0644
Magnetic Resonance Fingerprinting of the Normal Pancreas1Radiology, University of Cambridge, Cambridge, United Kingdom, 2Cambridge University Hospitals NHS Foundation Trust, Cambridge, United Kingdom, 3Cancer Research UK, Cambridge, United Kingdom, 4IMAGO7 Foundation, Pisa, Italy, 5GE Healthcare, Munich, Germany, 6Radiology, Cambridge University Hospitals NHS Foundation Trust, Cambridge, United Kingdom, 7University of Cambridge, Cambridge University Hospitals NHS Foundation Trust, Cambridge, United Kingdom
Synopsis
MR imaging of the pancreas is challenging due to its retroperitoneal deep-sited location in the abdomen. In addition to its position, the pancreas is subject to breathing motion artifact, which limits the clinical value of pancreatic MRI. Patients with pancreatic cancer are usually very frail, which limits their tolerance to long examinations or breath-hold MRI measurements. MR Fingerprinting (MRF) is an innovative measurement technique that provides qualitative data and quantitative parameter maps from a single acquisition with the potential to reduce exam times. MRF is technically challenging due to limitations in processing capabilities, which we assess in this work.
Introduction
MR imaging of the pancreas is challenging due to its retroperitoneal deep-sited location in the abdomen. In addition to its position, the pancreas is subject to breathing motion artifact, which limits the clinical value of pancreatic MRI. Patients with pancreatic cancer are usually very frail, which limits their tolerance to long examinations or breath-hold MRI measurements. In most clinical centres, MRIprotocols remain mostly qualitative and subjective based on “MR signal intensity”. Quantitative sequences are rarely performed in clinical settings, because quantitation has previously been limited to single parametric measurements with significant scan time requirements and sensitivity to system imperfections and patient motion.
MR Fingerprinting (MRF) is an innovative measurement technique that provides qualitative data and quantitative parameter maps from a single acquisition, which has the potential to reduce clinical exam times. MRF is a method that promises to enable fast, sensitive, repeatable, and quantitative T1 and T2 mapping by exploiting transient signals caused by the variation of pseudorandom sequence parameters. MRF has several advantages that could benefit pancreatic studies. This work investigates the utility of MRF for pancreatic imaging in the presence of free-breathing motion.
Methods
Twelve healthy-volunteers were imaged with free-breathing MRF on a 3.0 T MRI system (MR750 GE Healthcare, Waukesha, WI, USA) using a 32-channel receive-only abdominal array. Imaging occurred with local ethical approval. The MRF acquisition consisted of 2D steady-state-free-precession (SSFP) acquisitions (1, 2), with 979 frames using undersampled spirals interleaved by the golden-angle. Imaging parameters were: field-of-view=260x260mm2, matrix=256x256, slices=15-22, slice thickness=3.0mm, spacing 1.0mm, sampling bandwidth=±250kHz, slice dephasing=8π, echo time=2.5ms, acquisition time=13seconds/slice, total scan time=3-5minutes, with repetition time and flip angle lists matching the values in Jiang (1). Sagittal and axial imaging directions were acquired. Maximum gradient strength per spiral was 28mT/m and maximum slew rate 108T/m/s. T1 and T2 maps from MRF were obtained by inner product pattern matching of signal look-up table based on T1 and T2 simulations with the acquired reconstructed data. Qualitative T1 or T2 weighted images were acquired by using the generated maps. The MRF dictionary was computed for T1 and T2 using extended phase graphs formalism and included the slice profile. The dictionary was simulated for T1=[0.01:0.005:1;1:0.04:6] seconds, and for T2=[0.005:0.001:0.1;0.1:0.01:1;1:0.01:4;4:0.04:6]seconds.Results
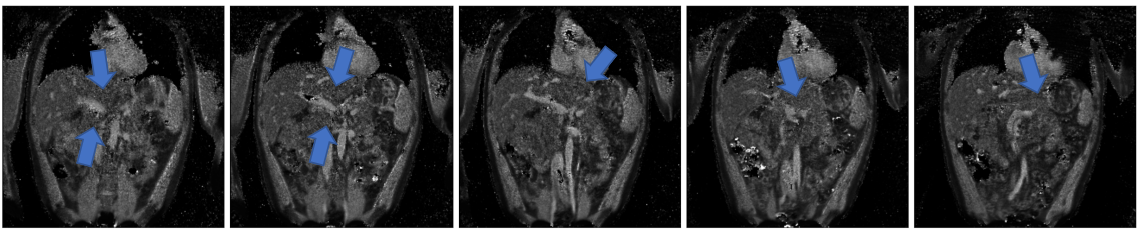
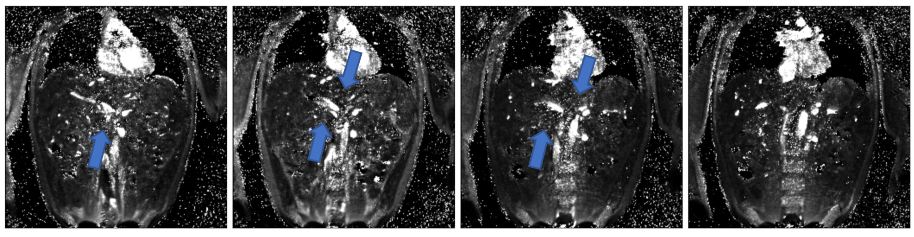
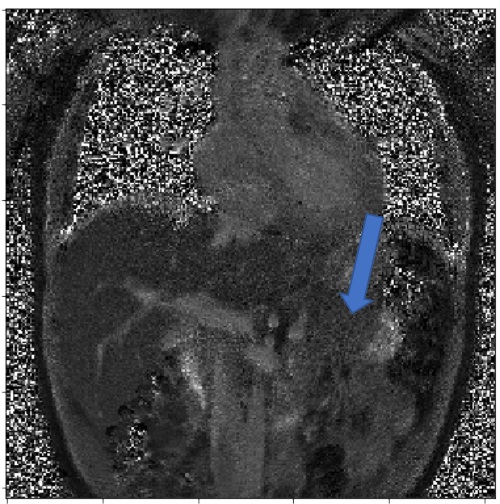
Qualitative T1WI and T2WI images, and standard T1(variable flip angle) and T2maps were obtained for each individual. A representative T1 and T2map generated from MRF is shown in Figures1-3. The reconstruction time was however significant. Dictionary simulation normally only need be performed once for a specific flip angle / TR list. The reconstruction of each channel, slice, and frame prior to data compression in combined coil and SVD space required an hour. Dictionary matching occurred within several minutes after the frames were in image space.Discussion
This study demonstrated the feasibility of MRF in the pancreas. The total acquisition time was reduced compared with institutional pancreatic protocol. With the MRF framework, T1 and T2 mapping were also acquired besides qualitative data. The maps appeared insensitive to motion, although some slices displayed either a hyper or hypointensity that was not visible on other slices, which is explainable by imperfect matching of the dictionary due to motion. The T1 maps appeared relatively similar throughout all image sets. The T2 maps had more visible artefact, such as gradient sampling pattern artefacts visible on the maps, or T2 underestimation, likely resulting from field inhomogeneities such as susceptibility mismatch caused by air inside the gut. This work was challenging due to computational limitations involving the high dimensionality of the acquired and simulated datasets. The 979 temporal frame was reconstructed with 32 coil channels and ~20 slices at the given matrix size of 256x256, which required memory reduction via coil combination and SVD compression before data matching. During dictionary matching where the inner product was calculated between the simulated dictionary and compressed acquisition data, the maximum amount of RAM used was 350 gigabytes while using 44 threads (Xeon Gold 6152). When higher reconstruction matrices or multiple simulated B1+ or B0 values were used, inner product matching would fail within Matlab due to memory errors. These memory issues are specific to the high number of channels used in abdominal arrays, when combined with the large amount of data generated multi-slice, free-breathing MRF.Conclusion
This work demonstrates fast quantitative T1 and T2 mapping of the pancreas. The potential benefit of MRF is that it could result in fast, accurate, quantitative measurements to improve disease detection.Acknowledgements
This work has been supported by funding from Cancer Research UK, GlaxoSmithKline, the National Institute of Health Research (NIHR) Cambridge Biomedical Research Centre and Addenbrooke’s Charitable Trust.References
1. Jiang Y, Ma D, Seiberlich N, Gulani V, Griswold MA. MR fingerprinting using fast imaging with steady state precession (FISP) with spiral readout. Magnetic Resonance in Medicine. 2015;74(6):1621-31.
2. Ma D, Gulani V, Seiberlich N, Liu K, Sunshine JL, Duerk JL, et al. Magnetic resonance fingerprinting. Nature. 2013;495(7440):187-92.
Figures