0642
Can two breath-hold 3D-MRCP replace the conventional 3D-MRCP?1Department of Radiology, Peking Union Medical College Hospital, Beijing, China, 2Philips Healthcare, Beijing, China, 3Cancer Research UK Cambridge Institute, University of Cambridge, Cambridge, United Kingdom
Synopsis
This study was to evaluate and compare the image quality and diagnostic performance of three MRCP protocols, including BH-3D-CS-MRCP, Gradient Spin Echo (BH-GraSE-3D-MRCP) and navigator-triggered (NT) MRCP.
Introduction
Conventional navigator-trigger(NT)3D MRCP routinely requires 3–6 minutes of acquisition time, leading to diaphragmatic drift and suboptimal imaging quality as a consequence [1]. Several approaches have been reported to shorten the scan time and achieve the 3D-MRCP with a single breath-hold, including 3D gradient and spin-echo (GRASE) technique [2] and compressed-sensing (CS) [3]. Two previous study have reported that the imaging quality of BH- GraSE-MRCP were comparable or even superior to that of the conventional 3D-NT-MRCP [4, 5]. However, these studies did not compare GraSE-MRCP with other BH-3D-MRCP, like CS-BH-MRCP and did not focus on any specific disease. This study was to evaluate and compare the image quality and diagnostic performance of three MRCP protocols on pancreas cyst, including BH-3D-CS-MRCP, Gradient Spin Echo (BH-GraSE-3D-MRCP) and navigator-triggered (NT) MRCP.Method and Materials
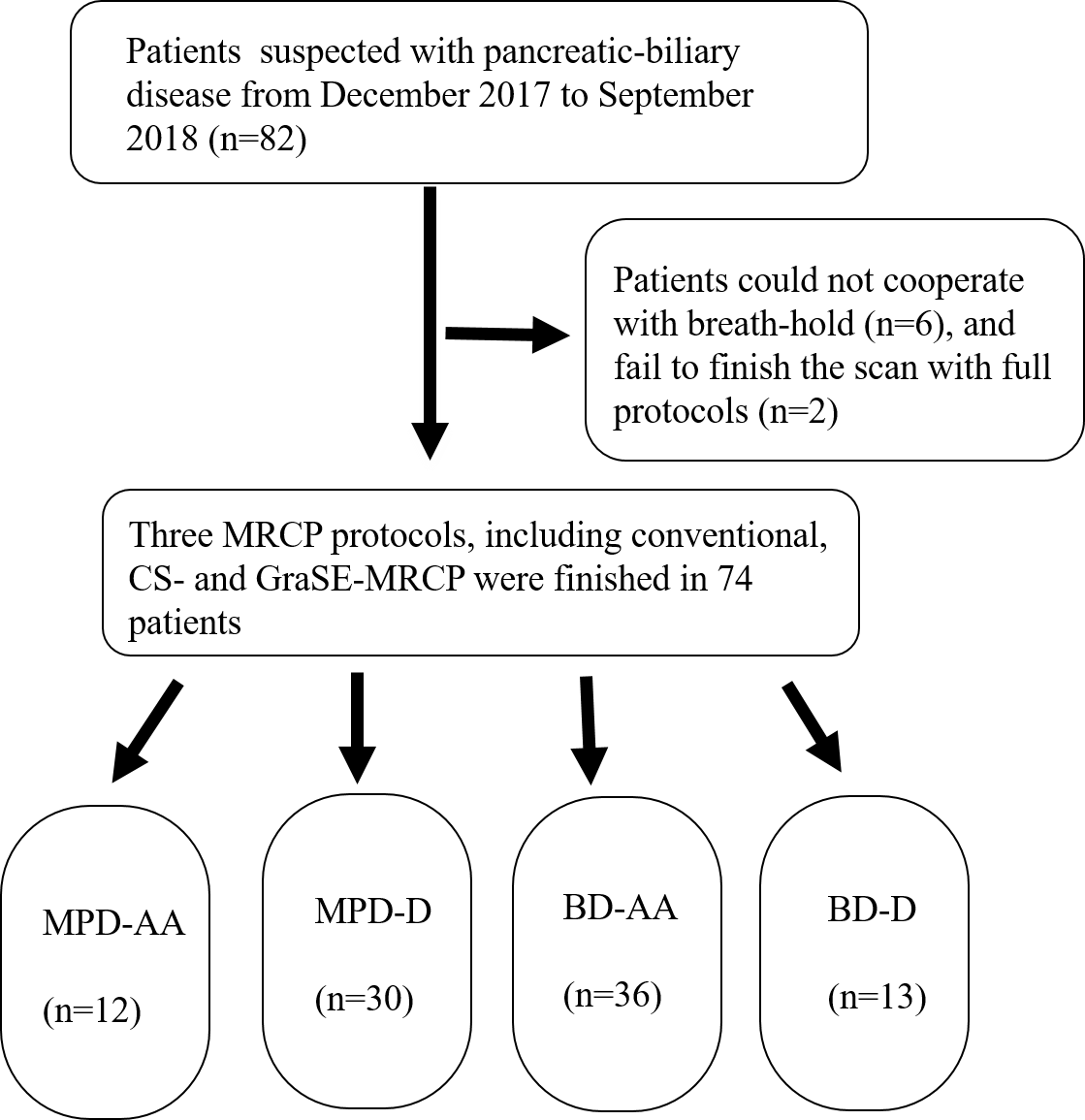
The study design was summarized in Figure 1. Seventy-four (mean age 45.1 years, age range 13-78 years, 32 females and 42 male) patients suspected with duct-related pathologies were prospectively enrolled. All the patients went through the three MRCP protocols in a random order. The acquisition time of each protocol was recorded. The imaging assessment was based on a 5-point scale by 2 radiologists independently, which included the following four parts: overall imaging quality, background suppression, artifacts, and the duct visualization. For duct visualization, the entire pancreaticobiliary system was divided into the 12 segments: the common bile and hepatic ducts as an integral segment (CBD+CHD), the cystic duct (CD), the gallbladder (GB), the right hepatic duct (RHD), the anterior branch of the right hepatic duct (RHD-AB), the posterior branch of the right hepatic duct (RHD-PB), the left hepatic duct (LHD), the medial branch of the left hepatic duct (LHD-MB), the lateral branch of the left hepatic duct (LHD-LB), and the proximal / middle / distal parts of the main pancreatic duct (P-MPD, M-MPD, and D-MPD respectively). The Friedman test was used to compare the imaging quality (IQ) scores and the scan time among conventional NT, BH-GraSE, and BH-CS MRCP followed by post hoc analysis. The duct-related disease was divided into four groups: main pancreatic duct related anatomy abnormality (MPD-AA), main pancreatic duct related disease (MPD-D), bile duct related anatomy abnormality (BD-AA), and bile duct related disease (BD-D). The diagnosis performance of the three protocols were evaluated using the AUC value and compared against each other using McNemar’s test. The inter-observer agreement was evaluated by linearly weighted kappa coefficients.Results
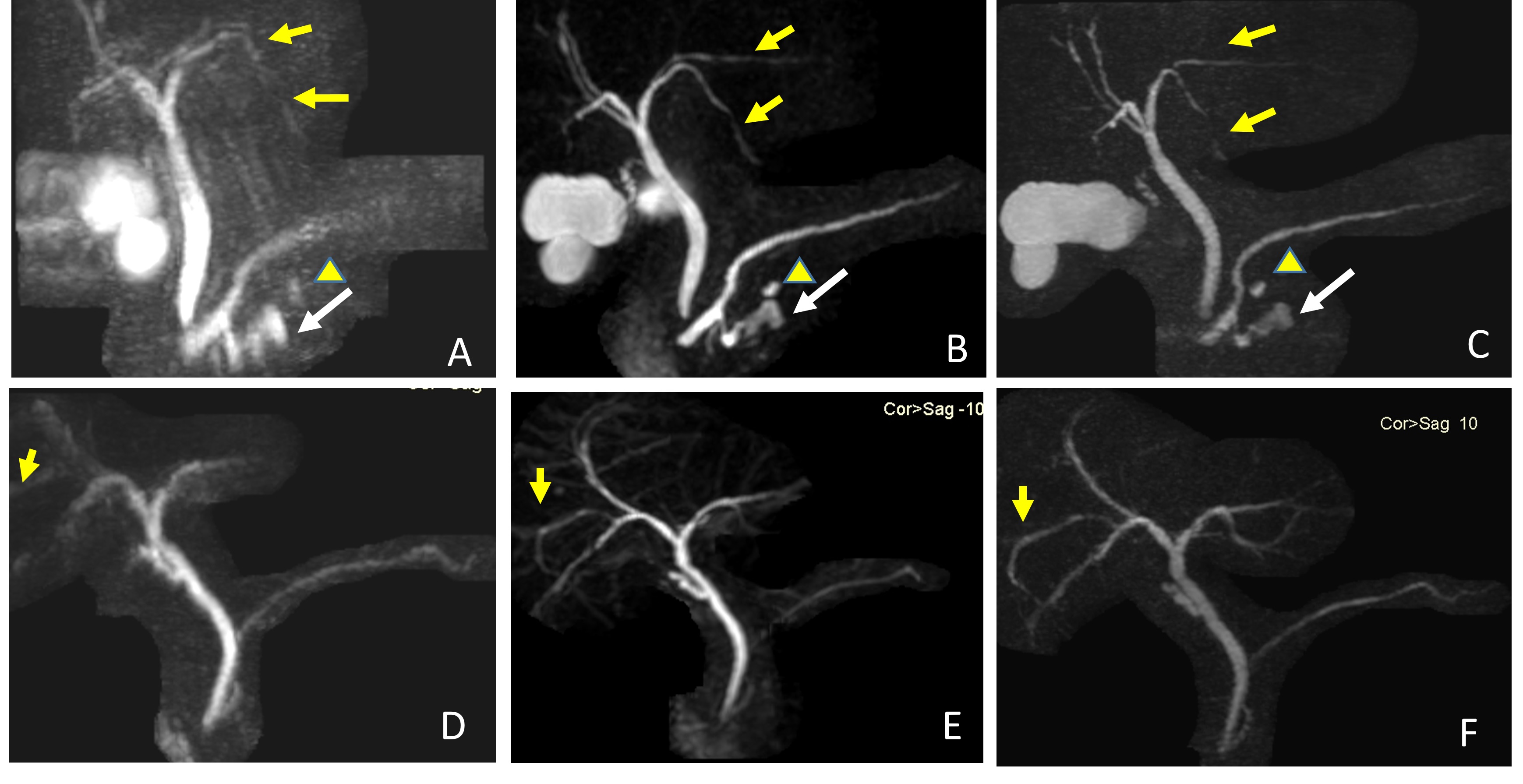
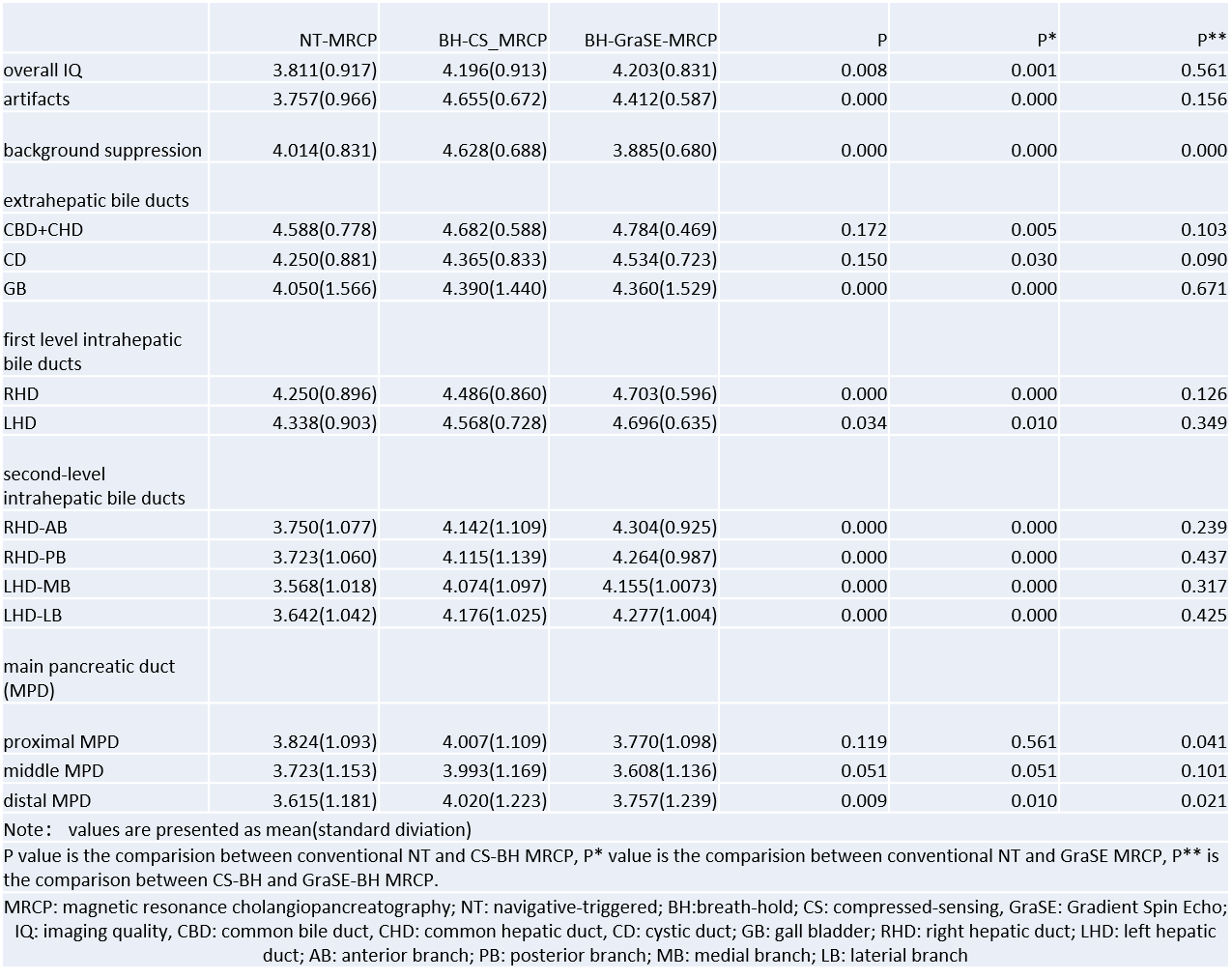
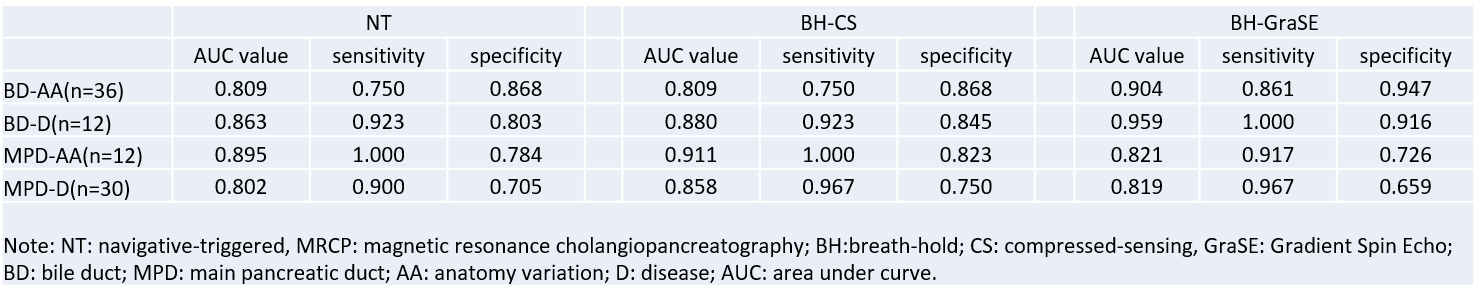
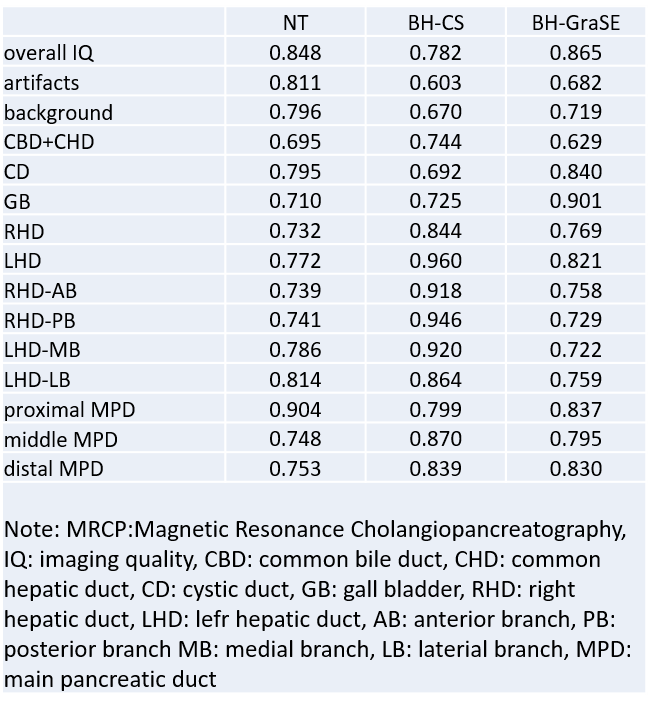
The acquisition time was 17-19, 16-18, and 283-325 seconds for CS-BH-3D-MRCP, GraSE-3D-BH-MRCP, and conventional 3D-MRCP protocols, respectively. The overall imaging quality of 3D BH-GRASE-MRCP and 3D BH-CS-MRCP (Figure 2) were significantly better than that of 3D conventional MRCP , as shown in Figure 3. There was no significant difference in both scan time and imaging quality (both P﹥0.05) between CS-BH-3D-MRCP and GraSE-3D-BH-MRCP except for the background suppressing and MPD. The number of positive cases was 12 for MPD-AA, 30 for MPD-D, 36 for BD-AA, and 13 for BD-D. As shown in Figure 4, the diagnostic performance of both CS-MRCP (AUC=0.911) and NT-MRCP (AUC=0.895) for MPD-AA were significantly better than that of the GraSE-MRCP (AUC=0.821). The AUC of MPD-D was 0.802 with NT-MRCP, 0.858 with CS-MRCP, and 0.819 with GraSE-MRCP, and there was no significant difference among them (all P﹥0.05). For both BD-D and BD-AA, the diagnosis performance of GraSE MRCP (AUC=0.959 and 0.904) was statistically better than those of the NT-MRCP (AUC=0.863 and 0.809) and CS-MRCP (0.880 and 0.809). The overall diagnosis performance of the combination of CS-MRCP and GraSE-MRCP (AUC=0.935) was significant better than that of the NT-MRCP (AUC=0.826), the P value in less than 0.05. All the subjective evaluation reached good to excellent level of agreement ranging from 0.603 to 0.960 (Figure 5).Discussion
The scan time of these two BH-MRCP was significantly decreased compared to conventional MRCP. For main pancreatic duct visualization and characterization, the CS-MRCP is superior to GraSE-MRCP and comparable to conventional NT-MRCP. However, the GraSE-MRCP performed better in visualization the bile duct pathologies than CS-MRCP. What’s more, when combine these two breath-hold 3D-MRCP, the diagnosis performance was significantly better than that with the conventional NT-MRCP. These findings are expected to help improve the workflow for patients suspected with duct-related pathologies. The acquisition of conventional NT-MRCP was shown non-optimal for patients with sufficient breath-hold capacity, suggesting the potential of imaging time reduction without pampering the diagnostic capability.Conclusion
Compared to NT-MRCP, CS-BH-3D-MRCP and GraSE-3D-BH-MRCP can provide better image quality for pancreas disease, while reducing the scan time significantly. When combine these two breath-hold 3D-MRCP, the diagnosis performance was significantly better than that with the NT-MRCP.Acknowledgements
No acknowledgement found.References
1. Anupindi SA, Victoria T. Magnetic resonance cholangiopancreatography: techniques and applications. Magn Reson Imaging Clin N Am. 2008;16(3):453-66
2. Wielopolski PA, Gaa J, Wielopolski DR, Oudkerk M. Breath-hold MR cholangiopancreatography with three-dimensional, segmented, echo-planar imaging and volume rendering. Radiology. 1999;210(1):247-52. 3. Chandarana H, Doshi AM, Shanbhogue A, et al. Three-dimensional MR Cholangiopancreatography in a Breath Hold with Sparsity-based Reconstruction of Highly Undersampled Data. Radiology. 2016;280(2):585-94.
4. Nam JG, Lee JM, Kang HJ, et al. GRASE Revisited: breath-hold three-dimensional (3D) magnetic resonance cholangiopancreatography using a Gradient and Spin Echo (GRASE) technique at 3T. Eur Radiol. 2018;28(9):3721-8.
5. Yoshida M, Nakaura T, Inoue T, et al. Magnetic resonance cholangiopancreatography with GRASE sequence at 3.0T: does it improve image quality and acquisition time as compared with 3D TSE? Eur Radiol. 2018;28(6):2436-43.
Figures