0664
Rapid Reconstruction of Accelerated, Free-Breathing, Thoracic, Non-Contrast Magnetic Resonance Angiography using Convolutional Neural Network1Department of Radiology, Northwestern University, Chicago, IL, United States, 2Department of Biomedical Engineering, Northwestern University, Evanston, IL, United States, 3Department of Computer Science & Engineering, Northwestern University, Evanston, IL, United States
Synopsis
In this study we developed a convolutional neural network (CNN) for reconstructing 3D non-contrast magnetic resonance angiography (NC-MRA) images. We trained our proposed CNN using 4,800 zero-filled images and the corresponding GRASP reconstructed images from 10 patients as input and output, respectively. For validation, we used 6,720 zero-filled images from 14 patients as input to our trained CNN. Comparison between CNN and GRASP reconstructions showed excellent agreement using quantitative metrics and quantified aortic diameters . The mean reconstruction time, excluding the pre- and post-processing steps, for CNN (74 s) was 99% shorter than GRASP (12,703 s).
Introduction
Non-contrast magnetic resonance angiography (NC-MRA)1,2 is an alternative to contrast-enhanced MRA for evaluation of thoracic aortic aneurysms (TAAs). The clinical translation of thoracic NC-MRA based on 3D balanced steady-state precession (b-SSFP) with T2-preparation and fat suppression1,2 has been hampered due to low spatial resolution (mean spatial resolution of 1.6 mm x 1.6 mm x 2.9 mm) and long scan times (mean scan time of 9 min 10 sec).3-5 In response, we developed a thoracic NC-MRA method using a combination of radial stack-of-star k-space sampling and Golden-angle Radial Sparse Parallel MRI (GRASP)6 reconstruction, in order to achieve a high spatial resolution (1.5 mm x 1.5 mm x 1.5 mm) at a clinically acceptable scan time (6 min).7 Although the proposed NC-MRA is clinically acceptable from an imaging perspective, the image reconstruction time (~5 hours) was deemed too slow for clinical translation. Convolutional neural networks (CNNs)8 are powerful image processing tools that have been shown to successfully reconstruct MRI images.9-12 The purpose of this study was to construct, train, and validate a convolutional neural network (CNN) for reconstructing 3D non-contrast magnetic resonance angiography (NC-MRA) images with high fidelity at a clinically acceptable reconstruction time (~1 min).Methods
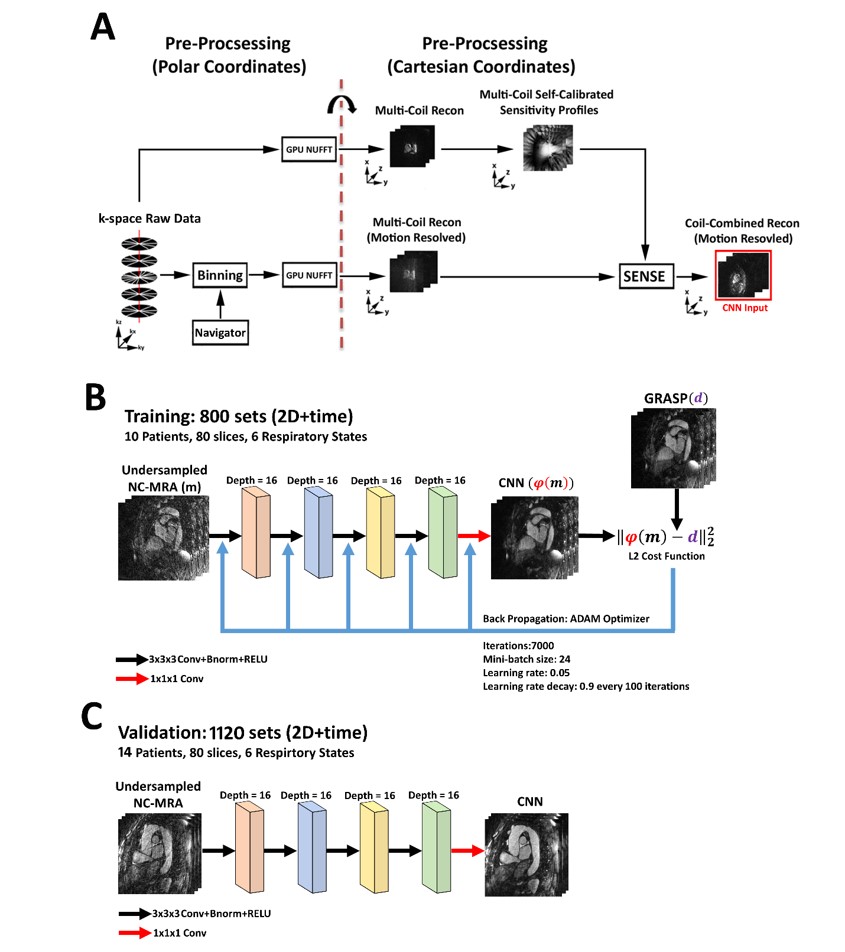
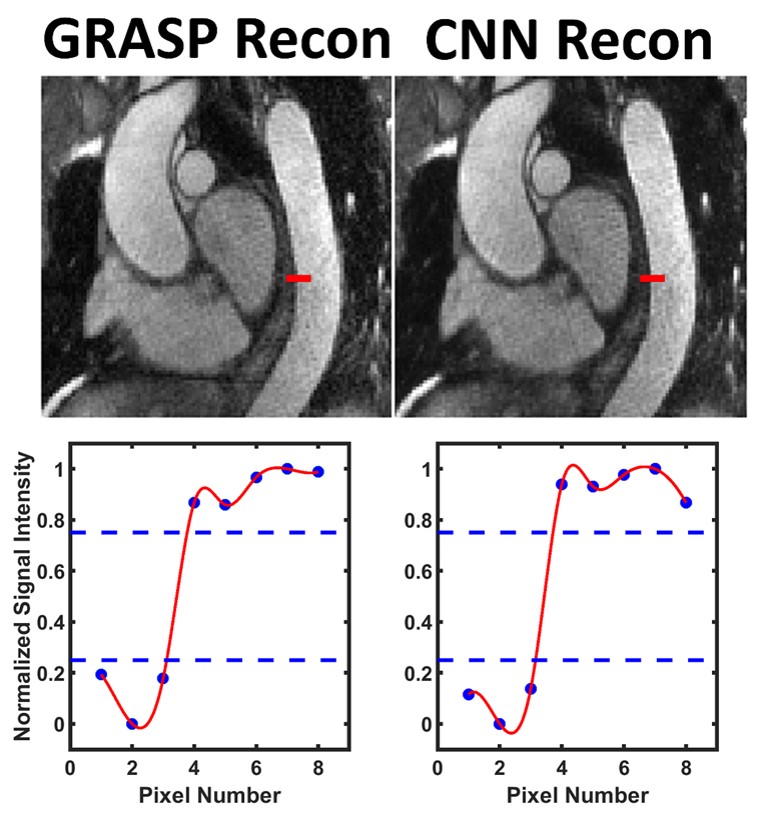
We acquired thoracic NC-MRA data from 24 patients (18 males, mean age=56.8 ± 11.8 years) with FOV=288x288x120mm3, acquisition matrix=192x192x80, and scan time=350 heart beats. For more details on the image acquisition and self-navigation of respiratory motion within the GRASP reconstruction framework, please see reference.7 GRASP reconstruction was performed on a workstation equipped a CPU (6 cores) and 128 GB of RAM. We built a CNN with 4 layers and a 3x3x3 convolutional kernel to achieve the stated objective. Our CNN was implemented on a different workstation equipped a GPU card (P100 Tesla) and Python with TensorFlow. As shown in Figure 1, our CNN framework included a pre-processing step where stack-of-stars k-space data were gridded onto a Cartesian space using GPU based NUFFT.13 For training, we used 4,800 zero-filled images and the corresponding GRASP reconstructed images from 10 patients as input and output, respectively. For validation, we used 6,720 zero-filled images from 14 patients as input to our trained CNN, and compared the CNN results against those by GRASP using quantitative metrics (DSC, SSIM, NRMSE, edge sharpness assessment [see Figure 2 for example], SNR). To evaluate the impact of data fidelity on clinical task, aortic diameters were measured at seven standardized locations of thoracic aorta.14 Appropriate statistical tests were conducted to compare two groups.Results
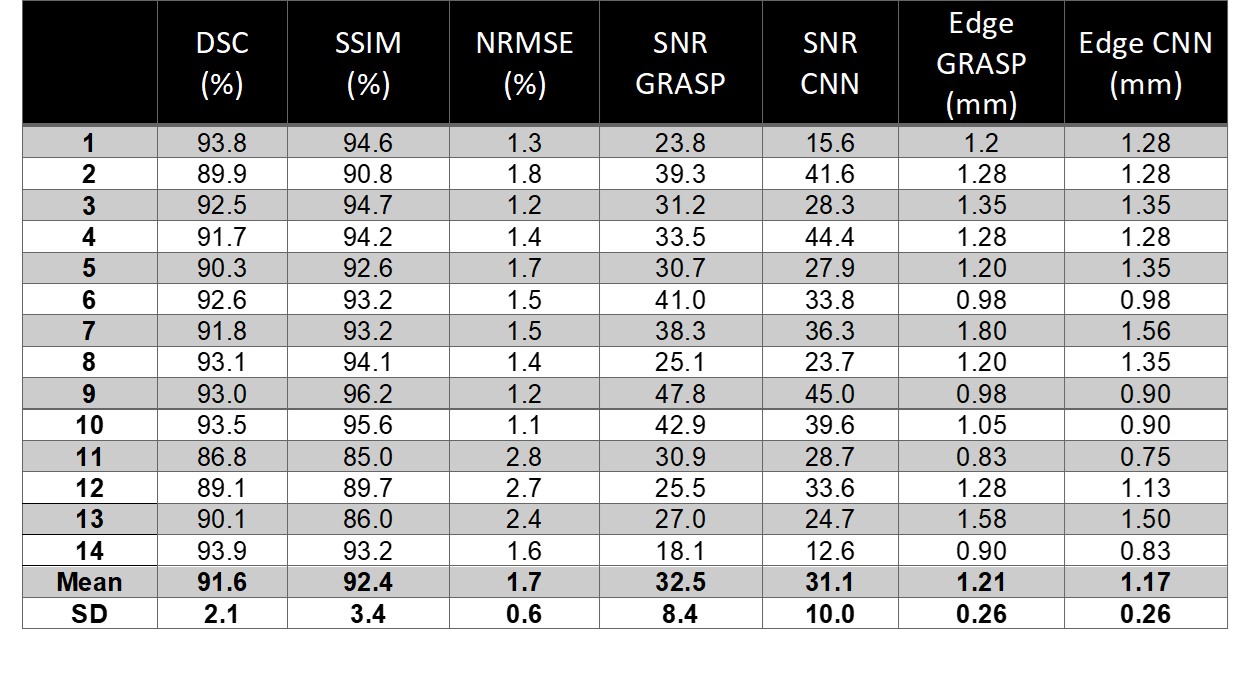
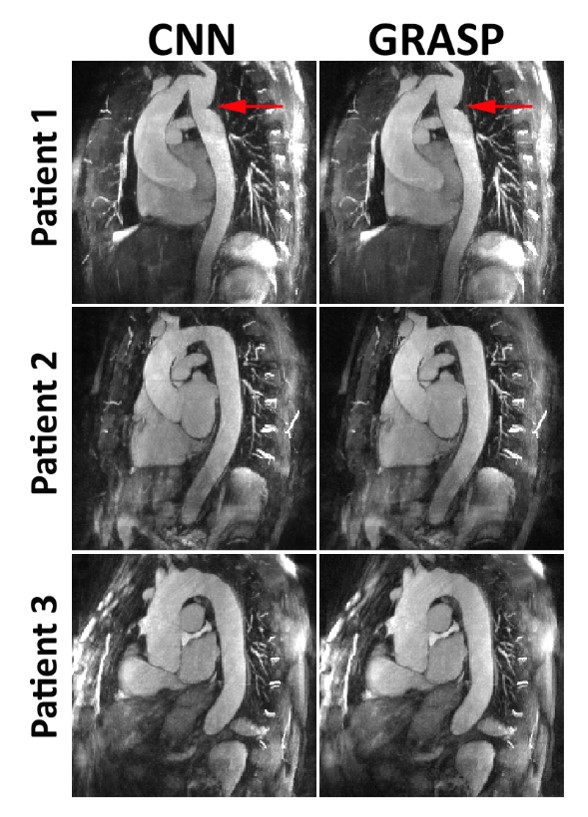
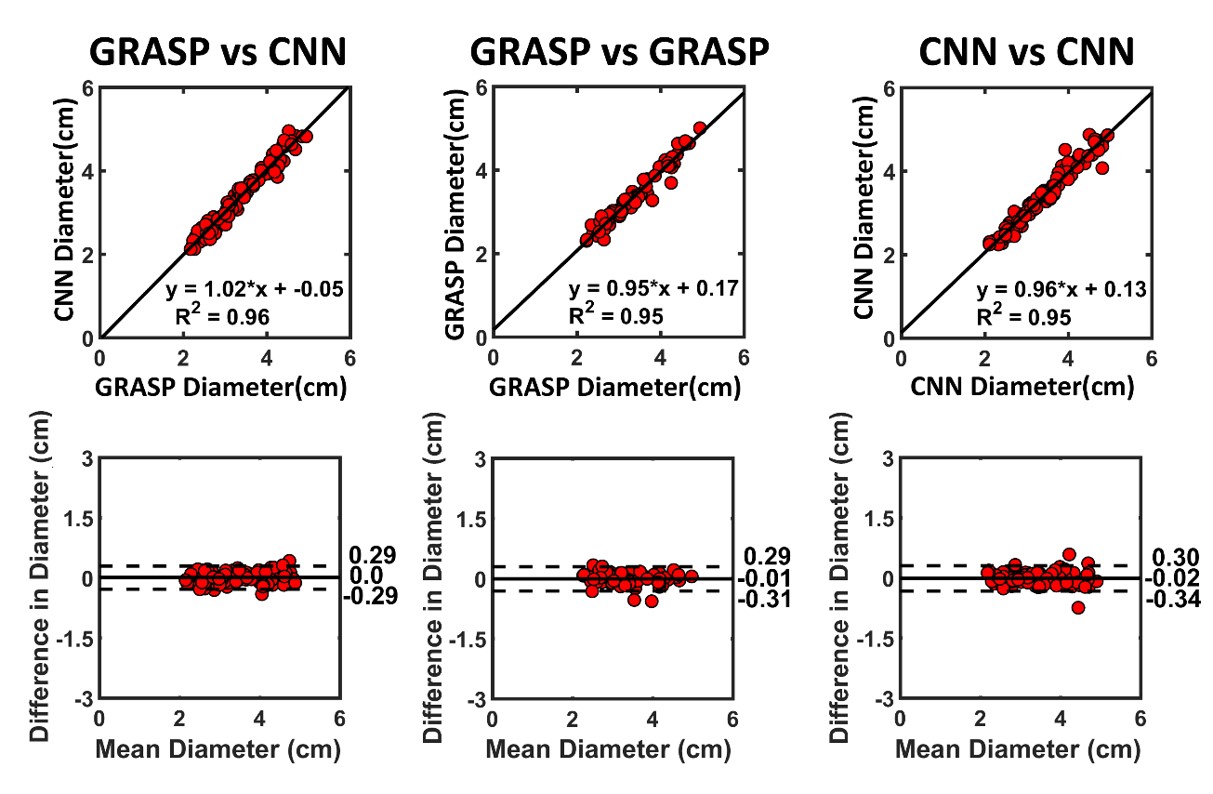
The mean reconstruction time, excluding the pre-processing step, for CNN (74 s) was 99% shorter (P < 0.001) than GRASP (12,703 s). Figure 3 shows representative thin reformatted MIPs of three patients. As shown, patient 1 exhibited coarctation which is clearly delineated in both GRASP and CNN (red arrow). As summarized in Table 1, compared with GRASP, CNN produced high data fidelity (DSC=91.6 ± 2.0%; SSIM=92.4 ± 3.4%, NRMSE=1.7±0.5%). Other metrics such as SNR (32.5 ± 8.4 for GRASP vs.31.2 ± 10.0 for CNN) and edge sharpness (1.21 ± 0.26 mm for GRASP vs.1.17 ± 0.26 mm for CNN) were not significantly different (P > 0.28). As shown in Figure 4, the vessel diameters were not significantly different (P>0.32), and they were strongly correlated (R2>0.95) and in good agreement (mean difference 0.0 cm; coefficient of repeatability=0.29 cm). These statistics indicate that intra-observer variability is similar to inter-reconstruction variabilityConclusion
This study shows that the proposed CNN reconstructs 3D thoracic NC-MRA images with high fidelity at 99% shorter time than GRASP. Future work includes a study to integrate our CNN into a vendor’s image reconstruction pipeline and achieve in-line image reconstruction.Acknowledgements
This work was supported in part by the following grants:NIH R01HL116895, R01HL138578, R21EB024315, R21AG055954References
1. Wheaton AJ, Miyazaki M. Non-contrast enhanced MR angiography: physical principles. J Magn Reson Imaging 2012;36(2):286-304.
2. Miyazaki M, Lee VS. Nonenhanced MR angiography. Radiology 2008;248(1):20-43.
3. Srichai MB, Kim S, Axel L, Babb J, Hecht EM. Non-gadolinium-enhanced 3-dimensional magnetic resonance angiography for the evaluation of thoracic aortic disease: a preliminary experience. Tex Heart Inst J 2010;37(1):58-65.
4. Francois CJ, Tuite D, Deshpande V, Jerecic R, Weale P, Carr JC. Unenhanced MR angiography of the thoracic aorta: initial clinical evaluation. AJR Am J Roentgenol 2008;190(4):902-906.
5. Amano Y, Takahama K, Kumita S. Non-contrast-enhanced MR angiography of the thoracic aorta using cardiac and navigator-gated magnetization-prepared three-dimensional steady-state free precession. J Magn Reson Imaging 2008;27(3):504-509.
6. Feng L, Grimm R, Block KT, Chandarana H, Kim S, Xu J, Axel L, Sodickson DK, Otazo R. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med 2014;72(3):707-717.
7. Haji-Valizadeh H, Collins JD, Aouad PJ, Serhal AM, Lindley MD, Pang J, Naresh NK, Carr JC, Kim D. Accelerated, free-breathing, noncontrast, electrocardiograph-triggered, thoracic MR angiography with stack-of-stars k-space sampling and GRASP reconstruction. Magnetic Resonance in Medicine;0(0). 8. Sahiner B, Chan HP, Petrick N, Wei D, Helvie MA, Adler DD, Goodsitt MM. Classification of mass and normal breast tissue: a convolution neural network classifier with spatial domain and texture images. IEEE Trans Med Imaging 1996;15(5):598-610.
9. Hammernik K, Klatzer T, Kobler E, Recht MP, Sodickson DK, Pock T, Knoll F. Learning a variational network for reconstruction of accelerated MRI data. Magn Reson Med 2018;79(6):3055-3071.
10. Yang G, Yu S, Dong H, Slabaugh G, Dragotti PL, Ye X, Liu F, Arridge S, Keegan J, Guo Y, Firmin D, Keegan J, Slabaugh G, Arridge S, Ye X, Guo Y, Yu S, Liu F, Firmin D, Dragotti PL, Yang G, Dong H. DAGAN: Deep De-Aliasing Generative Adversarial Networks for Fast Compressed Sensing MRI Reconstruction. IEEE Trans Med Imaging 2018;37(6):1310-1321.
11. Schlemper J, Caballero J, Hajnal JV, Price AN, Rueckert D. A Deep Cascade of Convolutional Neural Networks for Dynamic MR Image Reconstruction. IEEE Trans Med Imaging 2018;37(2):491-503. 12. Chaudhari AS, Fang Z, Kogan F, Wood J, Stevens KJ, Gibbons EK, Lee JH, Gold GE, Hargreaves BA. Super-resolution musculoskeletal MRI using deep learning. Magn Reson Med 2018;80(5):2139-2154.
13. Knoll F, Schwarzl A, Diwoky C, Sodickson DK. gpuNUFFT - An Open Source GPU Library for 3D Regridding with Direct MATLAB Interface. 2014; Melbourne, Australia. p No. 4297.
14. Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE, Jr., Eagle KA, Hermann LK, Isselbacher EM, Kazerooni EA, Kouchoukos NT, Lytle BW, Milewicz DM, Reich DL, Sen S, Shinn JA, Svensson LG, Williams DM, American College of Cardiology Foundation/American Heart Association Task Force on Practice G, American Association for Thoracic S, American College of R, American Stroke A, Society of Cardiovascular A, Society for Cardiovascular A, Interventions, Society of Interventional R, Society of Thoracic S, Society for Vascular M. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010;121(13):e266-369.
Figures