0635
Cortical thickness is a sensitive biomarker for characterizing the gray matter abnormities in neonates with mild white matter injury1Department of Diagnostic Radiology, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, China, 2Department of Radiology and BRIC, University of North Carolina at Chapel Hill, North Carolina, NC, United States, 3MR Research China, GE Healthcare, Beijing, China
Synopsis
White matter injury is common in neonates. The most common punctate white matter lesions (PWML) can disappear along with time and are easily missed diagnosis, but quantitative measurements may find more subtle alterations. Since DTI is not sensitive to detect the white-matter microstructural changes in mild PWML, alterations in gray-matter (GM) may provide additional knowledge for predicting prognosis. This study aims to quantitatively assess alterations of GM in neonates with mild PWML. Compared with controls, a significant reduction of cortical volume is observed in neonates with mild PWML, and cortical thickness is a sensitive biomarker for characterizing the GM abnormalities.
Introduction
White matter injury (WMI) is common in neonates, and the most common punctate white matter lesions (PWML) can be detected on conventional MRI as hyper-intensity on T1WI and hypo-intensity on T2WI.1 It is important to note that these lesions can gradually disappear along with time and are easily missed diagnosis.2 But even accurate assessment of the lesions on qualitative MRI images at different postnatal ages is difficult, quantitative measurements may find more subtle alterations. The extensive white matter (WM) microstructural abnormalities caused by PWML were reported in several DTI studies, but this method is not sensitive to the mild subgroup.1, 3 Additionally, WM abnormalities are known to disturb the development of the cortical gray matter (GM), which impacts cognition, motor and behavioral functions.4 However, little is known about the changes of GM in neonates with PWML, which may provide additional knowledge for predicting prognosis. Thus, this study aims to quantitatively assess the alterations of GM in neonates with mild PWML.Methods
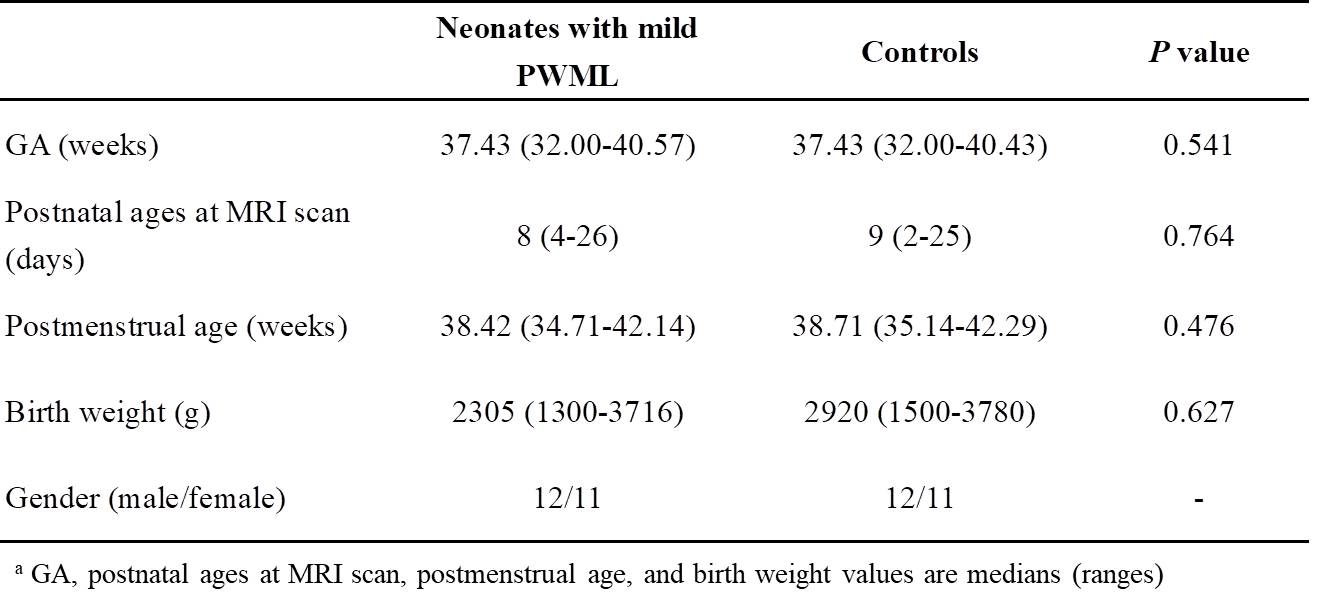
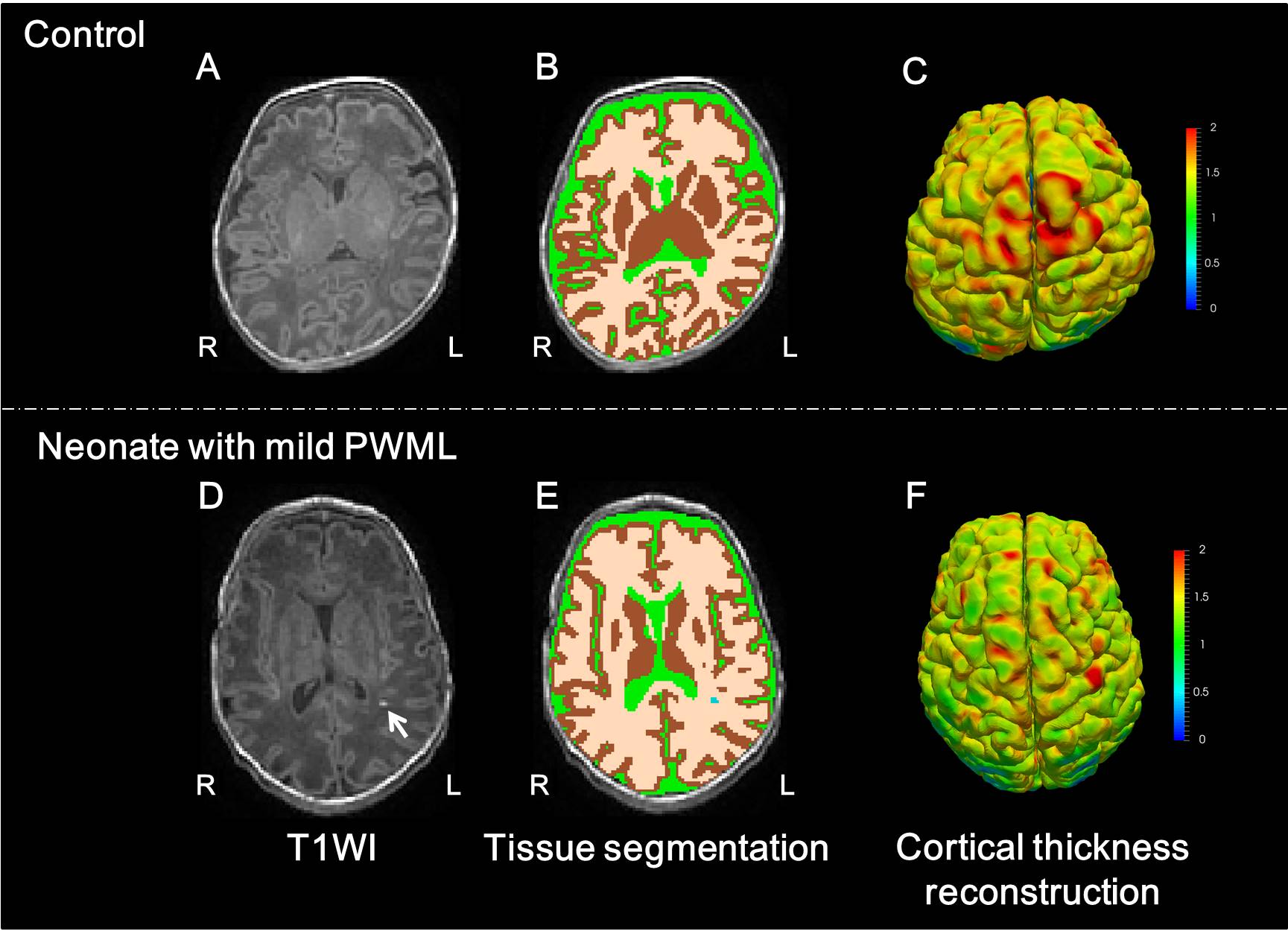
The local institutional review board approved this study and all the written informed consents were obtained from parents of neonates. Subjects Neonates with evidence of mild PWML (diagnosed by conventional MRI: ≤6 lesions or 1 large lesion [diameter≥5mm]) were included. Subjects with intraventricular hemorrhage, cerebral infarction, basal ganglia lesions and obvious imaging artifacts were excluded. Controls were matched for gestational age (GA), postnatal age at MRI scan, gender, and birth weight, and did not have any MRI abnormality. MRI Protocols All MR examinations were performed using a 3T scanner (Signa HDxt, GE Healthcare, Milwaukee, Wisconsin) with an 8-channel head coil. The parameters of transverse 3D-T1WI sequence were as follows: TR/TE=10ms/4.6ms; matrix=256×256; section-thickness=1mm with no gap; and FOV= 240mm. Data and statistical analysis Tissue segmentation was performed by using a deep learning method (Figure 1).5 The PWML volume, whole brain volume, total and relative cortical volume were calculated. All MR images were further processed by using the infant-specific pipeline to reconstruct the topologically-correct and accurate cortical surfaces.6 All cortical surfaces were then mapped on to a spherical surface, and aligned to the UNC 4D Infant Surface Atlas (https://www.nitrc.org/projects/infantsurfatlas), and parcellated as gyral-based regions.7 For each cortical vertex, multiple biologically-distinct cortical attributes were computed.8, 9 Finally, the total surface area (SA) and average cortical thickness (CT) in each region were computed. Wilcoxon signed-rank tests and paired t-tests were used for the group differences in demographics and cortical attributes between mild PWML and the matched controls, respectively. All statistical analysis were performed by using SPSS 19.0 (SPSS, Chicago, IL, USA); P<0.05 was considered as statistically significant difference.Results
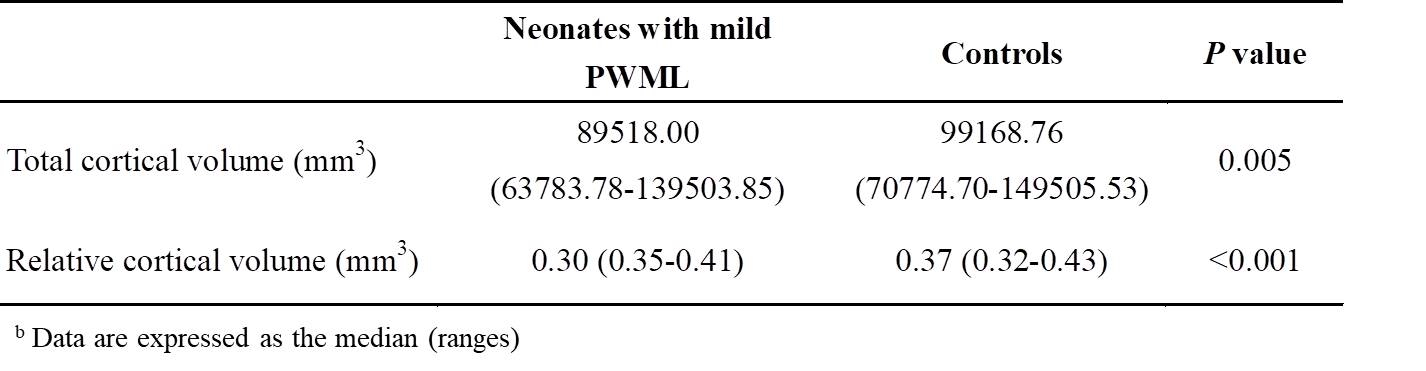
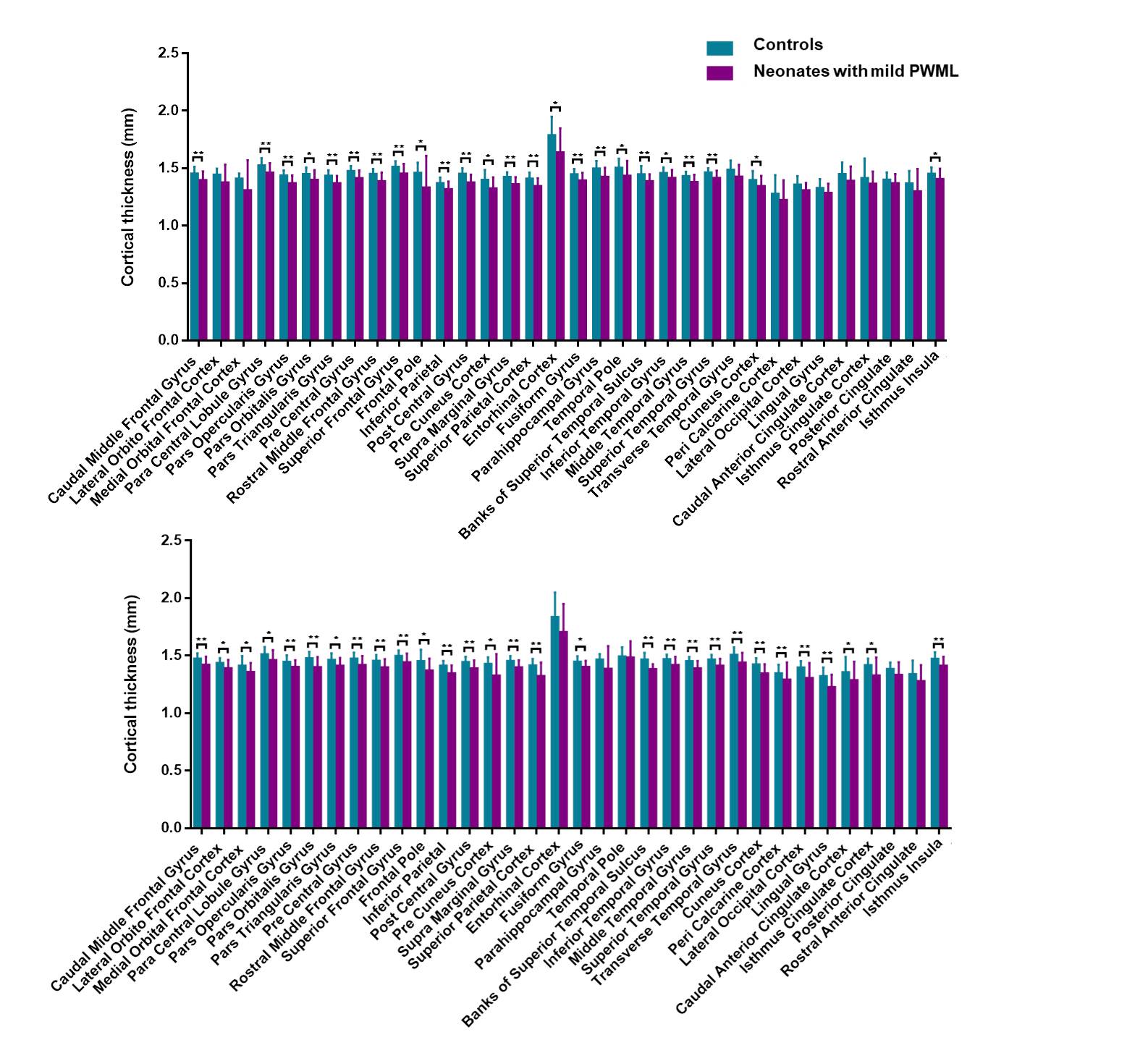
A total of 23 neonates (9 preterm and 14 term subjects, respectively) with mild PWML and 23 matched controls were enrolled. No significant differences in GA, postnatal ages at MRI scan, postmenstrual age, or birth weight were found between neonates with mild PWML and controls (Table 1).Compared with controls, the total and relative cortical volume were significantly decreased in PWML group (P<0.05, Table 2). Correcting the volume of the whole brain, the PWML volume was negatively with the total cortical volume (r=-0.37, P=0.029). Considering the different brain regions, no significant differences were found in SA between two groups (P>0.05). Moreover, significant thinning of CT was observed in many regions (frontal, parietal, temporal, and insula) of neonates with mild PWML (Figure 2).Discussion
This study quantitatively characterized the reduction in cortical volume in neonates with mild PWML, and CT showed extensive alterations compared to cortical SA. The processes that lead to WMI also damage neurons that migrate through WM, which may be the main cause of the GM damage. Additionally, excitotoxic and inflammatory processes that probably contribute to WMI are also able to effect developing neurons.4 The cortical volume is the product of the cortical SA and CT. According to the radial unit hypothesis, the cortical SA is determined by the number of neuron columns generated during the early embryonic period.10 Although these can be further regulated by afferents from subcortical and other cortical areas, it seems less susceptible affected by this perinatal mild PWML. In the third trimester and perinatal stage, neurons complete their migration to the cortical GM to makes the cortex gradually mature,10, 11 the disturbance of this process of neural migration and lamination due to PWML likely contribute to the extensive thinning of CT.Conclusion
Mild WMI affects the cortical development in neonatal period, and CT is a sensitive biomarker for characterizing the GM abnormalities.Acknowledgements
Miaomiao Wang, Jing Xia, and Jian Chen contributed equally to this study.
Corresponding authors (Gang Li, Dinggang Shen and Jian Yang) contributed equally to this study.
This work was supported by the grant from the National Key Research and Development Program of China (2016YFC0100300), National Natural Science Foundation of China (81171317, 81471631, 81771810), the 2011 New Century Excellent Talent Support Plan of the Ministry of Education, China (NCET-11-0438), the Clinical Research Award of the First Affiliated Hospital of Xi’an Jiaotong University (XJTU1AF-CRF-2015-004), the Fundamental Research Funds for the Central Universities (xjj2018265), and the Youth Innovation Fund of the First Affiliated Hospital of Xi’an Jiaotong University (2017QN-09).
References
1. Li X, Gao J, Wang M, et al. Characterization of extensive microstructural variations associated with punctate white matter lesions in preterm neonates. American Journal of Neuroradiology, 2017, 38(6): 1228-1234.
2. Kersbergen KJ, Benders MJ, Groenendaal F, et al. Different patterns of punctate white matter lesions in serially scanned preterm infants. PloS one, 2014, 9(10): e108904.
3. Bassi L, Chew A, Merchant N, et al. Diffusion tensor imaging in preterm infants with punctate white matter lesions. Pediatric research, 2011, 69(6): 561-566.
4. Leviton A, Gressens P. Neuronal damage accompanies perinatal white-matter damage. Trends in neurosciences, 2007, 30(9): 473-478.
5. Wang L, Li G, Adeli E, et al. Anatomy-guided joint tissue segmentation and topological correction for 6-month infant brain MRI with risk of autism. 2018, 39(6): 2609-2623.
6. Li G, Wang L, Shi F, et al. Construction of 4D high-definition cortical surface atlases of infants: Methods and applications. Medical image analysis, 2015, 25(1): 22-36.
7. Yeo BT, Sabuncu MR, Vercauteren T, et al. Spherical demons: fast diffeomorphic landmark-free surface registration. IEEE transactions on medical imaging, 2010, 29(3): 650-668.
8. Li G, Lin W, Gilmore JH, et al. Spatial Patterns, Longitudinal Development, and Hemispheric Asymmetries of Cortical Thickness in Infants from Birth to 2 Years of Age. J Neurosci, 2015, 35(24): 9150-9162.
9. Li G, Nie J, Wang L, et al. Mapping region-specific longitudinal cortical surface expansion from birth to 2 years of age. Cerebral cortex, 2013, 23(11): 2724-2733.
10. Rakic P. Specification of cerebral cortical areas. Science, 1988, 241(4862): 170-176.
11. Rajagopalan V, Scott JA, Liu M, et al. Complementary cortical gray and white matter developmental patterns in healthy, preterm neonates. Human brain mapping, 2017, 38(9): 4322-4336.
Figures