0640
Precise stiffness-based detection of pancreatic carcinoma by tomoelastography1Radiology, Charite - University Hospital Berlin, Berlin, Germany, 2Surgery, Charite - University Hospital Berlin, Berlin, Germany, 3Informatics, Charite - University Hospital Berlin, Berlin, Germany
Synopsis
Pancreatic stiffness was investigated using multifrequency MR elastography (MRE) and tomoelastography data processing in healthy controls (CTR) and patients with pancreatic ductal adenocarcinoma (PDAC). In healthy volunteers, tomoelastography was highly reproducible and showed no significant influences of region and age on pancreatic stiffness. Furthermore, we show that PDAC can be detected as stiff masses with full separation of MRE-values between CTR and PDAC. MRE-based tumor volume correlated excellently with CT-volumetry. Tomoelastography is well suited for boundary detection of pancreatic tumors within standardized, quantitative and contrast-agent free imaging examinations.
Introduction:
Pancreatic ductal adenocarcinoma (PDAC) is the most common form of pancreatic cancer with a rapid progression and poor 5-year survival rate 1. Detection for tumor boundaries based on precise stiffness-based definition could support therapy planning and treatment monitoring in PDAC. PDAC have been reported to be stiffer than normal-appearing pancreatic tissue 2,3 motivating the use of magnetic resonance elastography (MRE) 4 for PDAC boundary detection. Therefore, we test novel multifrequency MR elastography (MRE) and tomoelastography data processing 5 based on multiple pressurized-air drivers for its capability to precisely detect tumor boundaries.Methods:
In this prospective study 27 healthy subjects (CTR, subdivided, based on a cut-off of 50 years; HV-young, <50 years, n=14; HV-old, ≥50 years, n=13) and 14 patients with histologically proven PDAC, subdivided into non-tumorous (PDAC-NT) and tumorous (PDAC) regions) were investigated by multifrequency MRE and tomoelastography processing 5. All experiments were conducted on a 1.5 T MRI scanner equipped with a 12-channel phased array surface coil. Three-dimensional wave fields at four frequencies between 30 and 60Hz acquired under free breathing within 5 min were induced by four synchronized, pressurized-air driven actuators placed around the thorax (figure 1). Shear wave speed (SWS in m/s) as a surrogate of stiffness was measured in the pancreas' head, corpus and tail. A subgroup of 9 randomly chosen healthy volunteers were scanned twice, to assess the test-re-test variability using the intraclass correlation coefficient (ICC) and relative absolute difference (RAD). The diagnostic accuracy was calculated for detection of PDAC. SWS-based tumor volumes (V-MRE) were correlated with contrast-agent enhanced computed tomography (CT)-volumetry (V-CT).Results:
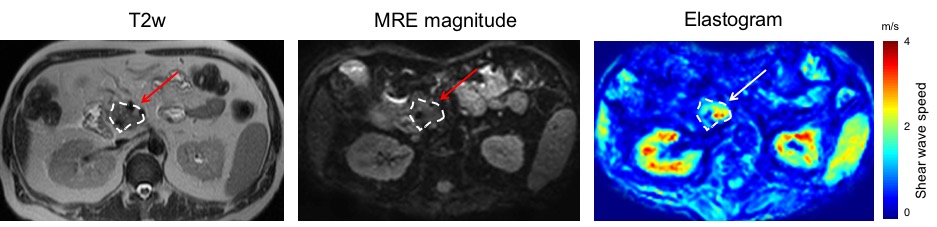
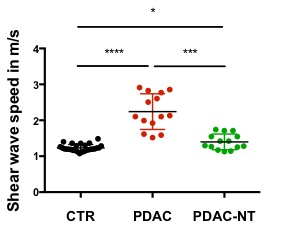
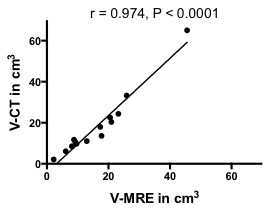
Figure 2 shows representative elastograms (wave speed maps) demonstrating a visual differentiation of PDAC with higher stiffness values. Repeated measurements of 9 healthy volunteers showed a high repeatability with an ICC of 0.79 and a RAD of 0.04. No significant influences of region (head, 1.23±0.12m/s; corpus, 1.23±0.11m/s; tail, 1.24±0.13m/s) and age (CTR-young, 1.22±0.07m/s vs CTR-old, 1.25±0.12m/s, p=0.45; age vs SWS, r=0.15, p=0.46) were discernable. PDAC (2.20±0.49 m/s; p<0.0001, figure 3) was stiffer than CTR, without any overlap between both groups, providing a cutoff of 1.5 m/s with a sensitivity and specificity of 100% and 100%, giving an AUROC of 1.0. Inner-patient analysis showed a higher stiffness in PDAC compared to PDAC-NT (1.40±0.22m/s; p=0.001, figure 3) and a cutoff of 1.6 m/s provides a sensitivity and specificity of 79% and 93%, giving an AUROC of 0.94. Pa-NT was stiffer than control (p=0.01, figure 3). V-MRE (16.31±10.99 cm3) correlated excellently (r=0.974; p<0.0001) with V-CT (18.37±15.75 cm3), see figure 4.Discussion:
In our study cohort all PDAC were stiffer than normal tissue implying a clear change of the biophysical tissue properties due to tumor progression in the pancreas within distinct boundaries. From a biophysical perspective, these boundaries are related to energy barriers which have to be overcome by metastatic cells migrating into non-tumorous tissue. Tomoelastography is a quantitative MRE method which generates contrast by the change of wavelengths of shear waves e.g. when crossing through tumor boundaries. The observed correlation between V-CT and V-MRE is an encouraging result demonstrating that PDAC boundaries agree with perfusion-margins of the CT-contrast agent. This suggests that MRE might be useful in the future as endogenous-contrast based MRI technique for boundary mapping and tumor volume quantification in PDAC. The obtained stiffness contrast might also be of value for the differential diagnosis of malignant versus benign entities or mass forming pancreatitis.
Our pilot study reported normal values which can be used as control values for diagnosis. PDAC are associated with SWS values above 1.5 m/s. This is in agreement to Shi et al 3 who reported 3.3 kPa shear modulus which can be translated to SWS = 1.8 m/s (assuming 1 kg/L mass density). Our normal parenchymal values also agree with Shi et al 3 and Kolipaka et al 6. Kolipaka et al also analyzed the regional stiffness variation showing no effect 6 similar to our findings. However, other than this group, we observed no age effect possibly due to the low number of elderly subjects in our study cohort.
Conclusion:
In tomoelastography, stiff PDAC are highly contrasted by the very soft pancreatic tissue favoring the use of tomoelastography for boundary detection of pancreatic tumors within standardized, quantitative and contrast-agent free imaging examinations.Acknowledgements
The authors would like to thank the German Research Foundation for financial support (GRK2260, BIOQIC, SFB1340).References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin 2015;65:5-29.
2. Shi Y, Cang L, Zhang X, et al. The use of magnetic resonance elastography in differentiating autoimmune pancreatitis from pancreatic ductal adenocarcinoma: A preliminary study. Eur J Radiol 2018;108:13-20.
3. Shi Y, Gao F, Li Y, et al. Differentiation of benign and malignant solid pancreatic masses using magnetic resonance elastography with spin-echo echo planar imaging and three-dimensional inversion reconstruction: a prospective study. Eur Radiol 2018;28:936-45.
4. Muthupillai R, Ehman RL. Magnetic resonance elastography. Nat Med 1996;2:601-3.
5. Tzschatzsch H, Guo J, Dittmann F, et al. Tomoelastography by multifrequency wave number recovery from time-harmonic propagating shear waves. Med Image Anal 2016;30:1-10.
6. Kolipaka A, Schroeder S, Mo X, Shah Z, Hart PA, Conwell DL. Magnetic resonance elastography of the pancreas: Measurement reproducibility and relationship with age. Magn Reson Imaging 2017;42:1-7.
Figures