0696
First human imaging studies at 10.5 Tesla: body studies at 450 MHz1Center for Magnetic Resonance Research, University of Minnesota, Minneapolis, MN, United States, 2University of Minnesota, Minneapolis, MN, United States
Synopsis
This work presents the first in vivo human images from a whole body 10.5T MRI system. An initial coil was validated for safe operation at 10.5T allowing anatomic targets in the pelvis and abdomen to be explored. The translation of RF management strategies developed at 7T were employed to tackle the challenges at 10.5T demonstrating that high quality anatomic and quantitative data can be achieved at 450 MHz in the human torso.
INTRODUCTION
This work presents the first in vivo human images ever obtained on a 10.5T whole body MRI scanner. An imaging component was added to an ongoing safety study to explore the practicality and challenges of imaging the human body at 450 MHz where the short wavelengths inside the body (~8cm) create challenges with low transmit efficiency, poor homogeneity, and high local specific absorption rates (SAR). Imaging was performed with a previously published 10-channel fractionated-dipole transceiver torso body array1. As part of the investigation device exemption (IDE) to the FDA, the RF coil was validated2 and approved by the FDA prior to running in vivo studies. It was this validation process which led to a focus on the torso rather than the brain, since the uniform proximity of the elements to the body and consequently uniform loading of elements made validation more straightforward. Presented are initial studies imaging multiple targets in the torso to evaluate how well the methods developed at 7T translate to 10.5T, and to motivate continued development of human imaging at UHF.METHODS
MRI experiments were conducted on a whole-body 10.5T scanner (Siemens Healthcare, Germany) under an FDA and IRB approved protocol. The system is currently equipped with 32 receivers (to be upgraded to 128 receivers) and a 16 channel parallel transmit (pTx) system where each channel is driven by 2kW power amplifiers (Stolberg HF-Technik AG, Germany). The 10-channel dipole array was interfaced to the scanner by means of a 16-channel T/R box.
Electromagnetic simulations were performed in Ella, Duke and Fats29 virtual family human body models3 (Sim4Life, Zurich-Medtech, Zurich, Switzerland) at the level of the heart, kidneys and pelvis. The model sizes in terms of weight and BMI cover the range values encountered in vivo. B1+ shim solutions that maximized transmit efficiency were determined in the heart, kidney and pelvis4. For each model and target location the simulations were used to obtain the maximum 10g average SAR allowing for calculation of safe operating limits. In vivo imaging was performed in both male and female volunteers. In all studies, multi-slice B1+ shimming was performed through the anatomies of interest either during free breathing (pelvis) or during breath-hold (kidneys)4,5.
Prostate imaging provided an opportunity to acquire quantitative data; due to its size and limited motion, it was easy to calibrate power and achieve high transmit efficiency. These studies consisted of a combination of the following acquisitions in each subject: B1+ mapping using AFI6, T2w TSE for anatomy, T1 mapping using single-shot tubo-flash, T2 mapping using a CPMG mutli-echo sequence, and diffusion weighted imaging. Parametric mapping for T1 and T2 consisted of standard methods.
Bilateral hip imaging was performed to evaluate the performance of lipid suppression, the level of image uniformity across the pelvis and the ability to visualize the important structures of interest. Imaging studies consisted of rapid fat-suppressed gradient echo imaging and 3D isotropic multi-echo imaging data (i.e. MEDIC).
Kidney imaging included breath-hold, fat suppressed sequences to image the anatomy and in-flow sequences to observe in-flow enhancement to delineate the vessels.
Liver imaging was performed to test the limits of transmit homogeneity of static B1+ shimming methods and the importance/capabilities of pTx to obtain uniform contrast across the torso. Standard gradient echo acquisitions were used to compare static phase-only B1+ shimming with a homogeneous solution against one- and two-spoke pTx solutions7.
RESULTS
The peak local SAR values and derived time average power limits used for the studies are given in Fig.1. Peak average B1+ in the prostate is determined plotted as a function of subject size in Fig.2. Example anatomic and parametric maps of the prostate and quantitative results are in Fig.3. Anatomic hip and renal imaging are shown in Fig.4 along with non-contrast in-flow renal angiography studies. The role of pTx in the body at 10.5T is demonstrated in the liver in Fig.5.DISCUSSION / CONCLUSION
Multiple targets in the human body were successfully imaged with a variety of techniques. RF management strategies developed to image similar targets at 7T continue to work at 10.5T with increasing importance of pTx to obtain more uniform B1+ fields and contrast while simultaneously increasing SAR efficiency1, a concern limiting many of the acquisitions presented. To improve performance, a new 16 channel array has shown to have an increased transmit and SAR efficiency while providing access to 6 more 2kW RF amplifiers leading up to 50% more peak B1+ and more flexibility for the design and optimization of acquisition strategies. Validating this coil and streamlining pTx functionality will greatly enhance body imaging capabilities at 10.5T.Acknowledgements
Supported by: NIBIB P41 EB015894 and NIH S10 RR029672.References
1. Erturk, M. A., Wu, X., Eryaman, Y., Van de Moortele, P. F., Auerbach, E. J., Lagore, R. L., DelaBarre, L., Vaughan, J. T., Ugurbil, K., Adriany, G. & Metzger, G. J. Toward imaging the body at 10.5 tesla. (2017) Magn Reson Med 77, 434-443.
2. Hoffmann, J., Henning, A., Giapitzakis, I. A., Scheffler, K., Shajan, G., Pohmann, R. & Avdievich, N. I. Safety testing and operational procedures for self-developed radiofrequency coils. (2016) NMR Biomed 29, 1131-1144.
3. Christ, A., Kainz, W., Hahn, E. G., Honegger, K., Zefferer, M., Neufeld, E., Rascher, W., Janka, R., Bautz, W., Chen, J., Kiefer, B., Schmitt, P., Hollenbach, H. P., Shen, J. X., Oberle, M., Szczerba, D., Kam, A., Guag, J. W. & Kuster, N. The Virtual Family-development of surface-based anatomical models of two adults and two children for dosimetric simulations. (2010) Physics in Medicine and Biology 55, N23-N38.
4. Metzger, G. J., Snyder, C., Akgun, C., Vaughan, T., Ugurbil, K. & Van de Moortele, P. F. Local B1+ shimming for prostate imaging with transceiver arrays at 7T based on subject-dependent transmit phase measurements. (2008) Magn Reson Med 59, 396-409.
5. Metzger, G. J., Auerbach, E. J., Akgun, C., Simonson, J., Bi, X., Ugurbil, K. & van de Moortele, P. F. Dynamically applied B1+ shimming solutions for non-contrast enhanced renal angiography at 7.0 Tesla. (2013) Magn Reson Med 69, 114-126.
6. Yarnykh, V. L. Actual flip-angle imaging in the pulsed steady state: a method for rapid three-dimensional mapping of the transmitted radiofrequency field. (2007) Magn Reson Med 57, 192-200.
7. Wu, X., Schmitter, S., Auerbach, E. J., Uğurbil, K. & Van de Moortele, P.-F. Mitigating transmit B 1 inhomogeneity in the liver at 7T using multi-spoke parallel transmit RF pulse design. (2014) Quantitative Imaging in Medicine and Surgery 4, 4-10.
Figures
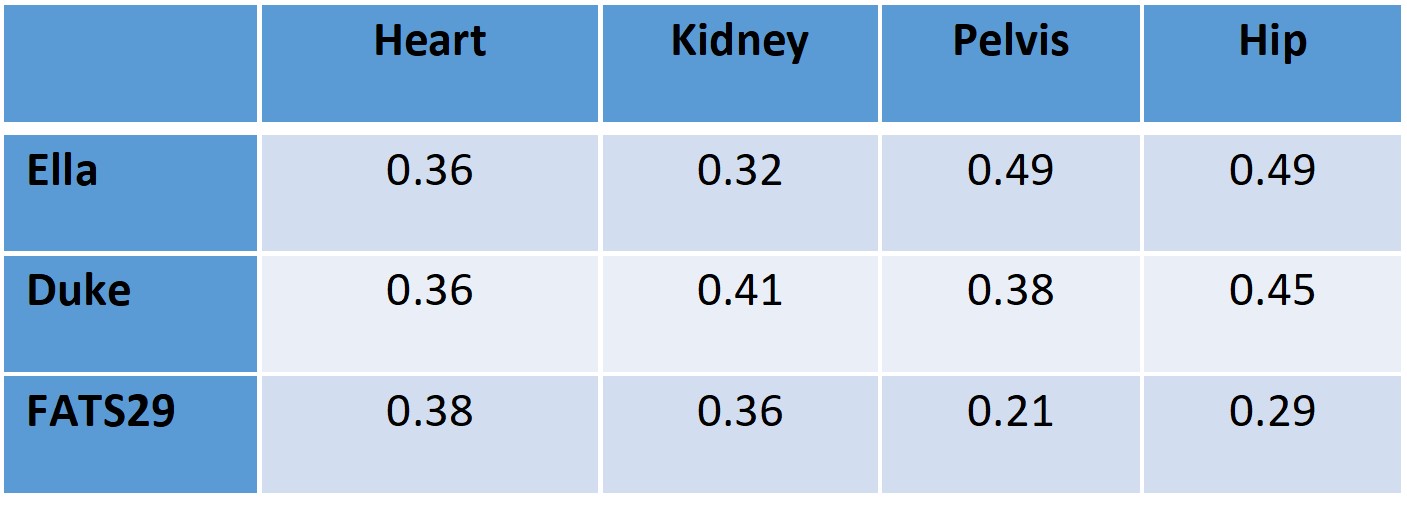
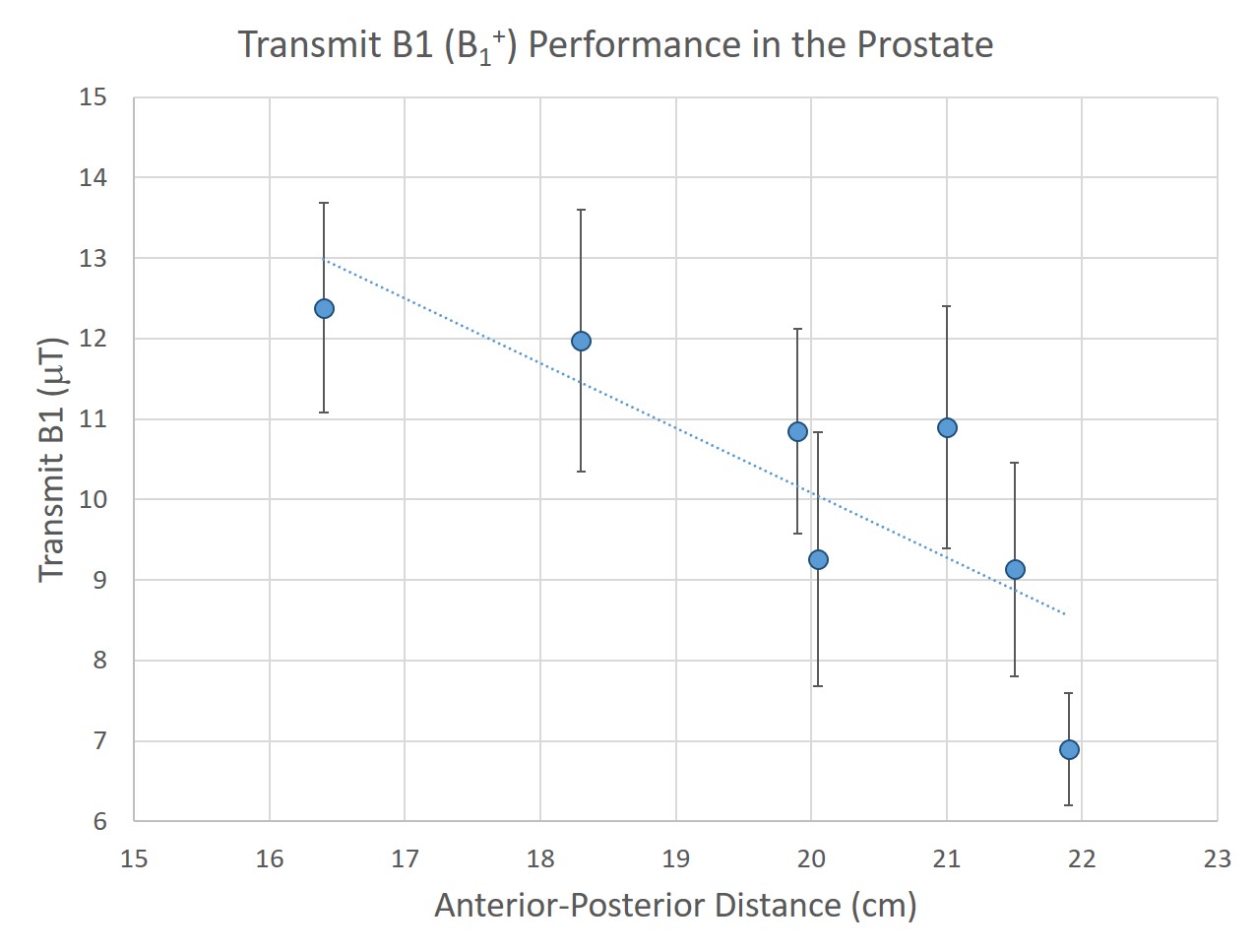
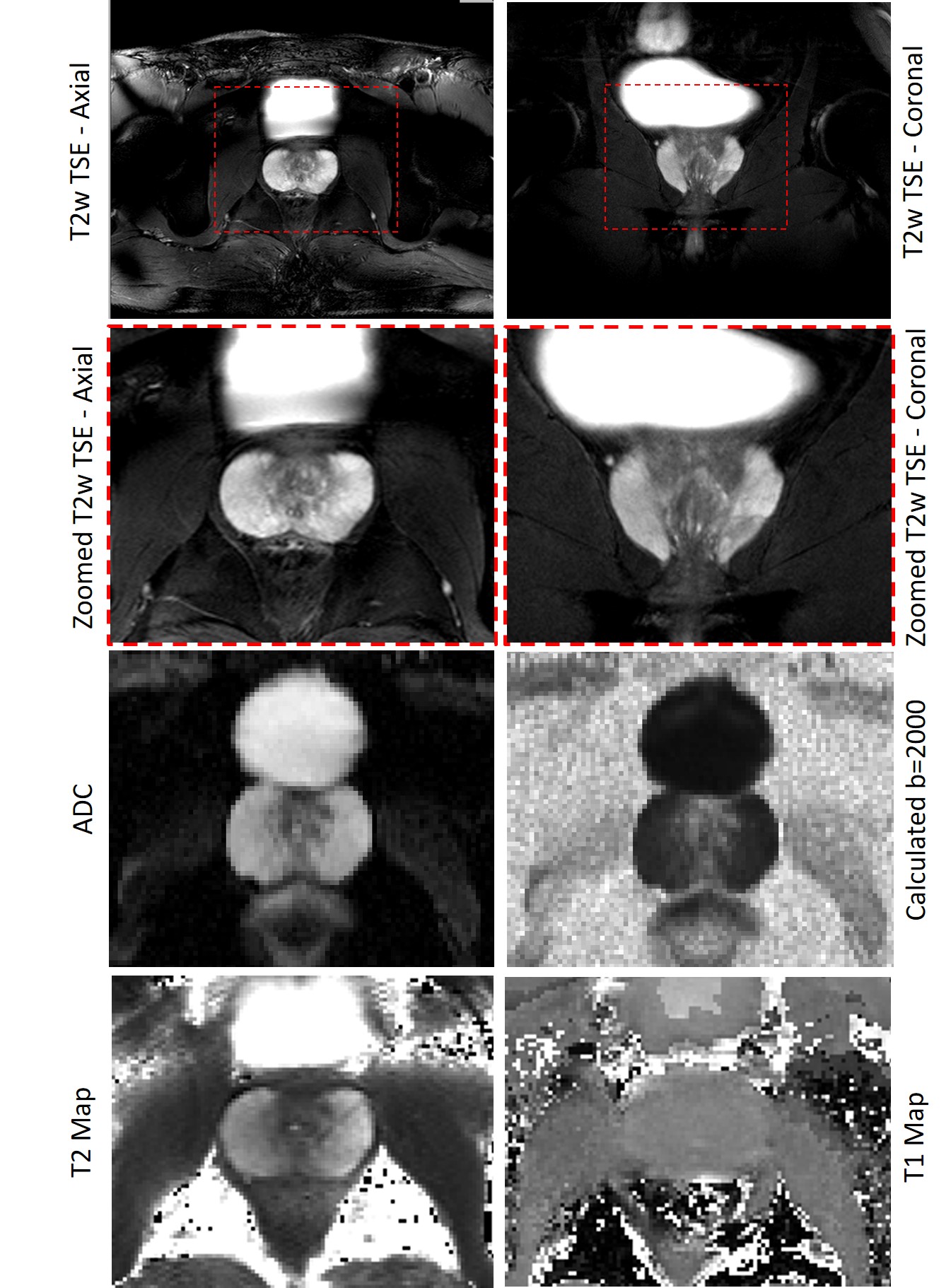
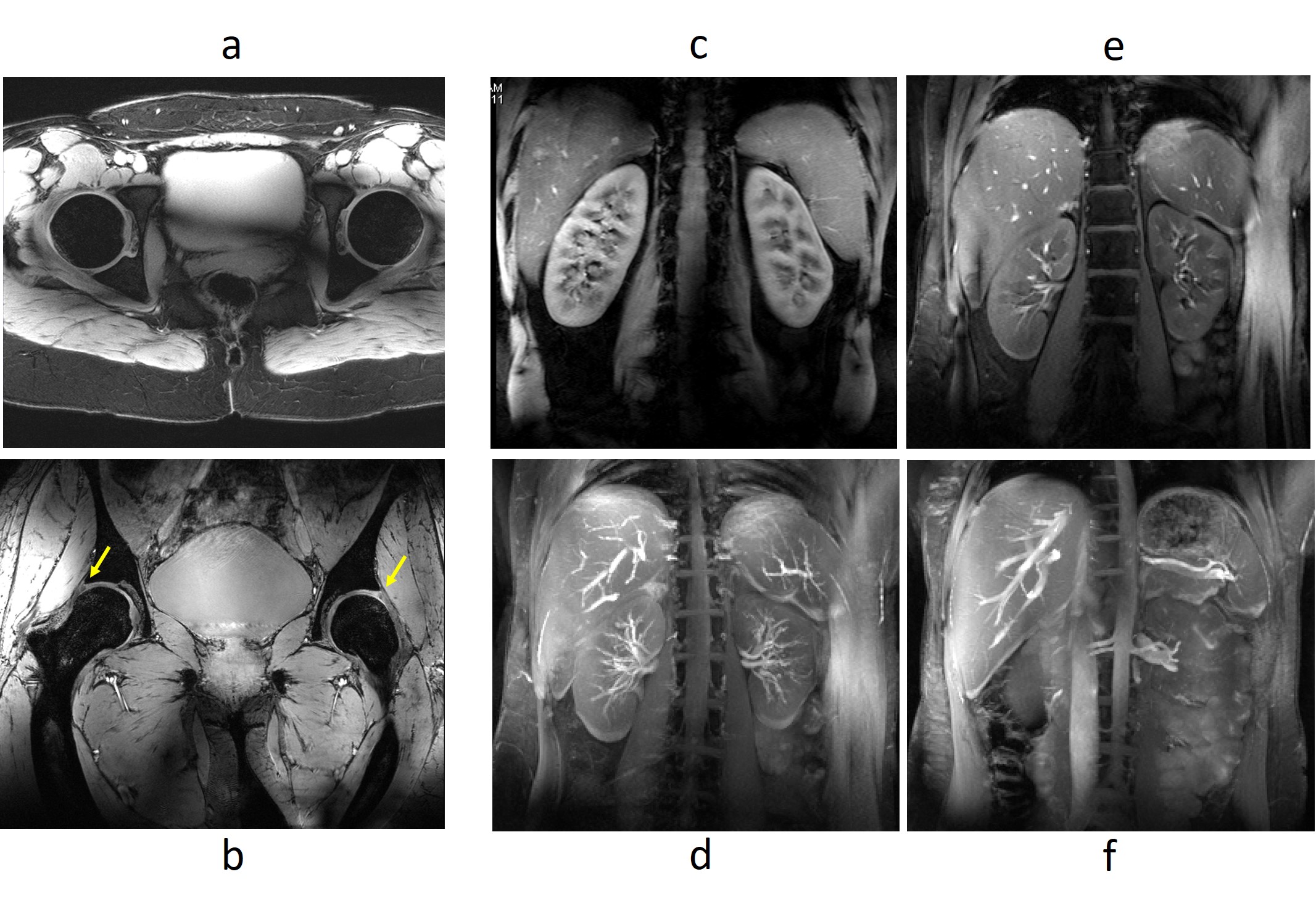
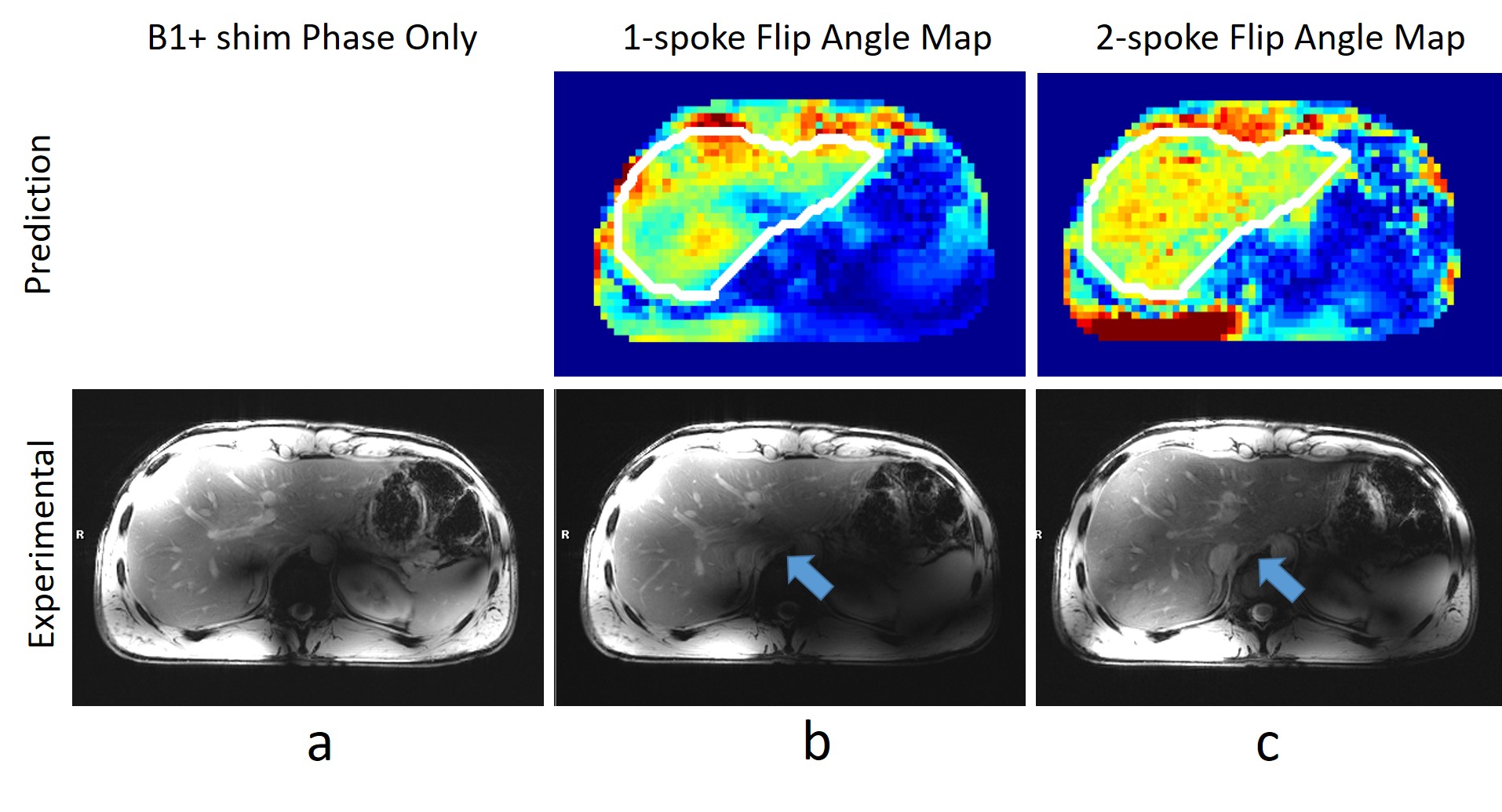
Fig.5: The demands of liver imaging at UHF require the effective management of B1+ fields. Static B1+ shimming (a,b) is insufficient to provide uniform B1+ and contrast. The B1+ shim phase only solution in (a) uses a uniform power across all channels. (b) Even when allowing the magnitude to vary across transmit channels in the 1-spoke solution, local destructive interferences cannot be resolved. (c) With the two-spoke solution however, a significantly more homogeneous flip angles are achieved providing improved contrast uniformity (blue arrow). Much of the remaining signal inhomogeneity is the results of an non-uniform receive profile.