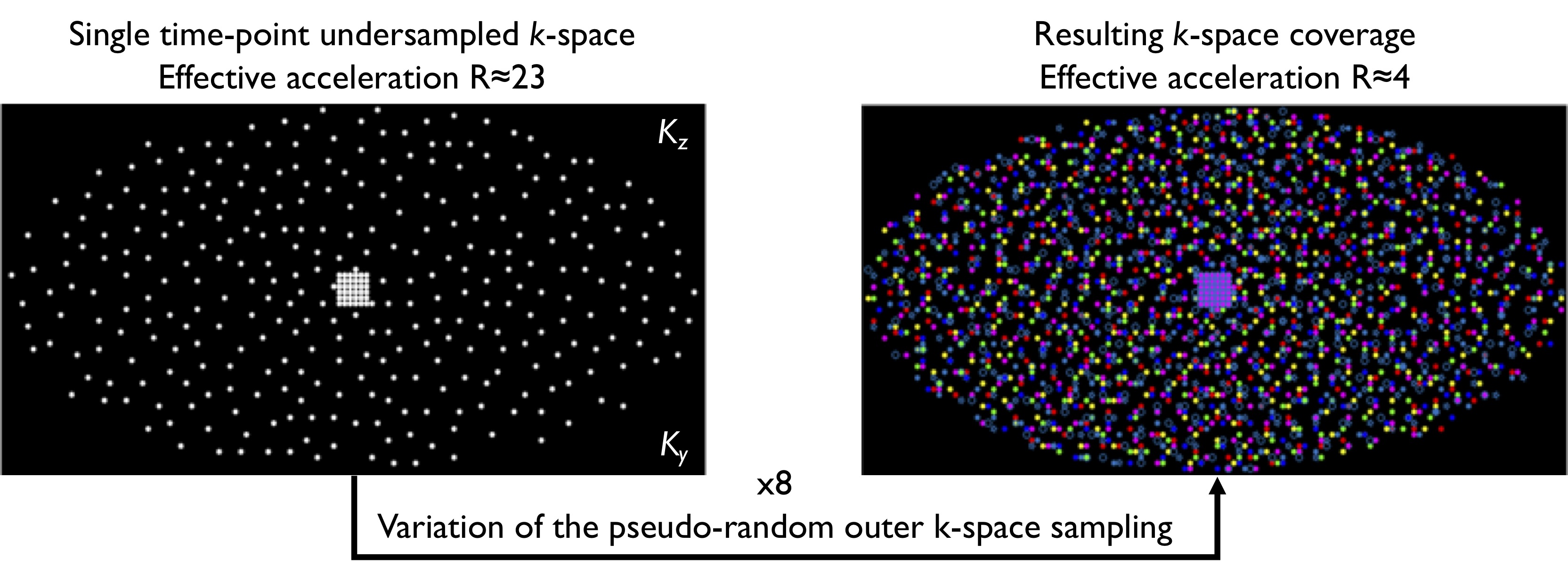
A pseudo-continuous ASL preparation was combined with a variable-density (VD) elliptic Poisson-disk segmented Cartesian FSE readout including a fully-sampled 6x6 k-space center region. To provide motion robustness, the outer k-space was pseudo-randomly undersampled to increase the temporal resolution. The undersampling was changed from repetition to repetition to increase overall k-space sampling. Because of resolution, slices and echo-train-length constraints, we designed a sampling enabling a minimum of 3-shots for each individual volumetric repetition. This acquisition was then repeated multiple times with variable outer k-space sampling (Fig.1). While each repetition was accelerated up to R≈23, the overall k-space coverage led to an effective acceleration of R=3.8.
N=3 volunteers were scanned at 3T (Discovery MR750, GE Healthcare) with a 32-ch body coil. We acquired free-breathing single-slice ASL with an single-shot-FSE (SSFSE) readout (TR/TE=6000/40ms, 128x128 matrix, 34-cm FOV, 10-mm slice thickness, bandwidth=20.83kHz, 6 label/control pairs, 1min30) as our gold standard.
Volumetric ASL scans were acquired with our VD-3D-FSE readout, with the following common parameters: TR/TE=6200/11ms, rBW=62.5kHz, ETL=120, FOV=32-34cm, 128x128x64 matrix, 64 3-3.4mm coronal slices, interleaved label/control acquisition as well as separate acquisition of a pre-saturated reference scan for coil-sensitivity estimation and blood-flow quantification using regular parallel-imaging undersampling for self-calibrated reconstruction. Two volumes were acquired, one with 4 repetitions of a 5-shot FSE (Tacq≈4min) under synchronized-breathing and another one with 8 repetitions of a 3-shot readout under free-breathing for Tacq=4min48s. All acquisitions used a pseudo-continuous labeling (500$$$\mu$$$s Hann-shaped pulses played for 1.5s followed by 1.5s PLD, average B1=1.4$$$\mu$$$T, Gmax/Gav=3.5/0.5mT/m), background suppression and in-flow saturation.
Raw k-space data were saved for offline reconstruction using MATLAB and the BART toolbox4. The high SNR reference volume was used for coil sensitivity estimation using ESPIRiT5 (calibration region 243,cluster size k=63,$$$\sigma$$$=0.01,threshold=0.8), followed by a 4D k-t-CS ESPIRiT reconstruction6,7 of the 4D-image m from the acquired data y with L1-norm minimization and spatial wavelets ($$$\psi$$$) and temporal total-variation (TV) sparsity operators:
$$$m(x,y,z,t)=argmin\parallel DFSm(x,y,z,t)-y(x,y,z,t)\parallel_{2}+\lambda_{1}\parallel\psi m(x,y,z)\parallel_{1}+\lambda_{2}\parallel TV m(t)\parallel_{1}$$$(1)
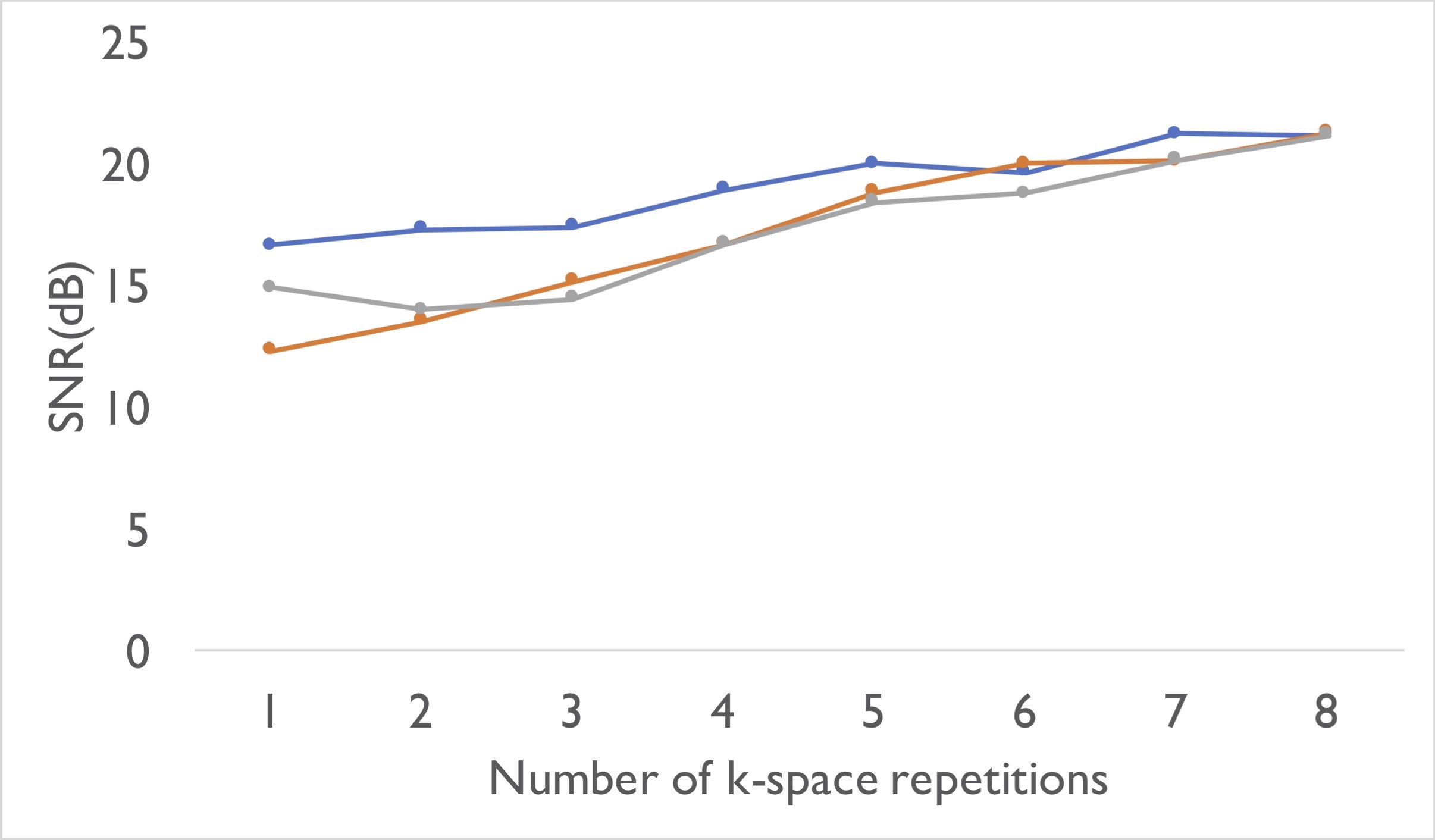
With D the sampling, F the Fourier-transform and S the ESPIRiT operators. Regularization terms were empirically determined ($$$\lambda$$$=0.001,$$$\lambda$$$=0.05) and the optimization was performed using an alternative direction method of multipliers (ADMM) algorithm. Individual repetition images were also reconstructed with a CS reconstruction removing the temporal-TV term from the regularization. Even though thermal SNR is very difficult to define and analyze due to the use of multi-array coils and PI-CS reconstruction, we measured a $$$SNR(dB)=20log_{10}(\frac{\mu}{RMS(\sigma)})$$$ with $$$\mu$$$ a mean kidney signal and $$$\sigma$$$ STD of background noise to assess the benefits of increased k-space coverage and comparing breathing strategies.
Results & Discussion
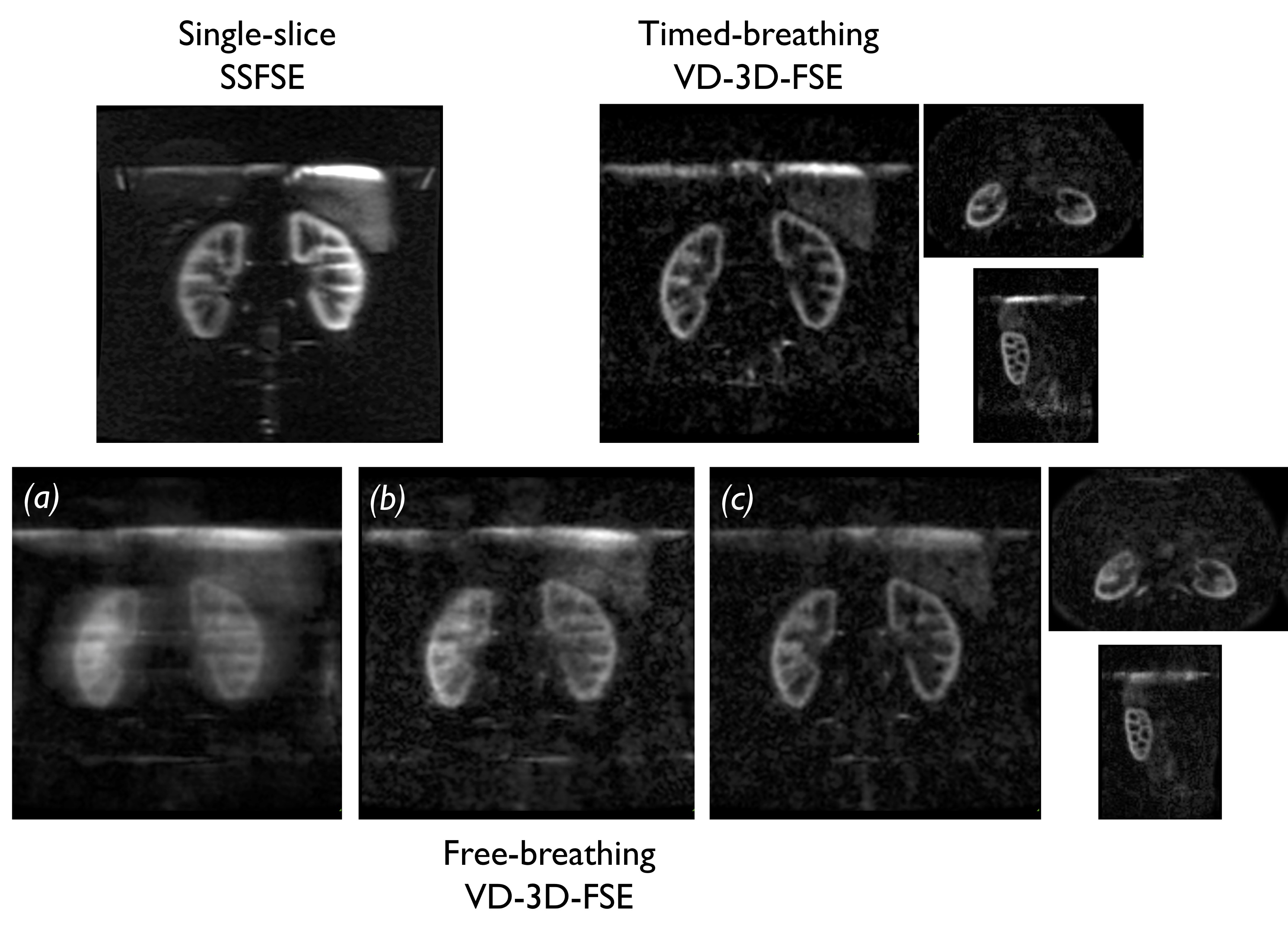
High quality whole kidneys perfusion imaging can be achieved using this variable-density 3D-FSE encoding, with an image quality comparable to our gold-standard motion-corrected single-slice-SSFSE (Fig.2). Interestingly, minimal image degradation was encountered in the free-breathing data and 4D-k-t-CS thanks to the higher temporal resolution achieved leading to increased bulk and physiological motion robustness. Minimal additional blurring can be observed in the kidneys on both original coronal and axial/sagittal reformats especially at the cortico-medullary interface.
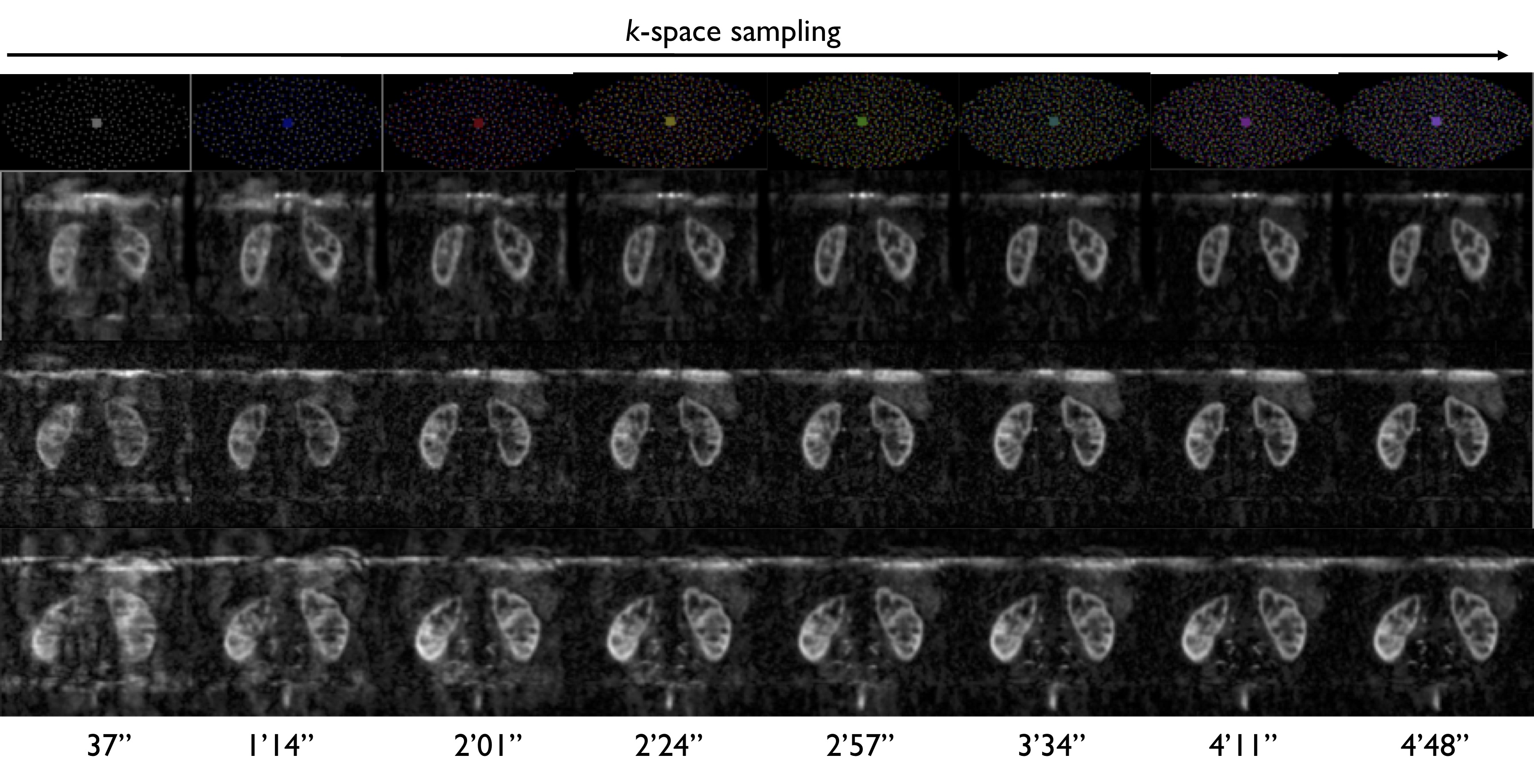
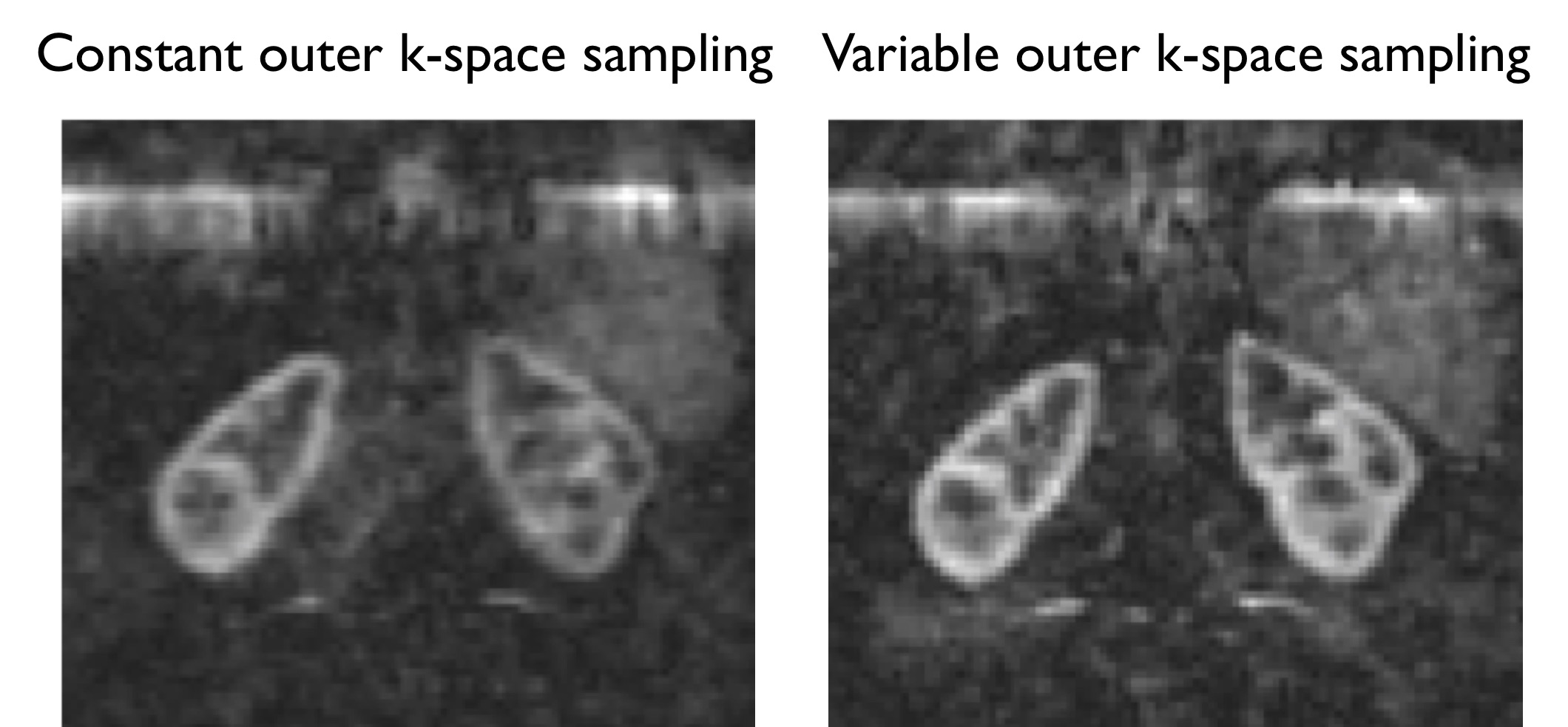
As seen in Fig.3, ASL image quality increases when the overall k-space coverage is extended by temporally varying the outer k-space undersampling and repeatedly sampling k-space center. However, the increase associated with denser outer k-space coverage is not linear (Fig.4), with a maximum SNR benefit between 3 and 6 repetitions. As seen on Fig.5, we can assume that both center oversampling and variable outer k-space coverage with 4D-CS provide motion robustness and reduced blurring. However, additional developments especially using additional motion compensation such as soft-gating7 or attempts to reconstruct heavily undersampled images for navigation8 should be considered to further improve the motion-robustness and image quality.
Conclusions
In conclusion, we have shown that whole kidneys isotropic free-breathing perfusion measurement using ASL is feasible in ≈5 minutes using a variable spatiotemporal density 3D-FSE acquisition with 4D-CS. This strategy provided high-quality perfusion images with minimal motion corruption in healthy volunteers. Future experiments should assess feasibility in uncooperative patient populations to assess image quality and benefits and/or pitfalls of free-breathing volumetric encoding to help in translating renal ASL into clinical practice.Acknowledgements
No acknowledgement found.References
1. Gardener, A. G. & Francis, S. T. Multislice perfusion of the kidneys using parallel imaging: image acquisition and analysis strategies. Magn. Reson. Med. 63, 1627–1636 (2010).
2. Taso, M., Guidon, A. & Alsop, D. C. Influence of background suppression and retrospective realignment on free-breathing renal perfusion measurement using pseudo-continuous ASL. Magn. Reson. Med. (2018), DOI 10.1002/mrm.27575.
3. Robson, P. M. et al. Volumetric Arterial Spin-labeled Perfusion Imaging of the Kidneys with a Three-dimensional Fast Spin Echo Acquisition. Acad. Radiol. 23, 144–154 (2016).
4. Uecker, M. et al. Berkeley Advanced Reconstruction Toolbox. in Proc. Intl. Soc. Mag. Reson. Med 2486 (2015).
5. Uecker, M. et al. ESPIRiT—an eigenvalue approach to autocalibrating parallel MRI: Where SENSE meets GRAPPA. Magn. Reson. Med. 71, 990–1001 (2014).
6. Cheng, J. Y. et al. Free-breathing pediatric MRI with nonrigid motion correction and acceleration. J. Magn. Reson. Imaging 42, 407–420 (2015).
7. Taso, M., Zhao, L., Guidon, A., Litwiller, D. V. & Alsop, D. C. Accelerated volumetric renal perfusion using pseudo-continuous ASL and a 3D Fast-Spin-Echo readout with Compressed Sensing. in Proceedings of the Joint annual meeting of the ISMRM-ESMRMB 3542 (2018).
8. White, N. et al. PROMO: Real-time prospective motion correction in MRI using image-based tracking. Magn. Reson. Med. 63, 91–105 (2010).
Figures