0639
The Stiffness as Obtained by MR Elastography Correlates with the Stroma Proportion and Prognosis of Resectable Pancreatic Adenocarcinomayu shi1, xianyi zhang1, xiaoli cai1, and fei yang1
1shengjing hospital of china medical university, shenyang, China
Synopsis
One of the defining characteristics of pancreatic adenocarcinoma (PDAC) is abundant desmoplastic stroma. Our study showed that pancreatic stiffness determined by magnetic resonance elastography (MRE) is a promising technique to predict the stroma proportion and shows potentials to predict prognosis of resectable PDAC.
Purpose
Abundant stroma is one of the most important features of PDAC that accounts for up to 90% of the tumor volume [1]. Studies have shown that the stroma component plays an important role in tumor growth, progression and chemoresistance in PDAC [2]. Recently, MRE showed that PDAC had significant higher MRE-determined stiffness than that of heathy volunteer and focal pancreatic inflammation [3]. However, the role of MRE in the prognostic prediction of PDAC remains unknown. Herein, our study was to investigate the value of the MRE-determined stiffness in evaluating the stroma proportion and the prognostic value of stiffness in resectable PDAC.Methods
A total of 47 resected PDAC patients (male/female: 27/20, mean age: 61.3yrs, range:33-75yrs) were prospectively enrolled in this study from Jan 2017 to Jan 2018, all without preoperative chemotherapy or radiotherapy. Both sirius-red staining and H&E staining was used to evaluate the stromal proportion in PDAC. MRE examinations were performed on a 3.0T MR scanner (Signa HDX 3.0T system; GE Healthcare, Milwaukee).The imaging parameters were as follows: frequency=40Hz; TR/TE = 1375/38.8ms; phase offsets = 3; FOV = 40 cm; matrix = 96×96; number of signal averages = 1; frequency-encoding direction = RL; parallel imaging acceleration factor = 3; number of slices = 32; thickness = 3.5mm. Survival rates were calculated according to the Kaplan–Meier method and were compared using the log rank test. Multivariate analysis was performed with a Cox regression model.Results
Figure 1 showed 2 PDAC cases with 15% and 64% different stroma proportions as examples, respectively. PDAC showed significantly higher stiffness (3.39±0.72 kPa) than that of the non-tumor pancreatic parenchyma (1.41±0.44 kPa) (P<0.001). The average stromal proportion was 45.5±21.1%. The pancreatic stiffness was positively associated with the stromal proportion of resected PDAC (r= 0.829, P < 0.001). The pancreatic stiffness was also positively correlated with TNM stage (AJCC 7th edition) (r= 0.700, P < 0.001) and tumor size (r= 0.680, P < 0.001). High pancreatic stiffness (>3.39kPa) predicted unfavorable overall survival (OS) relative to low pancreatic stiffness (22.4 vs. 35.1 months, P= 0.017). The pancreatic stiffness was an independent prognostic factor for resected PDAC based on multivariate analysis (hazard ratio =5.174, 95%CI:2.41-11.07 P <0.001).Discussion
MRE has been recently used for the staging of chronic pancreatitis and benign or malignant pancreatic tumor differentiation. In literature, pancreatic stiffness in PDAC has a broad range of increased stiffness [3]. Our study’s result further clearly demonstrated that this increased pancreatic stiffness was mainly determined by amount of stroma proportion, which predicted poor OS in resectable PDAC patients. The novel prognostic value of the pancreatic stiffness for resectable PDAC has been established. Our study was in consistence with an endoscopic elastography study obtaining strain ratio. Compared with endoscopic elastography, MRE is non-invasive, fast and improves patient comfort [4]. Further clinical and basic research studies would be helpful to clarify the underlying mechanisms and to see the correlation of MRE-determined stroma proportion with treatment response after chemotherapy.Conclusions
We demonstrated that the pancreatic stiffness obtained by MRE was positively associated with the stroma proportion in pancreatic cancer. Pancreatic stiffness can be a promising biomedical index for prognostic prediction in PDAC.Acknowledgements
We thank Richard Ehman, Meng Yin, Kevin Glaser and Ziying Yin from the Mayo Clinic for providing the MRE technical guidance. We also thank Jun Chen from the Mayo Clinic for his assistance with providing the tailored pancreatic MRE driver.References
[1] Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018; 68:7–30.[2] Erkan M, Hausmann S, Michalski CW, et al. The role of stroma in pancreatic cancer: diagnostic and therapeutic implications. Nat Rev Gastroenterol Hepatol. 2012; 9:454–467.[3] Shi Y, Gao F, Li Y, et al. Differentiation of benign and malignant solid pancreatic masses using magnetic resonance elastography with spin-echo echo planar imaging and three-dimensional inversion reconstruction: a prospective study. Eur Radiol. 201;28(3):936-945. [4] Shi S, Liang C, Xu J, et al. The Strain Ratio as Obtained by Endoscopic Ultrasonography Elastography Correlates With the Stroma Proportion and the Prognosis of Local Pancreatic Cancer. Ann Surg. 2018, doi: 10.1097/SLA.0000000000002998.Figures
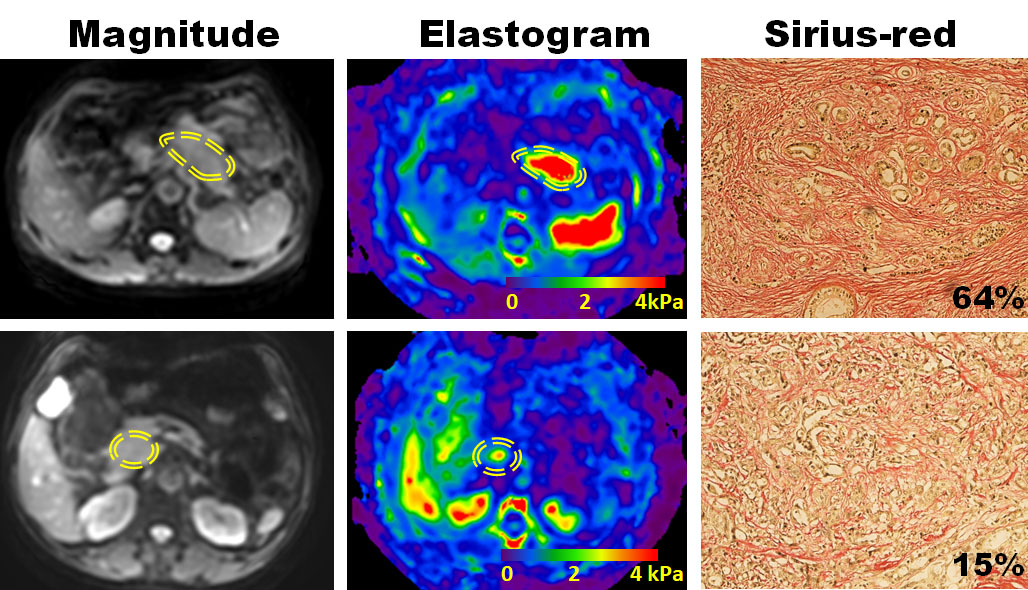
Figure 1. From left to right are the magnitude, elastogram and sirius-red
staining images for two PDAC cases with different stroma proportion. The
stiffness was 5.51±0.78kPa with 64% stroma on the first row, and
the stiffness was 1.99±0.54kPa with 15% stroma on the second row.