0682
How tumour pressure components are related to tumour blood perfusion and mechanical properties1Laboratory of Imaging Biomarker, INSERM-University Paris Diderot, Paris, France, 2Sanofi, Vitry sur seine, France, 3Department of Radiology, Beaujon University Hospital Paris Nord, Clichy, France
Synopsis
The purpose of this study was to assess the influence of
INTRODUCTION
Solid stress and interstitial fluid pressure (IFP) are both components of the total tumour pressure (TTP)1. These components are important biomarkers of the tumour severity by compressing tumour vessels, reducing the efficacy of chemotherapeutic agents and immunotherapy, and promoting tumour progression2-5. Knowledge of the importance of IFP and solid stress on tumour pressure could help to improve treatments, however, their influences on pressure are still debated6, 7. Also, separation of solid stress and fluid pressure could provide information on how each component influences tumour behaviour such as its blood perfusion or stiffness. In this study, we propose to measure pressure in an in-vivo xenograft tumour model and assess at MRI the influence of each pressure component on tumour mechanical properties and perfusion.
METHODS
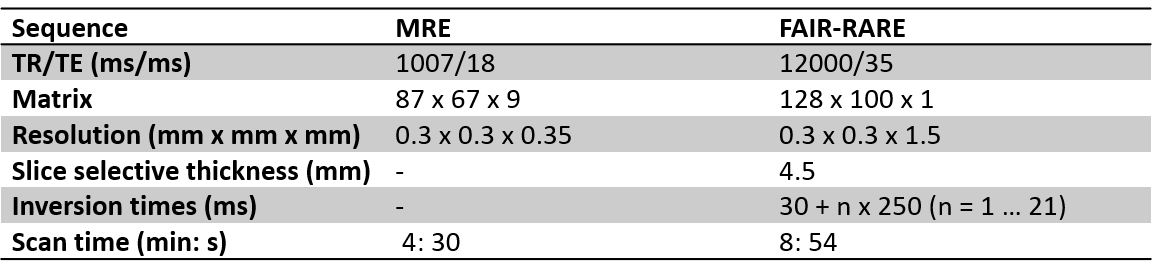
MRI examinations were performed in 19 SCID mice with subcutaneous tumours (patient-derived hepatocellular carcinoma xenografts) implanted in the right flank. A 7T MRI scanner (Pharmascan, Bruker, Germany) with a volume resonator and a 2 mm diameter receiver coil was used. Mechanical vibrations were generated with a uniaxial acoustic shaker and transmitted to the tumours via a rigid carbon fiber rod linked to a 3D-printed plastic insert8. MR acquisitions were performed on tumours with an average volume of 832 ± 343 mm3. MR elastography and MR FAIR perfusion acquisitions were performed on each mouse with the parameters showed in Table 1. Mechanical vibrations were generated at 600 Hz and synchronized with a sinusoidal motion-encoded spin echo sequence. MRE acquisitions were performed in three spatial directions and included four times steps. Maps of G*, G’ and G’’ were obtained by inversion of the Helmholtz wave equation9. Once the MR acquisitions were performed the mice were placed outside the MR system and the TTP was measured using a catheter-mounted piezoelectric pressure transducer (SPR-1000 Mikro-Tip, Millar Instruments, Houston, USA). The IFP was also measured for each mouse, following the method developed by Nieskoski et al.10. The pressure catheter was covered with a perforated 24-gauge polytetrafluoroethylene sheath (Cole-Parmer, Vernon Hills, USA) to isolate the probe from the solid stress and only let the fluid carry pressure onto the probe through the perforations. All measures were taken in the same position at the centre of the tumour. Then, solid stress was calculated for each mouse by subtracting the IFP from the TTP. Mechanical properties and tumour perfusion were observed relative to the different tumour components.RESULTS
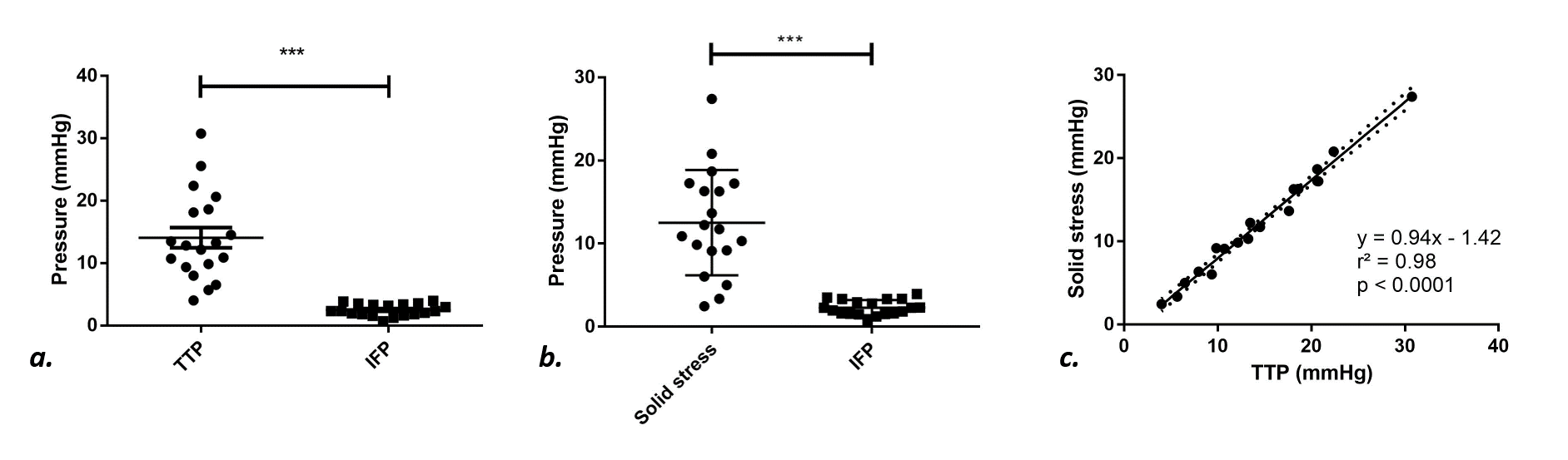
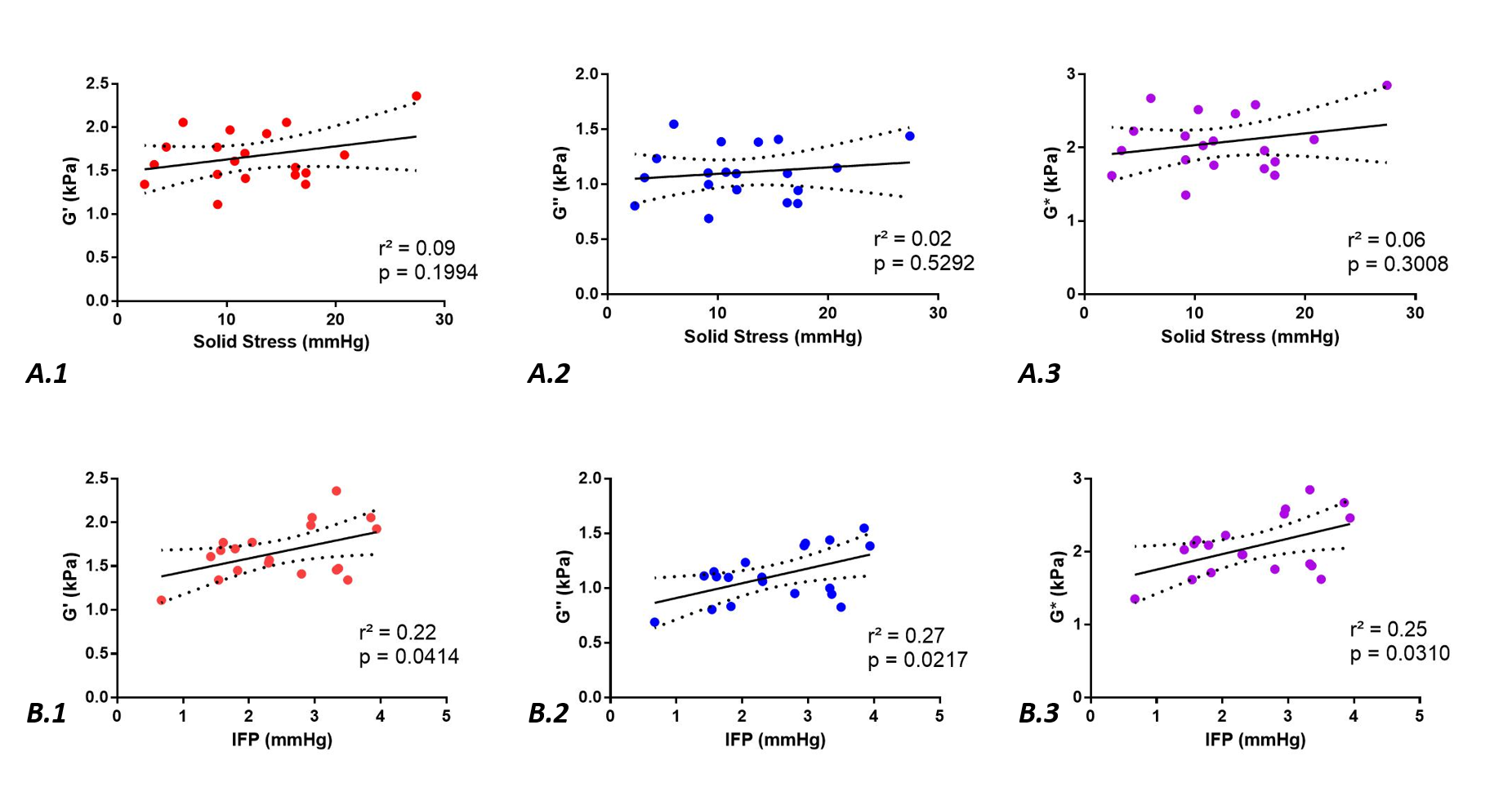
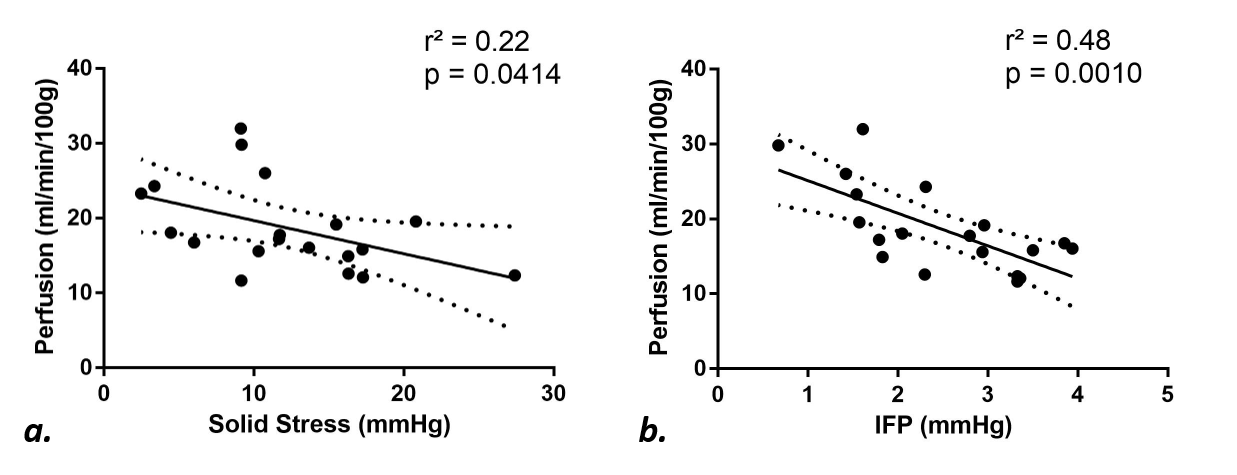
The average TTP, solid stress and IFP were measured at 14.67 ± 6.55 mmHg, 12.24 ± 6.27 mmHg and 2.43 ± 0.94 mmHg, respectively. A significant difference was observed between TTP and IFP (p < 0.0001, Fig.1.a.) and between solid stress and IFP (p < 0.0001, Fig.1.b.). Also, a strong correlation was noticed between solid stress and TTP, with the slope of the regression line close to 1 (Fig.1.c). No correlations were observed between solid stress and IFP. The average G*, G’ and G’’ were measured at 2.07 ± 0.40 kPa, 1.66 ± 0.31 kPa and 1.11 ± 0.24 kPa, respectively. Significant correlations were observed between the mechanical properties of the tumours and their IFP, but not between the mechanical properties and the solid stress (Fig.2). Tumour perfusion was measured at 18.68 ± 5.89 ml/min/100g and correlated significantly with both solid and fluid pressures (Fig.3).DISCUSSION
The results suggest that in hepatocellular carcinomas, the pressure is mainly generated by the solid stress rather than the IFP. Similar results were observed in human pancreatic adenocarcinoma10. Also, as previously described in other tumour types3, solid stress and IFP are two independent tumour components. Blood perfusion seems not to be only influenced by solid stress as suggested previously6, but high IFP can also be associated with decreased perfusion, as observed here. Presence of hyaluronan in the extracellular matrix could be responsible for the effect of high IFP on blood perfusion11. The mechanical properties are correlated to fluid pressure (IFP), as reported previously at ultrasonography12, 13. Finally, as observed with other methods14, elevated solid stress and stiffness are two distinct biomechanical characteristics.CONCLUSION
In conclusion, this study shows that in hepatocellular carcinoma the major component of the tumour pressure is the solid stress, hence therapeutic strategies aiming to decrease tumour pressure should be focused on solid components. However, tumour mechanical properties are distinct from solid stress and are instead linked to IFP, which also seems to have an influence on blood perfusion. High IFP could decrease blood perfusion and be an obstacle to drug delivery. Solid stress also diminishes perfusion, but through a mechanism that is independent from tumour mechanical properties.Acknowledgements
This project has received funding from the European Union's Horizon 2020 research and Innovation programme under grant agreement No 668039.
This work was performed by a laboratory member of France Life Imaging network (grant ANR-11-INBS-0006).
The authors would like to thank the FRIM UMS platform (Inserm, Diderot University, Bichat, Paris).
References
1. Jain RK, Martin JD, Stylianopoulos T. The role of mechanical forces in tumor growth and therapy. Annual Review of Biomedical Engineering 2014;16:321-346.
2. Jain RK. Normalizing tumor microenvironment to treat cancer: bench to bedside to biomarkers. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology 2013;31:2205-2218.
3. Mitchell MJ, Jain RK, Langer R. Engineering and physical sciences in oncology: challenges and opportunities. Nature Reviews Cancer 2017;17:659-675.
4. Padera TP, Stoll BR, Tooredman JB, et al. Pathology: cancer cells compress intratumour vessels. Nature 2004;427:695.
5. Kalli M, Papageorgis P, Gkretsi V, et al. Solid Stress Facilitates Fibroblasts Activation to Promote Pancreatic Cancer Cell Migration. Annals of Biomedical Engineering 2018;46:657-669.
6. Chauhan VP, Boucher Y, Ferrone CR, et al. Compression of pancreatic tumor blood vessels by hyaluronan is caused by solid stress and not interstitial fluid pressure. Cancer Cell 2014;26:14-15.
7. DelGiorno KE, Carlson M, Osgood R, et al. Interstitial pressure and vascular collapse in pancreas cancer: fluids and solids, measurement and meaning. Cancer cell 2014;26:16-17.
8. Ronot M, Lambert SA, Wagner M, et al. Viscoelastic Parameters for Quantifying Liver Fibrosis: Three-Dimensional Multifrequency MR Elastography Study on Thin Liver Rat Slices. PLOS ONE 2014;9:e94679.
9. Sinkus R, Tanter M, Xydeas T, et al. Viscoelastic shear properties of in vivo breast lesions measured by MR elastography. Magnetic Resonance Imaging 2005;23:159-165.
10. Nieskoski MD, Marra K, Gunn JR, et al. Separation of Solid Stress From Interstitial Fluid Pressure in Pancreas Cancer Correlates With Collagen Area Fraction. Journal of Biomechanical Engineering 2017;139.
11. Provenzano PP, Cuevas C, Chang AE, et al. Enzymatic targeting of the stroma ablates physical barriers to treatment of pancreatic ductal adenocarcinoma. Cancer Cell 2012;21:418-429.
12. Gennisson J-L, Grenier N, Combe C, et al. Supersonic shear wave elastography of in vivo pig kidney: influence of blood pressure, urinary pressure and tissue anisotropy. Ultrasound in Medicine & Biology 2012;38:1559-1567.
13. Rotemberg V, Palmeri M, Nightingale R, et al. The Impact of Hepatic Pressurization on Liver Shear Wave Speed Estimates in Constrained vs. Unconstrained Conditions. Physics in Medicine and Biology 2012;57:329-341.
14. Nia HT, Liu H, Seano G, et al. Solid stress and elastic energy as measures of tumour mechanopathology. Nature Biomedical Engineering 2017;1:0004.
Figures