0688
Ultra-High Resolution Whole-Brain DCE MRI makes Significant Difference in Estimating Permeability Maps for Cancer Patients1Sungkyunkwan University, Korea, Korea, Republic of, 2Seoul National University Hospital, Seoul, Korea, Republic of
Synopsis
An ultra-high resolution, whole-brain DCE MRI with a temporal resolution of 1.5sec (3~4 times higher than conventional routine) and a spatial resolution of isotropic 1.0mm3 (5~6 times higher than conventional routine) is introduced in a real clinical setting to address problems related to arterial input function and partial volumes for precise estimation of vascular permeability information in brain cancer patients. Compared with conventional routine vendor-provided method, the proposed ultra-high resolution DCE MRI produces significant differences in permeability maps particularly for both Ktrans and ve.
Introduction
Dynamic contrast enhanced (DCE) MRI has been widely used to obtain vascular information on permeabilities in the presence of blood-brain-barrier(BBB) leakages in pathological tissues with cancer,stroke etc1,2.In a clinical routine,a series of time-resolved 4D data in either the whole brain or a restricted region of interest1,2 were typically acquired with a temporal resolution of 4.8~6.0sec and a spatial resolution of 1.3x1.3x3.0mm3.Despite its partial success,the current state-of-the-art DCE-MRI is still not sufficient in accurately delineating rapidly varying arterial input signals(AIF) while avoiding partial volume effects, eventually precluding precise estimation of permeability information(e.g.Ktrans,ve,vp).Given the above considerations,we develop an ultra-high resolution whole-brain DCE-MRI technique in a real clinical setting that exploits prospective,highly undersampled and spatiotemporally constrained reconstruction, achieving a temporal resolution of 1.5 sec(3~4 times higher than conventional method) while attaining a spatial resolution of isotropic 1.0mm3(5~6 times higher than conventional method).Within our knowledge, this is the first work that demonstrates the feasibility of the ultrahigh resolution DCE-MRI(1.5sec,1mm3) in addressing both AIF and partial volume problems simultaneously.In-vivo experiments were performed in cancer patients to validate the effectiveness of the proposed method over conventional DCE-MRI.Materials and Method
Data Acquisition: A time series of 4D-DCE data were acquired in cancer patients on a 3.0 T MR-scanner(Skyra,Siemens) using the proposed ultra-high resolution DCE-MRI(1.5sec,1mm3) and conventional vendor routine(4.8sec,1.3x1.3x3.0mm3).Each set of 4D-data was vastly under-sampled in a radial-like pattern on a Cartesian grid (R=50) and then shared only in a portion of peripheral k-space over three neighboring phases.Imaging parameters common to both the proposed and conventional methods were: TR/TE=3.18/1.1ms,flip angle=15◦,matrix size=192×192×144,temporal phases=170.Variable-flip-angle Imaging(2°,8°,15°) was performed to estimate a reference T10 map3.
Spatiotemporally Constrained Reconstruction: The proposed DCE-MRI signal X is decomposed into:
$$\bf X=X_{0}+X_{D}+X_{M}+N$$
X0 is the baseline signal matrix,XD is the matrix of interest that contains time-varying contrast agent induced signals,and XM is the residual signal matrix.The proposed DCE reconstruction is performed by solving the following spatiotemporally constrained optimization problem:
$${{ \{ \hat{\bf{X}}_{D}, \hat{\bf{U}},\hat{\bf{X}_{M}} \}}=\underset{\bf{X}_{D},\bf{U},\bf{X}_{M}}{\mathrm{arg\;min}}\;\left \|\bf{D}_{t}\bf{X}_{D}\right\|_{\mathrm{1}}+\mathrm{\lambda_{U}}\left \| \bf{D}_{s}\bf{U}\right \|_{\mathrm{1}}+\mathrm{\lambda_{M}} \left \|\psi\bf{X}_{M}\right \|_1}$$
$${s.t.\bf{d}_{r}=\ \tt\bf{E}(\bf{X}_{D}+\bf{X}_{M}),\space \bf{X}_{D}=\bf{U}\bf{V}_{r}}$$
where Dt is the temporal finite difference operator,Ds is the spatial finite difference operator,dr is the residual(k-t space) between the baseline and DCE data,$$$\psi$$$ is temporal Fourier transform operator,and E is the sensitivity encoding operator,Vr denotes the temporal basis.
DCE Emulation and Permeability Quantification: A high definition reference data is available from the proposed ultra-high resolution DCE-MRI.To emulate a series of data with varying temporal resolution(1.5 to 10.5sec), a corresponding range of k-space data in neighboring time phases were shared.A series of data with varying spatial resolution(1x1x1 to 4x4x1mm3) was then emulated by low pass filtering the reference data.For each set of data,permeability information was quantified by the following procedures:1)T10 and T1 maps were generated and then converted to concentration time courses voxel by voxel; 2)AIF was manually measured in the internal carotid artery; and 3)Given the AIF and the tissue concentration time course, permeability information was quantified by exploiting the extended tofts model and corresponding non-linear least squares fitting4.Permeability maps were compared with varying temporal and spatial resolutions from the emulated sets of data.
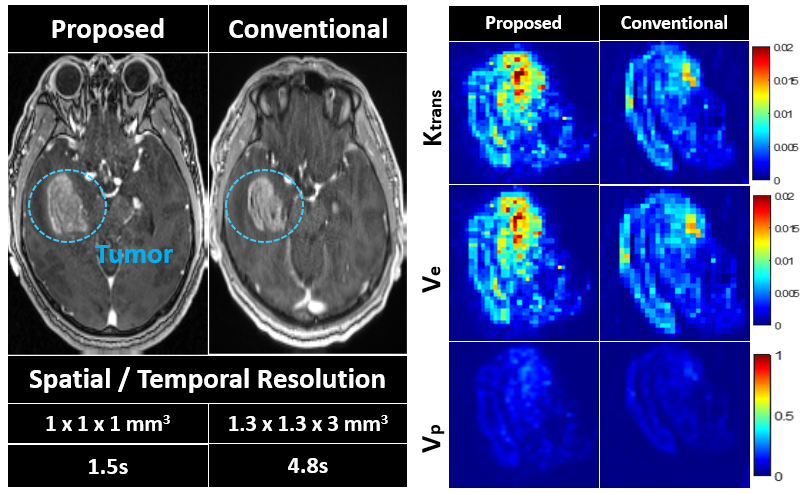
Direct Comparison between the Proposed Ultra-High DCE MRI and Conventional Routine MRI in a real clinical setting: To validate the feasibility of the proposed, ultra-high resolution DCE-MRI in a real clinical setting, two sets of DCE-MRI data obtained using the proposed method(1.5sec,1mm3) and conventional vendor routine(4.8sec,1.3x1.3x3.0mm3) were used to construct permeability maps for comparison.
Result
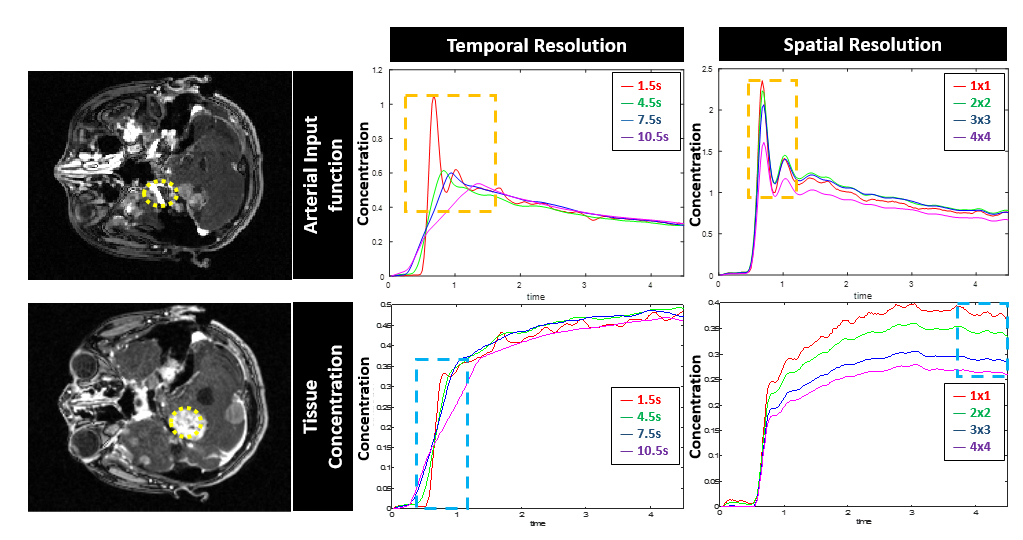
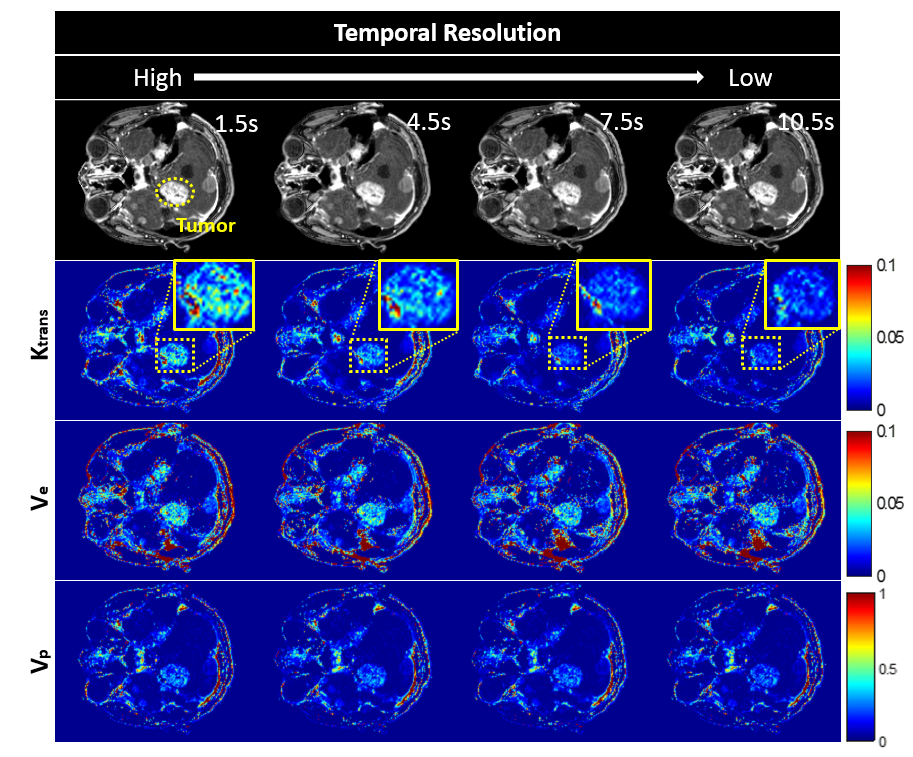
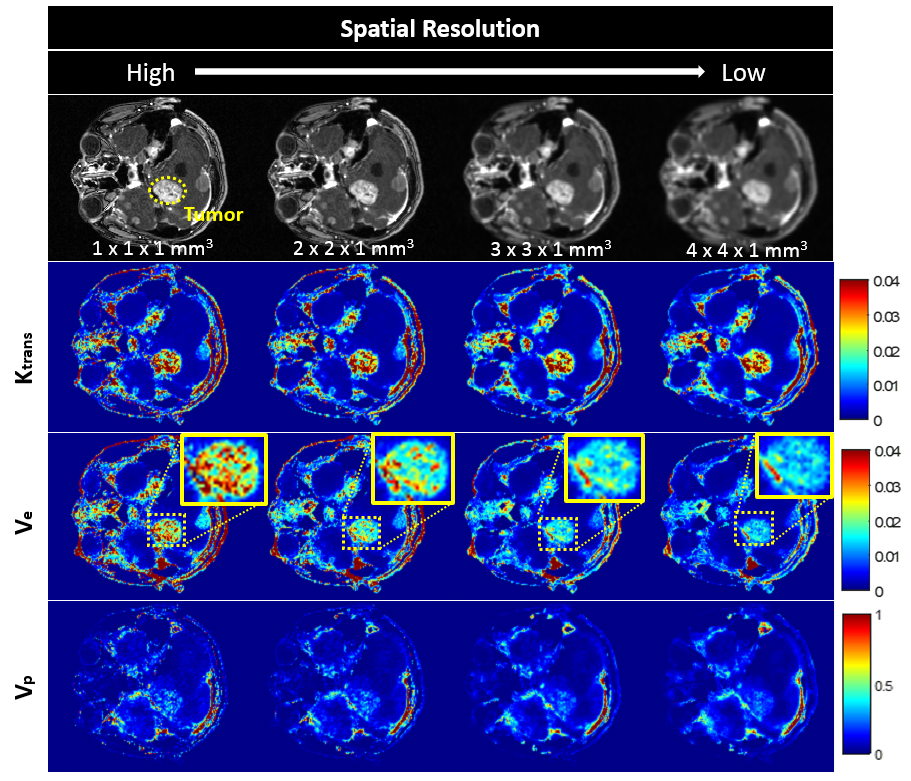
Fig.1 represents delineation of AIF and tissue concentration time courses in two corresponding ROIs with varying temporal and spatial resolution. A portion of AIF peak is accurately delineated at a temporal resolution of 1.5sec and a spatial resolution of 1.0mm3 while being blurred with decreasing resolution (brown-dotted box)(Fig.1,first row).An initial portion of tissue concentration time course is heavily affected by temporal resolution while a later saturated portion of the corresponding time course is highly sensitive to spatial resolution(blue-dotted box)(Fig.1,second row).Fig.2 demonstrates that Ktrans is highly sensitive to temporal resolution.A temporal resolution of 1.5sec makes substantial difference in Ktrans compared with that of even 4.5sec.Fig.3 shows that ve is highly sensitive to spatial resolution. A spatial resolution of 1mm3 makes substantial difference in ve compared with that of even 2x2x1mm3.In Fig.4,the proposed method yields much sharper delineation of cancer structures in the raw image and much more sensitive delineation of permeability maps than conventional routine DCE-MRI.Conclusion
We successfully demonstrated that compared with conventional routine vendor-provided method, the proposed,ultra-high resolution DCE-MRI makes substantial difference in Ktrans and ve by accurately delineating AIF and tissue concentration time courses without apparent partial volume effects.Clinical utilities of the proposed method need to be further validated in a large group of patient studies in the future.Acknowledgements
NRF-2017R1A2B4012581, NRF-2018M3C7A1056887, NRF-2016M3C7A1913844References
1.MING ZHAO: Quantitative analysis of permeability for glioma grading using dynamic contrast enhanced magnetic resonance imaging. ONCOLOGY LETTERS 14:5418-5426,2017
2.Vaios Hatxoglou: Dynamic contrast-enhanced MRI perfusion for differentiating between melanoma and lung cancer brain metastases.Cancer Medicine 2017,6(4):761–767.
3.Sean C.L Deoni, PhD: High-Resolution T1 and T2 Mapping of the Brain in a Clinically Acceptable Time with DESPOT1 and DESPOT2.Magn Reson in Med 2005;53:237–241
4.Steven P. Sourbron, David L. Buckley: On the Scope and Interpretation of the Tofts Models for DCE-MRI. Magn Reson in Med.2011;66:735–745
Figures