0630
In utero exposure to chemotherapy affects cortical neurodevelopment1Oncology, KU Leuven, Leuven, Belgium, 2Imaging and Pathology, KU Leuven, Leuven, Belgium, 3Radiology, University Hospitals Leuven, Leuven, Belgium, 4Development and Regeneration, KU Leuven, Leuven, Belgium, 5Gynaecology and Obstetrics, University Hospitals Leuven, Leuven, Belgium, 6Gynaecologic Oncology, Antoni van Leeuwenhoek, Amsterdam, Netherlands, 7Gynaecologic Oncology, Netherlands Cancer Institute, Amsterdam, Netherlands, 8Gynaecologic Oncology, Amsterdam university medical centers, Amsterdam, Netherlands
Synopsis
One in every 1000-2000 pregnancies is complicated by maternal cancer, for which chemotherapy is increasingly administered during pregnancy. However, only limited knowledge exists on the long-term impact of in utero exposure to cancer therapy. This study investigated the impact of prenatal exposure to chemotherapy, at the age of nine, on cortical development using surface-based morphometry. We found cortical thickness to be significantly lower in the superior part of the left pre-central sulcus of the prenatal-exposed children, compared to controls, whereas the gyrification index was significantly higher in the left post-central sulcus of this group, possibly impacting attentional development.
Introduction
One in every 1000-2000 pregnancies is complicated by maternal cancer1. Over the last 20 years clinical practice has evolved towards more cancer treatment during pregnancy, with chemotherapy in particular, being increasingly administered1. Simultaneously, less pregnancies are terminated and the rate of medically induced prematurity has decreased1. However, only limited knowledge exists on the long-term impact of in utero exposure to cancer therapy2–4.
Notwithstanding short-term clinical evidence on the safety of chemotherapy during pregnancy3–5, chemotherapy can possibly affect long-term cognitive development through a multitude of (in)direct pathways6. Moreover, while chemotherapy is contra-indicated during the first trimester of pregnancy due to the increased risk of congenital anomalies, it can be administered during the second and third trimester7. Brain development, however, accelerates through the second half of pregnancy with both nonlinear brain growth8 and gyrification9–12.
We investigated the long-term impact of in utero exposure to chemotherapy on cortical development by comparing surface-based morphometry parameters between exposed children and a matched control group.
Methods
Children were recruited via the Belgian cohort of the international follow-up study by the International Network on Cancer, Infertility, and Pregnancy (INCIP), after informed consent was provided by a legal guardian. Children in the prenatal-exposed group were born to mothers that were diagnosed with cancer and treated with chemotherapy during pregnancy, after the first trimester. Children in the control group were born to healthy mothers and matched on group level on gestational age (GA) at birth. Control children born after major neonatal complications, apart from prematurity itself, were excluded. All children were tested, at the age of 9 years, between 2015-2018, using the same scanner (3T Philips Achieva, 32-channel phased-array head coil) and with the same scanning protocol. The study was approved by the local ethical commission and conducted in accordance with the Declaration of Helsinki.
High-resolution whole brain T1-weighted MR images (MPRAGE, resolution=.98x.98x1.2mm, TR/TE=9.6/4.6 ms, FOV=160x256x256mm) were acquired from every participant. Images of poor quality (e.g. motion artifacts) were excluded by a blinded neuroradiologist.
All images were first corrected for biasfield, using ANTs N4 Biasfield correction13. Next, a population-specific template was created using DARTEL14. Afterwards, the spm1215 CAT1216 toolbox was used for surface registration and the calculation of both cortical thickness and gyrification index (GI). These parameters were smoothed along the surface with a gaussian kernel of 15mm. Finally, we compared both groups using an unpaired t-test, with GA as a covariate. Additionally, we investigated the influence of GA on both surface parameters within this model. Significance was assessed at p<.05, family-wise-error corrected on cluster level with an uncorrected vertex-wise threshold of p<.001.
Results
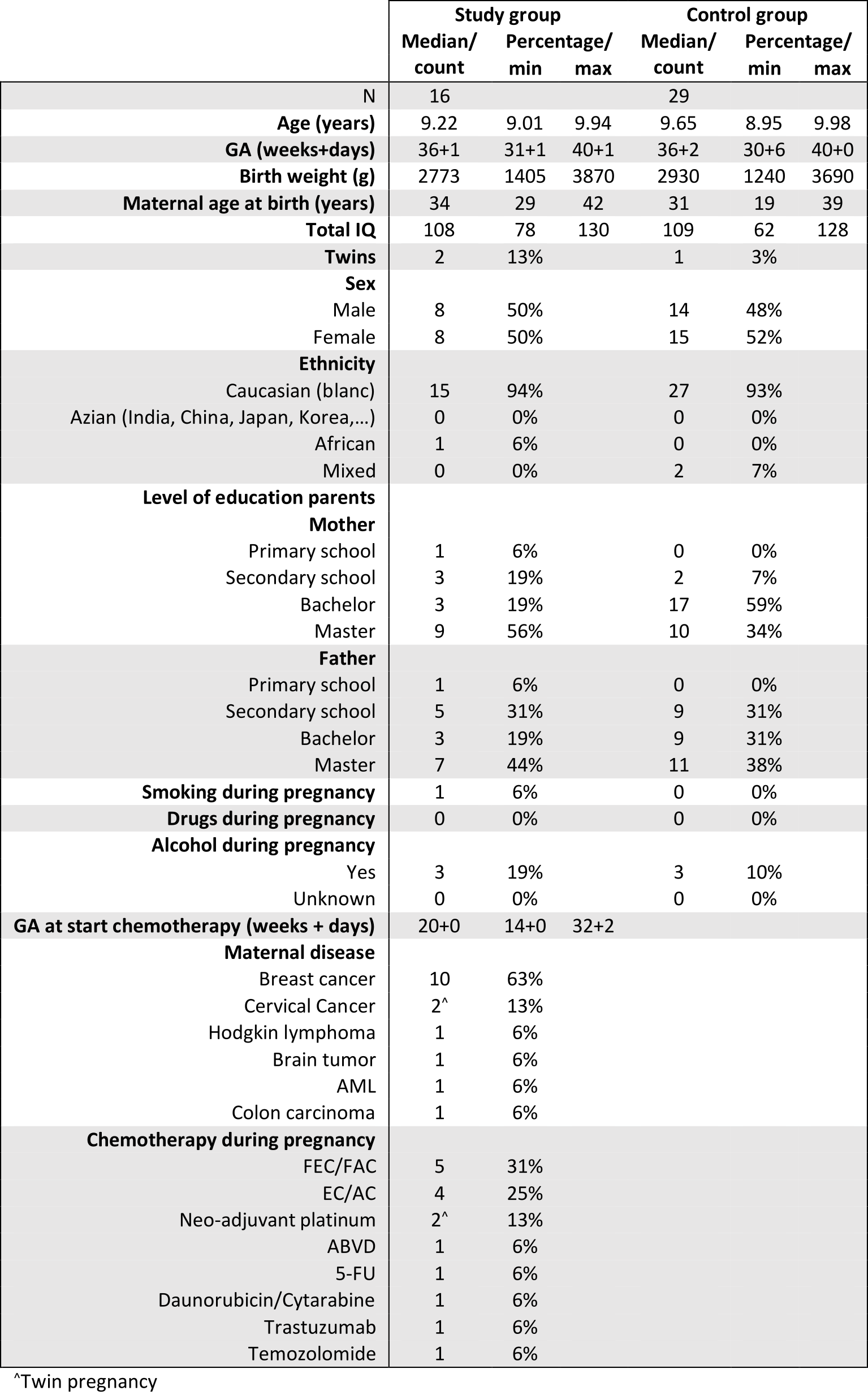
We included data of 18 children prenatally exposed to chemotherapy and 37 control children. Two controls had to be excluded due to incidental findings. Two children of the prenatal-exposed group and six control children were excluded due to extensive motion artifacts. Demographics after exclusion are shown in Figure 1.
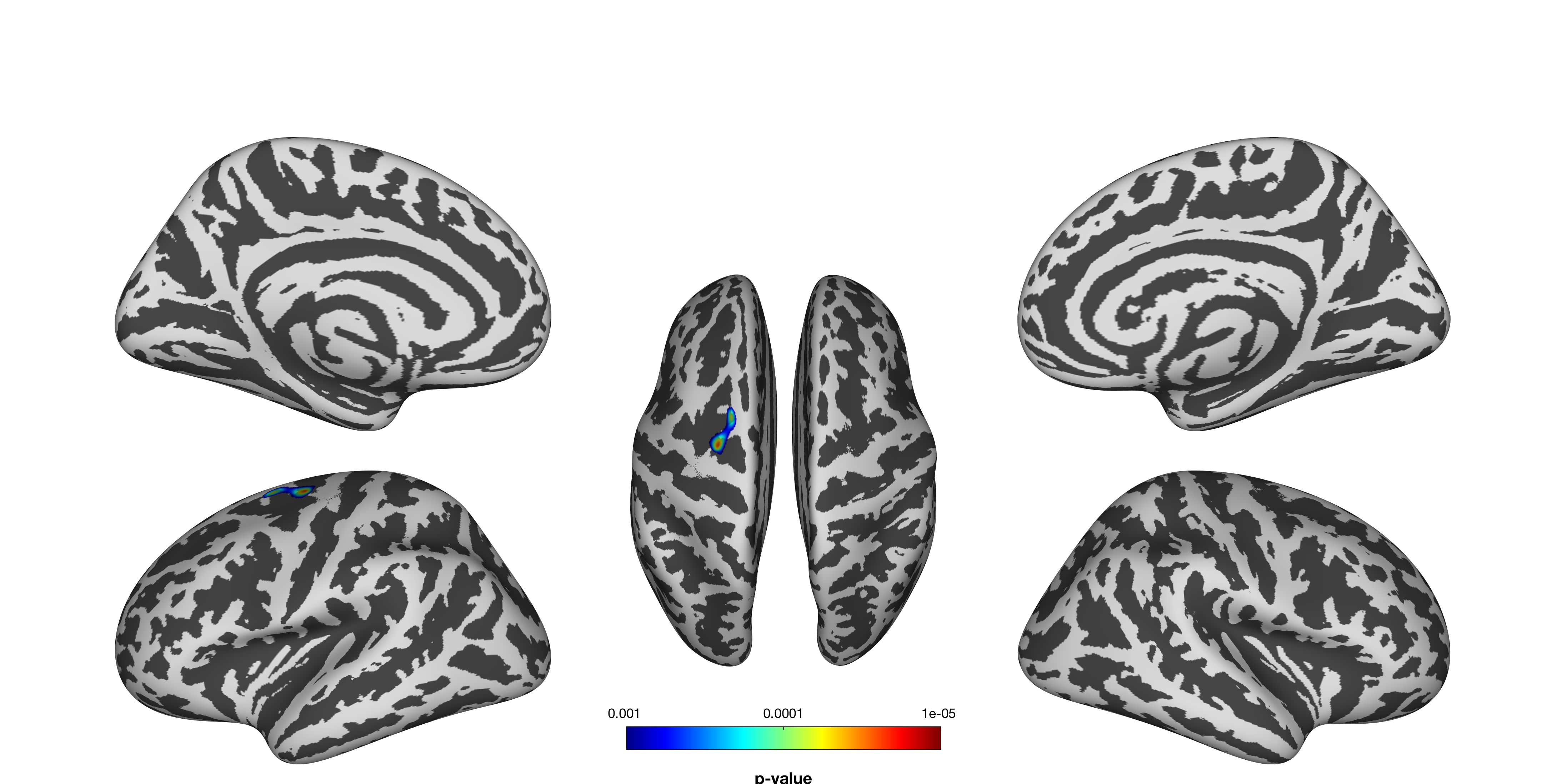
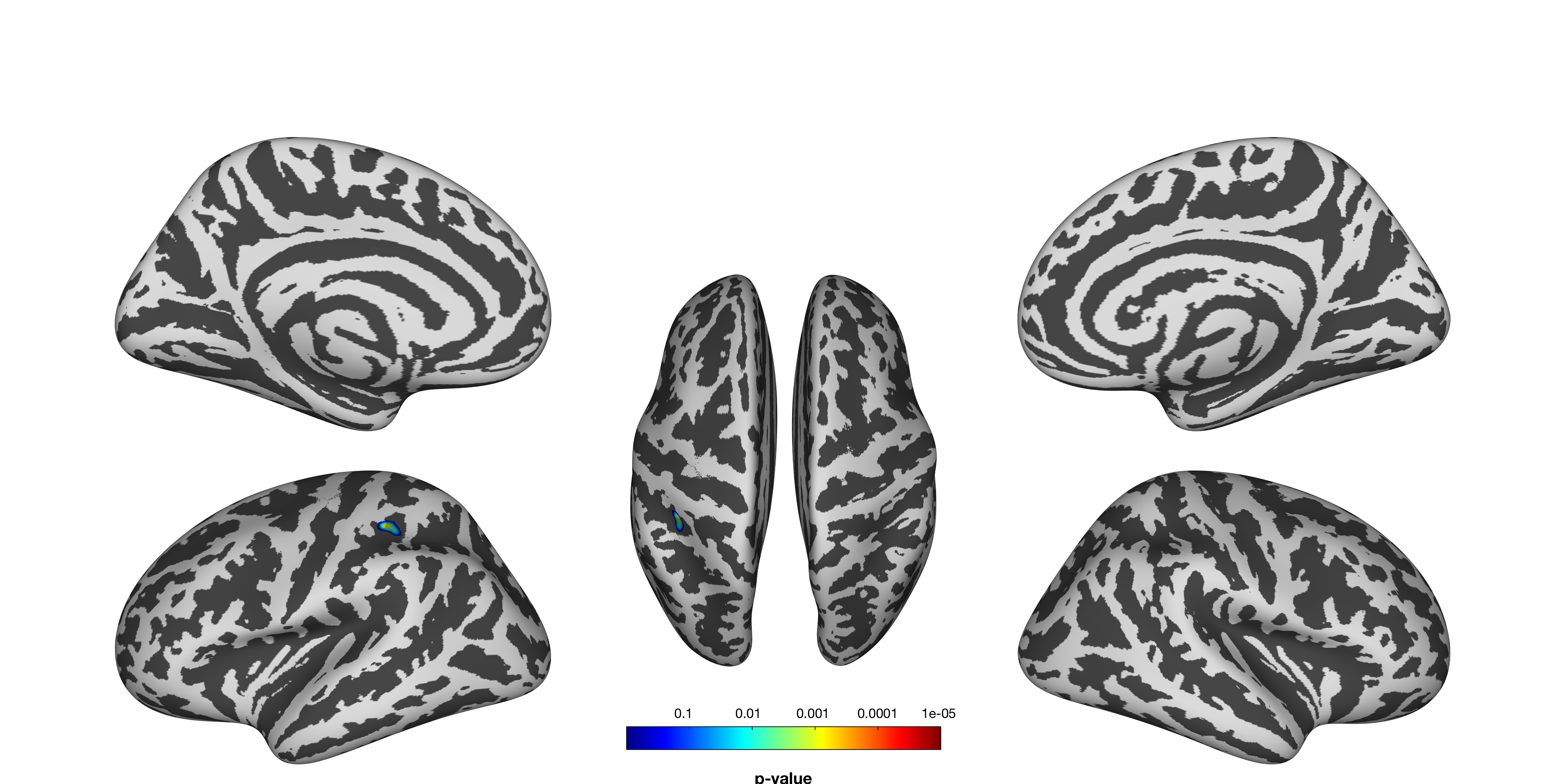
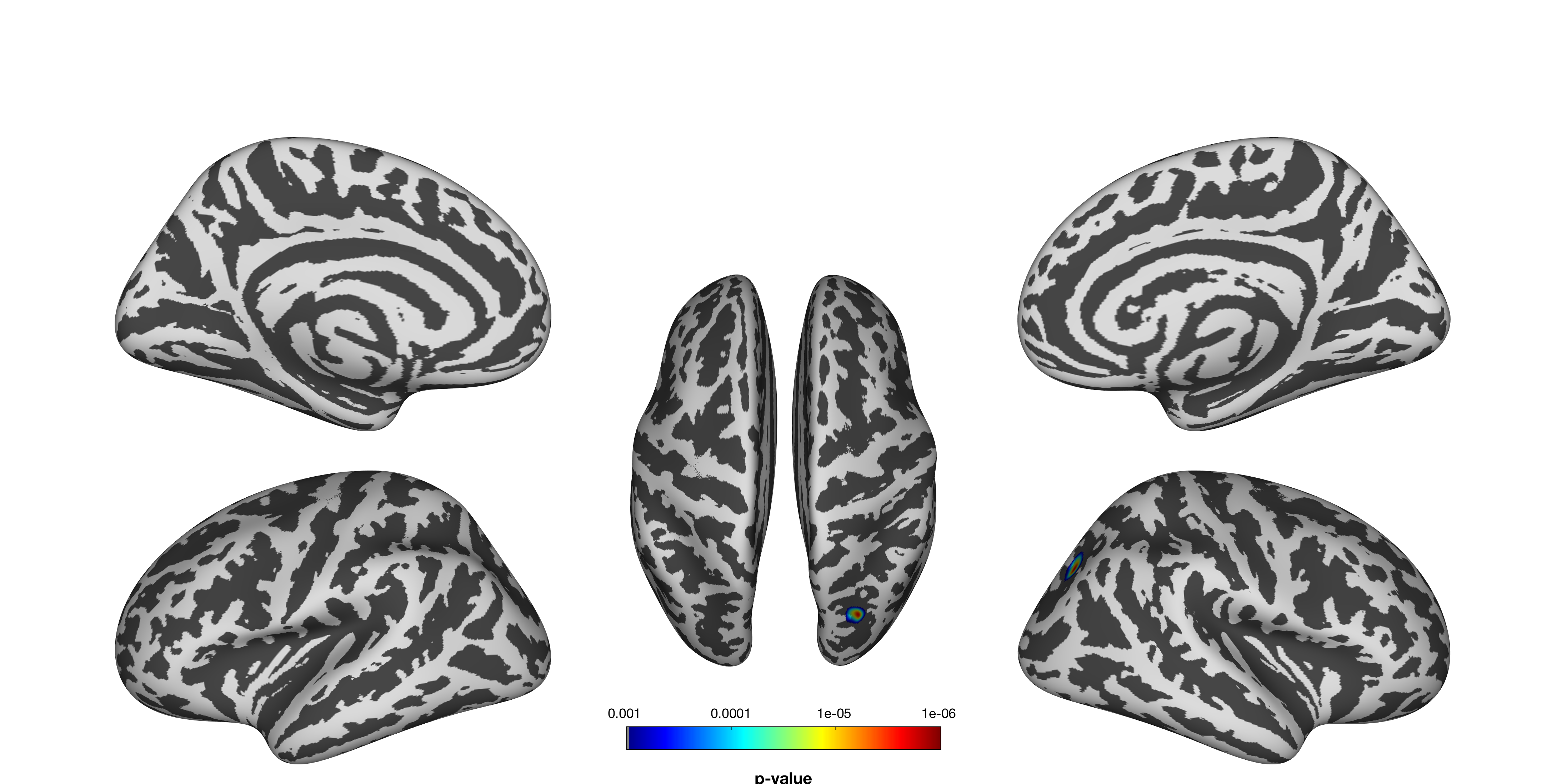
Cortical thickness was found to be significantly lower in the prenatal-exposed group in the superior part of the left pre-central sulcus (Figure 2), whereas GI was significantly higher in this group in the left post-central sulcus (Figure 3). GA did not significantly correlate with cortical thickness, but did correlate significantly with higher GI in the right superior transversal occipital sulcus (Figure 4).
Discussion
The findings in the left pre- and post-central sulci might indicate an effect of prenatal exposure to chemotherapy on neural development. Moreover, both regions are closely linked to attention and executive control functioning17–19. These findings indicate that development of these cognitive functions, through childhood and adolescence19, might be affected in these children. The higher gyrification found in the post-central sulcus might indicate a subclinical polymicrogyric tendency. Finally, the observation of higher gyrification with higher GA corroborates with earlier findings showing the possible discrepancy between intra- and extra-uterine cortical development10.Conclusion
To our knowledge, this is the first study to investigate brain development after prenatal exposure to chemotherapy. The findings suggest that prenatal exposure to chemotherapy impacts cortical development through both thickness and gyrification, possibly influencing attentional development. These results need validation in a larger sample, which is currently being collected.Acknowledgements
This project has received funding from the European Union’s Horizon 2020 research and innovation program(European Research council, grant no 647047), Foundation against cancer (Stichting tegen kanker, grant no. 2014-152) and Research Foundation Flanders (FWO, grant no. 11B9919N), J.B. and T.V. are aspirant researchers for the FWO, F.A. and S.S. are senior clinical researchers for the FWO.
The authors would like to thank: Jorine De Haan, Gunnar Naulaers, Charlotte Maggen, Liesbeth Leemans, Kaat Philippe, Cettina Schellens, Marie-Astrid Van Hoorick, Dorothée Vercruysse, Magali Verheecke and Diane Wolput.
References
1. de Haan J, Verheecke M, Van
Calsteren K, et al: Oncological management and obstetric and neonatal outcomes
for women diagnosed with cancer during pregnancy: a 20-year international
cohort study of 1170 patients [Internet]. Lancet Oncol 2045:1–10, 2018
2. Deprez S, Amant F, Smeets A, et al: Longitudinal Assessment of Chemotherapy-Induced Structural Changes in Cerebral White Matter and Its Correlation With Impaired Cognitive Functioning [Internet]. J Clin Oncol 30:274–281, 2012
3. Amant F, Vandenbroucke T, Verheecke M, et al: Pediatric Outcome after Maternal Cancer Diagnosed during Pregnancy. [Internet]. N Engl J Med 373:1824–34, 2015
4. Cardonick EH, Gringlas MB, Hunter K, et al: Development of children born to mothers with cancer during pregnancy: Comparing in utero chemotherapy-exposed children with nonexposed controls [Internet]. Am J Obstet Gynecol 212:658.e1-658.e8, 2015
5. Amant F, Van Calsteren K, Halaska MJ, et al: Long-term cognitive and cardiac outcomes after prenatal exposure to chemotherapy in children aged 18 months or older: an observational study [Internet]. Lancet Oncol 13:256–264, 2012
6. Vercruysse DC-M, Deprez S, Sunaert S, et al: Effects of prenatal exposure to cancer treatment on neurocognitive development, a review.
7. Amant F, Han SN, Gziri MM, et al: Management of cancer in pregnancy. [Internet]. Best Pract Res Clin Obstet Gynaecol 29:741–753, 2015
8. Scott JA, Habas PA, Kim K, et al: Growth trajectories of the human fetal brain tissues estimated from 3D reconstructed in utero MRI [Internet]. Int J Dev Neurosci 29:529–536, 2011
9. Rajagopalan V, Scott J, Habas PA, et al: Local Tissue Growth Patterns Underlying Normal Fetal Human Brain Gyrification Quantified In Utero [Internet]. J Neurosci 31:2878–2887, 2011
10. Clouchoux C, Kudelski D, Gholipour A, et al: Quantitative in vivo MRI measurement of cortical development in the fetus [Internet]. Brain Struct Funct 217:127–139, 2012
11. Habas PA, Scott JA, Roosta A, et al: Early Folding Patterns and Asymmetries of the Normal Human Brain Detected from in Utero MRI [Internet]. Cereb Cortex 22:13–25, 2012
12. Wright R, Kyriakopoulou V, Ledig C, et al: Automatic quantification of normal cortical folding patterns from fetal brain MRI [Internet]. Neuroimage 91:21–32, 2014
13. Tustison NJ, Avants BB, Cook PA, et al: N4ITK: Improved N3 Bias Correction [Internet]. IEEE Trans Med Imaging 29:1310–1320, 2010
14. Ashburner J: A fast diffeomorphic image registration algorithm. Neuroimage , 2007
15. Friston K, Holmes A, Worsley K: Statistical parametric maps in functional imaging: a general linear approach. Hum Brain Mapp , 1994 16. Gaser C, Dahnke R: CAT - A Computational Anatomy Toolbox for the Analysis of Structural MRI Data, in HBM Conference 2012. 2012, p 7743
17. van den Heuvel MP, Hulshoff Pol HE: Exploring the brain network: A review on resting-state fMRI functional connectivity [Internet]. Eur Neuropsychopharmacol 20:519–534, 2010
18. Fernandez-Duque D, Posner MI: Brain imaging of attentional networks in normal and pathological states. [Internet]. J Clin Exp Neuropsychol 23:74–93, 2001
19. Karbach J, Unger K: Executive control training from middle childhood to adolescence. [Internet]. Front Psychol 5:390, 2014
Figures