0641
Evaluation of the clinical usefulness of 3-dimensional Magnetic Resonance Cholangiopancreatography with compressed sensing in patients with pancreatobiliary disease1Magnetic Resonance Imaging, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 2MR Collaborations, Siemens Healthcare, Beijing, China, 3Siemens Healthcare Gmbh, Erlangen, Germany, 4Hepatobiliary and Pancreatic Surgery, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China
Synopsis
This study aimed to compare the acquisition time, image quality, and diagnostic performance of three three-dimensional (3D) magnetic resonance cholangiopancreatography (MRCP) with compressed-sensing (CS) prototype protocols with those of conventional MRCP in a large cohort of patients with suspected pancreaticobiliary disorders, and to explore the effect of the in-plane phase-encoding direction on the image quality of small-field-of-view (FOV) breath-hold (BH) CS-MRCP (sFOV-BH-CS-MRCP). We found that CS-MRCP provides comparable image quality and diagnostic performance with significantly shortened scan time, and sFOV-BH-CS-MRCP should be acquired in the head-feet phase-encoding direction instead of the left-right direction.
Introduction
Three-dimensional (3D) magnetic resonance cholangiopancreatography (MRCP) is an effective imaging method to evaluate pancreatobiliary disorders. However, respiratory-triggered 3D MRCP routinely requires 3 - 6 minutes of acquisition time and may result in suboptimal image quality in patients with shallow or irregular respiratory rhythm. Many acceleration techniques are currently available, including compressed sensing (CS) [1], which allows image reconstruction from under-sampled data using a non-linear algorithm. CS-MRCP can be acquired with navigator-triggered (NT),breath-hold in a regular field-of-view (rFOV-BH), and breath-hold in a small field-of-view (sFOV-BH). The purpose of this study was to compare the image quality and diagnostic performance of three prototypic CS-MRCP protocols with conventional MRCP (c-MRCP), in a large cohort of clinical patients with suspected pancreatobiliary diseases.Methods
A total of 128 consecutive patients were prospectively recruited (58 male and 70 female; mean age, 54.5 ± 15.4 years). All the patients underwent four 3D MRCP protocols in random order on a 3T MR system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany), including NT-CS-MRCP (380×380 mm2, resolution 0.5×0.5×1.0 mm3), rFOV-BH-CS-MRCP (380×380 mm2, resolution 0.5×0.5×1.1 mm3), sFOV-BH-CS-H/F-MRCP in a head-feet in-plane phase-encoding direction (250×250 mm2, resolution 0.5×0.5×1.1 mm3), and c-MRCP (380×380 mm2, resolution 0.5×0.5×1.1 mm3). In addition, 34 of the 128 patients with good breath-holding capability (≥18s) underwent the above small-field-of-view protocol modified to a left-right phase-encoding direction (sFOV-BH-CS-L/R-MRCP). All the CS-MRCP protocols were modified based on a prototype sequence. The acquisition time was documented for each examination. Two radiologists independently evaluated the images blindly on a 5-point scale for the following parameters: image quality or sharpness, visibility of biliary and pancreatic ducts, background suppression, diagnostic confidence with duct anatomic variations, and pancreaticobiliary disease. The Friedman test with post-hoc analysis and Wilcoxon signed-rank test were performed on these assessments. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of each protocol were calculated. Intraclass correlation coefficients (ICC) were obtained to assess reader agreement on each qualitative analysis item.Results
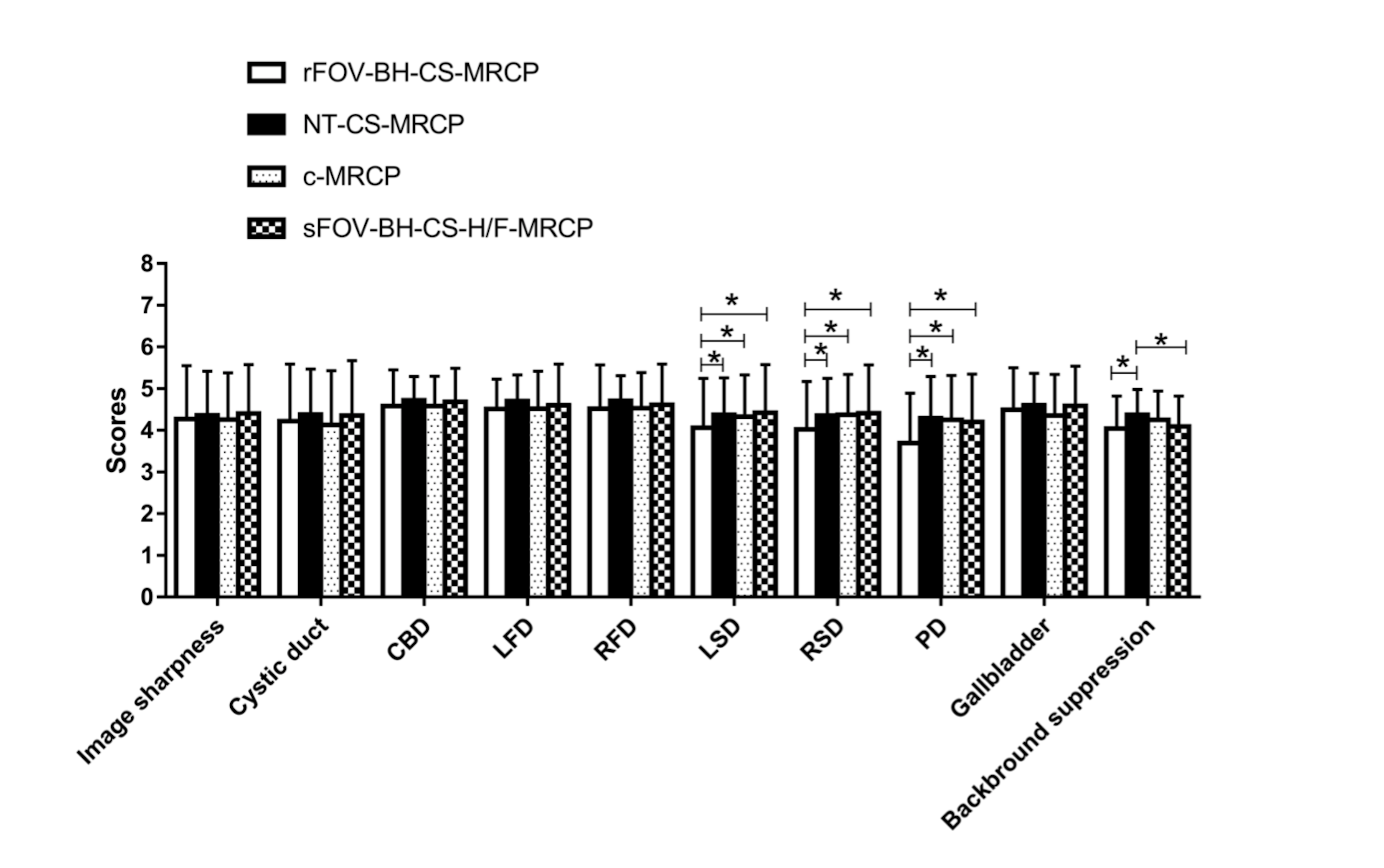
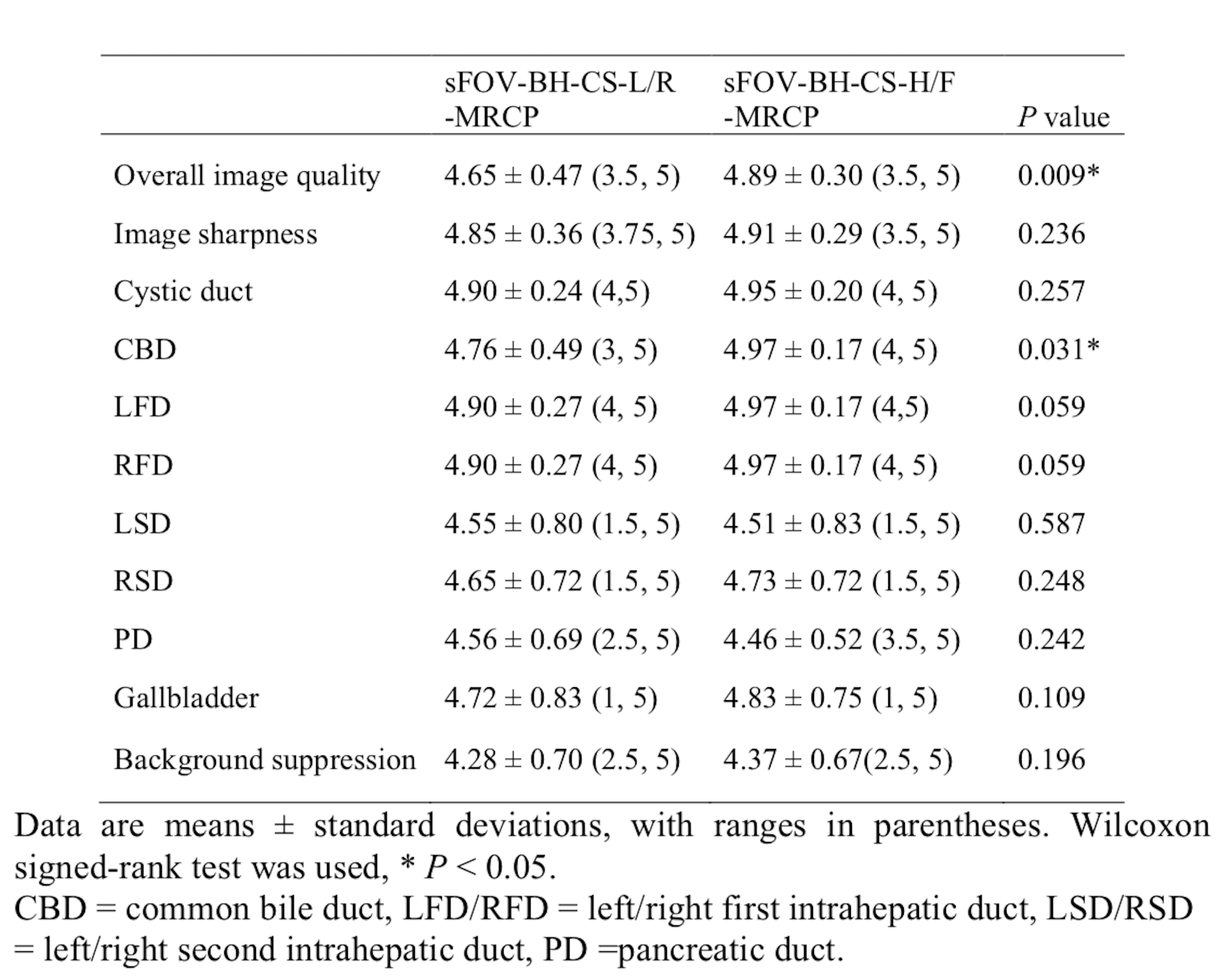
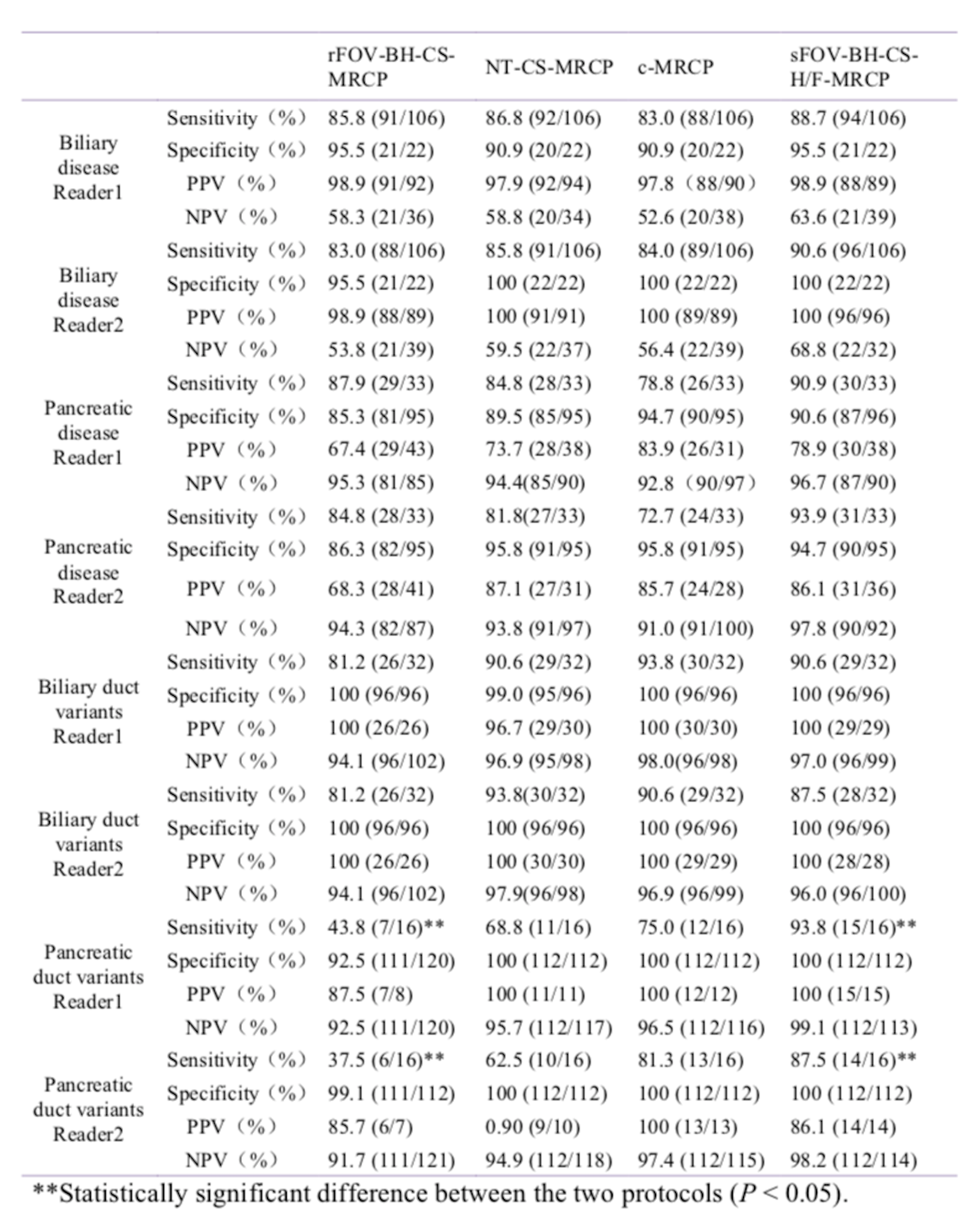
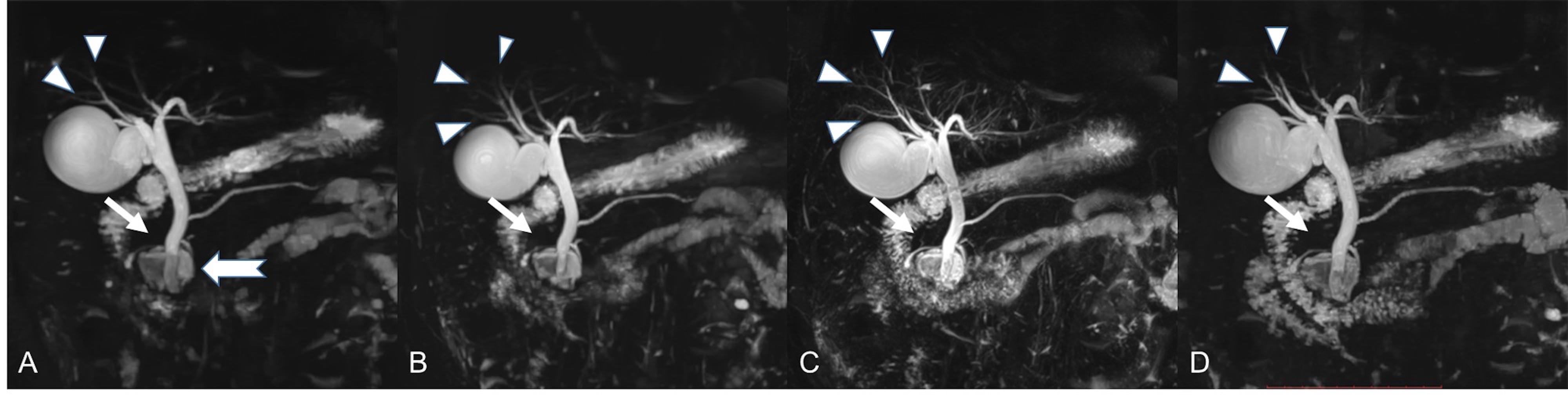
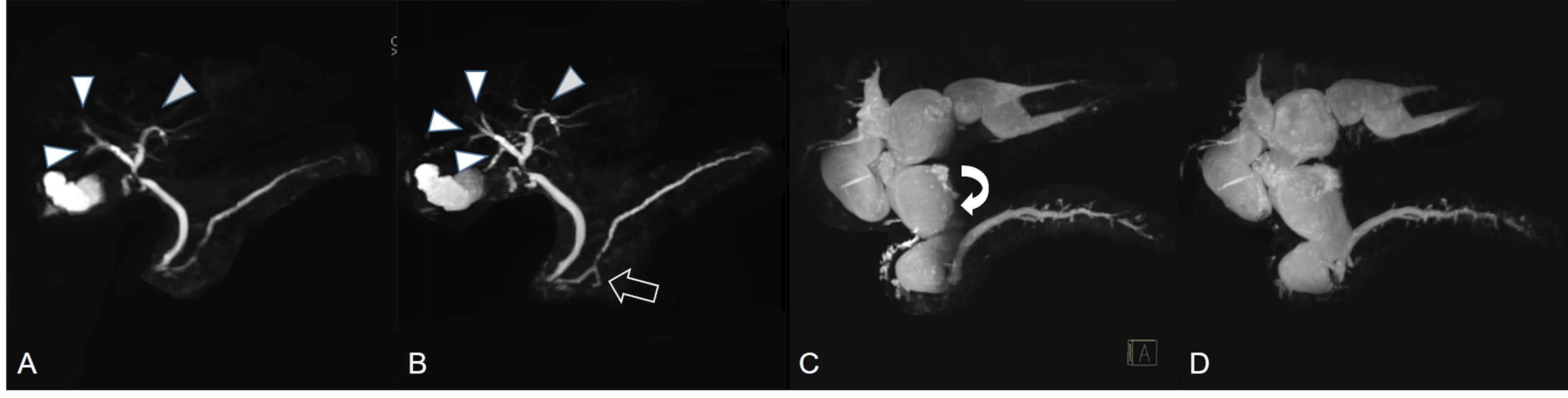
The mean acquisition times of c-MRCP, NT-CS-MRCP, and BH-CS-MRCP were 432 seconds, 207 seconds, and 17 seconds, respectively (all P< 0.001). The ICCs were fair to excellent for all items. Of the 128 patients who underwent the four sequences, the visualization of extrahepatic bile ducts and first-level intrahepatic bile ducts was generally good (all P> 0.05), whereas that of the second-level intrahepatic bile ducts (ISD) and pancreatic duct (PD) with rFOV-BH-CS-MRCP was lower than that of the other three protocols (P < 0.05 for each comparison). Background suppression was similar with BH-CS -MRCP, both of which were inferior to NT-CS-MRCP (both P< 0.05) (Figure 1). There were no significant differences among the four sequences for each reader when detecting bile duct variants and pancreaticobiliary disease (Table 2), whereas the sensitivity of sFOV-BH-CS-H/F-MRCP for each reader was significantly higher than that of rFOV-BH-CS-MRCP (P < 0.05) for detecting pancreatic duct variants. Of the 34 patients who also underwent sFOV-BH-CS-L/R-MRCP (Table 1), the overall image quality and visualization of the common bile duct (CBD) (Figure 2) with the protocol were inferior to those with sFOV-BH-CS-H/F-MRCP (both P < 0.05). In addition to respiratory artifacts occurring at other sequences, sFOV-BH-CS-MRCP was also prone to aliasing artifacts. A total of 6.2% (8/128) patients with sFOV-BH-CS-H/F-MRCP and 11.8% (4/34) with sFOV-BH-CS-L/R-MRCP were confronted with unresolved aliasing artifacts and significant degradation of image quality and duct structure appreciation (Figure 3).Discussion
We investigated all the proposed CS-MRCP methods by comparing with c-MRCP initially, and we found that CS-MRCP provided comparable image quality to c-MRCP with dramatically shortened acquisition time, except when revealing a fine pancreaticobiliary duct with rFOV-BH-CS-MRCP. However, this limitation could be improved by sFOV-BH-CS-MRCP. These findings were consistent with previous findings [2-3]. For the diagnostic performance of each protocol,our results were slightly different from those of a previous study [3], and we speculate that this might be due to the small number of cases with pancreatic disease in our study and the differences in disease types. Furthermore, we found that the overall image quality and visualization of CBD with sFOV-BH-CS-H/F-MRCP were better than those with sFOV-BH-CS-L/R-MRCP, which was recommended in this previous study [3]. Based on our observation, aliasing artifacts with the latter protocol usually folded into the CBD area and directly caused the suboptimal image quality.Conclusion
CS-MRCP provides comparable image quality to c-MRCP with significantly shortened acquisition time. Visualization of the small ductal structures could be improved by sFOV-BH-CS-MRCP compared with rFOV-BH-CS-MRCP, and using the head-feet phase-encoding direction instead of the left-right direction could reduce the degradation of image quality caused by unresolved aliasing artifacts.Acknowledgements
No acknowledgement found.References
1. Runge VM, Richter JK, Heverhagen JT. Speed in clinical magnetic resonance. Invest Radiol 2017; 52:1-17.
2.Yoon JH, Yu MH, Chang W, et al. Clinical feasibility of free-breathing dynamic T1-weighted imaging with gadoxetic acid-enhanced liver magnetic resonance imaging using a combination of variable density sampling and compressed sensing. Invest Radiol 2017; 52:596-604.
3. Zhu L, Wu X, Sun Z, et al. Compressed-sensing accelerated 3-dimensional magnetic resonance cholangiopancreatography: application in suspected pancreatic diseases. Invest Radiol 2018; 53:150-157.
Figures