0697
Precision medicine advanced by full body imaging biomarkers, whole genomic sequencing and blood-based measures1Human Longevity, Inc., San Diego, CA, United States
Synopsis
We present the findings from 1190 presumed healthy patients evaluated at a precision medicine clinic. We performed deep quantitative multimodal phenotyping and genotyping comprising quantitative whole-body imaging, whole genome sequencing, and advanced blood-based biomarkers. Within this cohort, medically significant findings included aneurysms, newly identified tumors, coronary artery disease, metabolic disease, cardiac arrhythmia, myocardial disease, and neurodegenerative risk. Forty percent of “healthy” patients had a new clinically significant finding that was not previously known. For this 40%, we are able to provide quantitative continuous metrics that enable individuals to make informed decisions to mitigate their health risks.
Introduction
Despite the enormous cost of U.S. health care spending, 1 in 3 individuals aged 50-75 dies prematurely from age-related chronic diseases1. Increased early detection of disease has the potential to reduce this statistic. We report the results from four years of precision medicine conducted with presumed healthy individuals presenting without significant symptoms. This is the largest cohort of its kind and the only report to our knowledge that includes whole-body MRI (WB-MRI) and whole genome sequencing (WGS) in a presumed healthy cohort. We seek to evaluate this comprehensive, predictive, preventative, and personalized assessment of each individual’s health status.Methods
Our comprehensive phenotyping platform addresses seven major disease categories (Figure 1) and comprises:
Non-contrast MRI using 3T GE Discovery 750 or Siemens Skyra whole-body coil configuration:
Brain: 3D T1 MPRAGE/FSPGR–structural analysis/segmentation–post-processing with Neuroquant, 3D FLAIR–white-matter assessment, 2D DWI, T2* 2D GRE–blood product and calcification detection, 3D Time-of-Flight MRA–cerebrovascular disease;
Whole body: T1 Dixon imaging–(subset post-processed with AMRA), T2 SSFSE/HASTE, DWI (B1000 NSA=5, B0); Five stations (head, neck, chest, abdomen, pelvis)
Cardiac: 2,3,4 CH LAX CINE, SAX stacked cine imaging–cardiac structure and function;
Liver: Coronal HASTE/SSFSE–biliary tree, Multi-echo Dixon–liver fat and iron evaluation;
Prostate: Focused FOV T2, DWI (B1000 NSA=8, B0)–PIRADS staging.
Whole genome sequencing: 30x coverage–detection of disease-related genetic variants
CT using GE 64 slice revolution: Evaluation of coronary artery calcification (subset)
Ultrasound: 4D Echocardiogram–cardiac structure and function
Electrocardiogram/Ziopatch: Cardiac rhythm
Advanced blood biomarkers: Metabolome including insulin resistance (IR); bloodwork including CBCs, kidney and liver function tests, vitamin and hormone levels, a lipid panel, cancer tumor marker screening, heavy metal screening, and blood sugar.
Vital signs
Results
We identified medically significant findings (MSFs) in seven major disease categories: cancer/tumor, metabolic disorders, cardiovascular disease, myocardial heart disease, cardiac conduction disorders, neurodegenerative, and cerebrovascular.
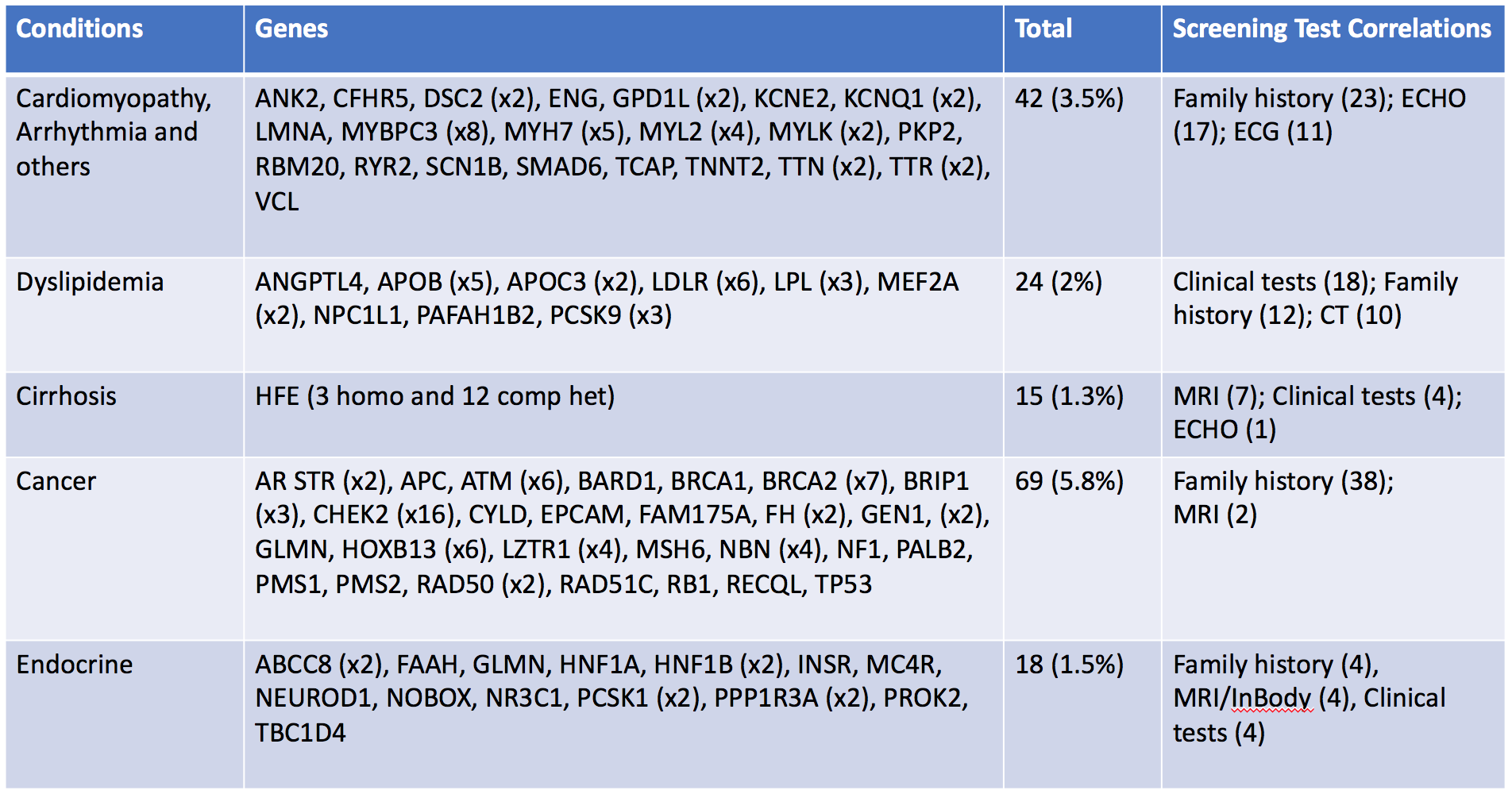
A significant proportion (24.3%) of participants had genetic MSFs relevant to risks of age-related chronic conditions. 206 unique variants in 111 genes were identified. Low to moderate penetrant variants, including F2, F5, ALDH2, comprised 7%. Clinical correlations with genomic findings were identified among 63.1% of individuals with high to moderate penetrance variants, suggesting the comprehensive platform significantly improves the diagnostic process in asymptomatic patients. Forty subjects had more than one MSF, and one subject had MSFs in four genes. 90.6% of subjects were found to be carriers for autosomal recessive conditions. A summary of MSFs correlated with other screening tests in selected diseases is reported in Figure 2.
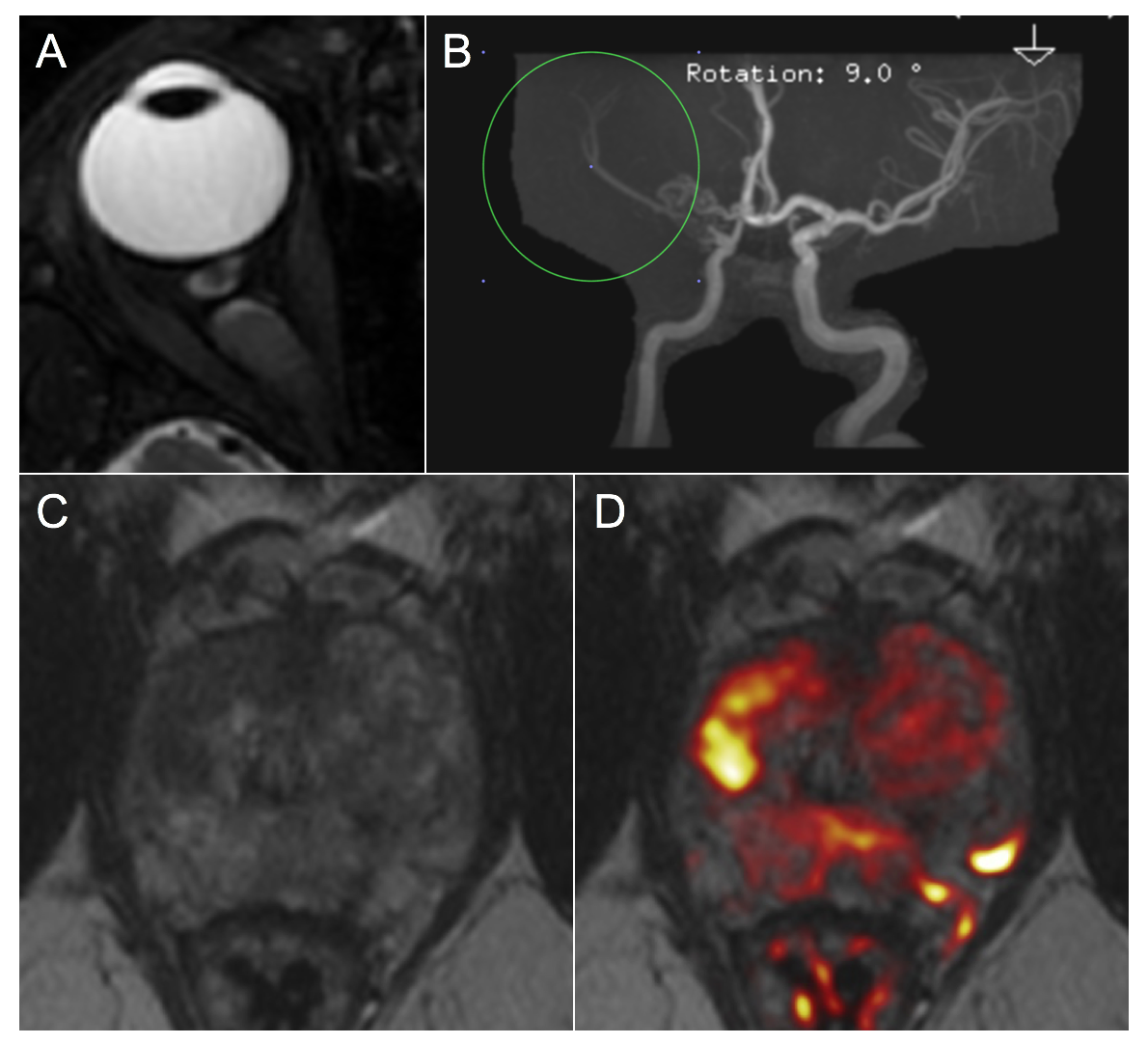
Phenotypic findings from imaging included previously unknown tumors, elevated R2*, elevated liver fat, elevated visceral adipose tissue, aortic and brain aneurysms, coronary artery calcification, arrhythmias and conduction disorders, aberrant cardiac structure/function, and low hippocampal occupancy score (Figure 3). Two examples of genetic variants (NF1 and AR STR) with significant MRI findings are illustrated in Figure 4.
22% of patients were referred for follow-up imaging based on MRI findings. However, given the international nature of the cohort, individuals may be lost to follow-up. Within this cohort, we are not aware of any false positive (FP) findings (Figure 3). Among the total of 2850 patients who have visited our clinic to date, we know of only two patients (prostate and mediastinal lymph node) for whom follow-up biopsies were benign.
Discussion/Conclusion
In this cohort of presumed healthy individuals presenting without symptoms, our data-driven precision health platform revealed a large portion who had significant findings. Extrapolating these findings to outcomes data based on the SEER cancer database and Global Burden of Disease1, we are adding 1-9 years of life in patients in whom we identified clinically significant actionable findings.
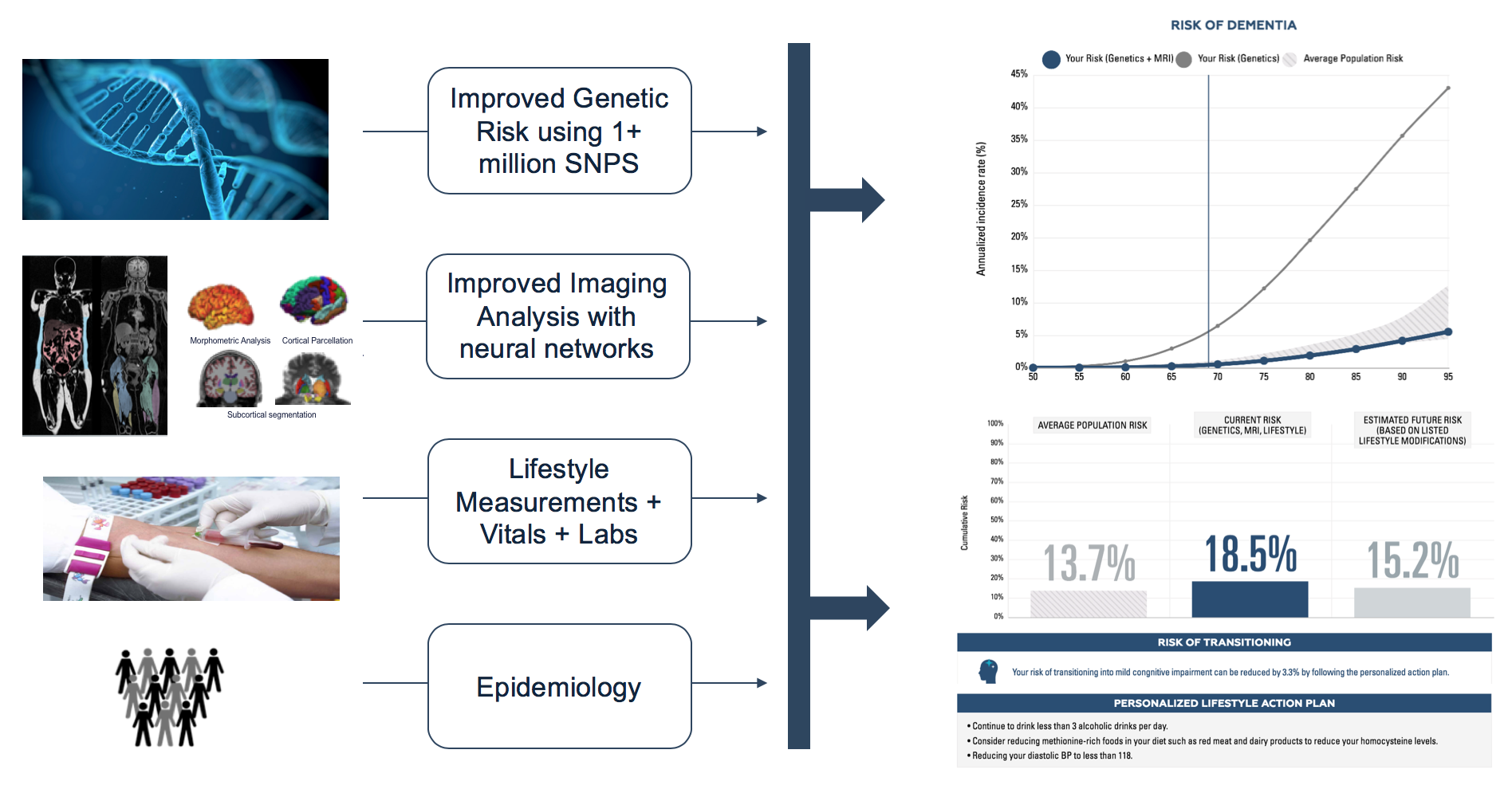
Our low FP rate is achieved through evaluation of imaging findings alongside genomic findings and deep phenotypic testing. WB-MRI based evaluation compared to CT allows for yearly non-invasive repeat analysis and exhibits inherently more soft tissue contrast, both of which decrease false positives. Furthermore, the use of Whole-body MRI and WGS goes beyond screening, providing continuous imaging and genomic biomarkers of chronic age-related disease risk in the form of integrated GWAS score and quantitative MRI biomarkers (Figure 5). Rather than utilizing a simple screening approach, we provide comprehensive, detailed analysis of each individual’s health status. With high-quality quantitative imaging biomarkers2,3 along with quantitative genetic and advanced blood biomarkers, in-depth analysis performed within each modality, and artificial intelligence models, we were able to cross-reference data across modalities, resulting in better quality and higher confidence diagnoses. The use of this analysis is currently being translated into clinical practice using integrated disease risk models that provide personalized assessments of individuals’ risks of developing dementia4, coronary artery disease, and diabetes5, providing high-risk individuals with ways to evaluate their health status and potentially mitigate their risk of disease progression using modifiable risk factors.
Acknowledgements
No acknowledgement found.References
- Vos T, Abajobir AA, Abbafati C, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017. doi:10.1016/S0140-6736(17)32154-2
- Wu J, Graff A, Deckman J, et al. Ultrafast Brain Segmentation using a 3D Fully Convolutional Neural Network for Risk Stratification of Cognitive Impairment. ISMRM. Submitted 2019.
- Graff A, Tkach D, Wu J, et al. Fully Automated 3D Body Composition Using Fully Convolutional Neural Networks and DIXON Imaging. ISMRM. Submitted 2019.
- Schenker-Ahmed NM, Swisher CL, Huang L, et al. Multimodal Models Provide Earlier Prediction of Dementia and Cognitive Decline and Personalized Actionability for Risk Mitigation for At-Risk Individuals. ISMRM. Submitted 2019.
- Bernal A, Schenker-Ahmed N, Karow D, Swisher CL. Predicting 10-Year Risk of Type 2 Diabetes Onset Using Lifestyle, Genomics, and Whole Body DIXON MR Imaging. ISMRM. Submitted 2019.
Figures