0629
Fetal diffusion MRI acquisition and analysis in the developing Human Connectome Project1Centre for the Developing Brain, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Biomedical Engineering Department, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom
Synopsis
Fetal diffusion MRI (dMRI) can offer unique insight in brain development during the period of rapid, formative growth in the third trimester of pregnancy. The developing Human Connectome Project (dHCP) aims to create a comprehensive mapping of brain connectivity development in a large neonatal and fetal imaging cohort. Here, we design a state-of-the-art acquisition and analysis pipeline for fetal dMRI, including closely integrated dynamic distortion correction and slice-to-volume motion correction. We present results in the first 125 fetal dHCP subjects acquired, demonstrating high quality motion and distortion corrected output in the large majority of subjects and across a broad age range.
Introduction
Fetal diffusion MRI (dMRI) can offer unique insight in brain development during the period of rapid, formative growth in the third trimester of pregnancy. However, analysis of fetal dMRI data is complicated by motion due to maternal breathing and due to the fetus itself 1-4. At 3T there can also be significant dynamically changing EPI distortion originating from the dynamically changing “static” magnetic (B0) field 5. These challenges can best be addressed with a close integration of the acquisition protocol and subsequent postprocessing.
In this work, we present the acquisition protocol and design the analysis pipeline for fetal dMRI in the developing Human Connectome Project (dHCP). This includes denoising; dynamic distortion correction; radiofrequency field (B1) inhomogeneity correction; slice-to-volume motion correction; brain masking; and voxel-level fibre orientation modelling.
Methods
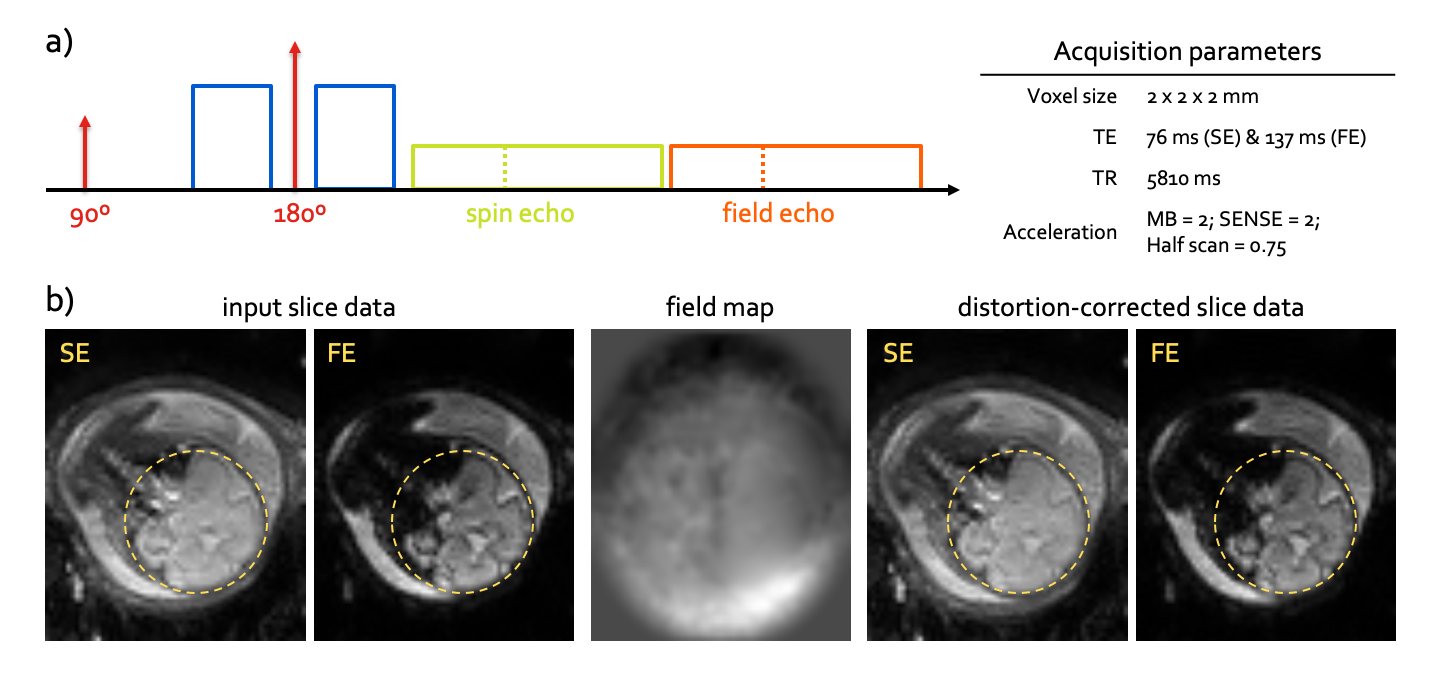
Acquisition: Following informed consent, all fetal dHCP data is acquired on a Philips Achieva 3T system with a 32-channel cardiac coil in supine position. dMRI is acquired with a combined spin echo and field echo (SAFE) sequence 6 at 2mm isotropic resolution (Fig.1). The diffusion encoding consists of 15 volumes at b=0s/mm2, 46 volumes at b=400s/mm2, and 80 volumes at b=1000s/mm2 (141 in total), as designed using a data-driven method 7. The total dMRI scan time is 13:45 min.
Processing pipeline:
- Marcenko-Pastur Principal Component Analysis image denoising 8 of the complex (phase-magnitude) dMRI data with optimal shrinkage prior 9.
- Dynamic distortion correction of susceptibility-induced B0 field changes, based on the phase difference between field and spin echoes from a dual hybrid EPI readout 6.
- Static B1 inhomogeneity correction using ANTs N4 10. The bias field is estimated from the mean b=0 spin echo image and applied to the entire image series.
- Fetal brain masking for slice-to-volume reconstruction, derived from the complex-averaged b=1000s/mm2 data, using intensity thresholding, connected component analysis and median filtering.
- Fetal and maternal motion occurs on a sub-TR time scale, motivating the need for slice-to-volume motion correction. We therefore use an iterative slice-to-volume reconstruction framework that alternates between updating a (low-rank) multi-shell data representation 11 from current motion parameters, and updating the motion parameters with image registration to the current representation 12. This framework also incorporates slice-level outlier suppression, and appropriately accounts for dMRI gradient reorientation 13.
- Local modelling of the diffusion tensor 14, including mean diffusion and fractional anisotropy contrasts, as well as the fibre orientation distribution with constrained spherical deconvolution 15.
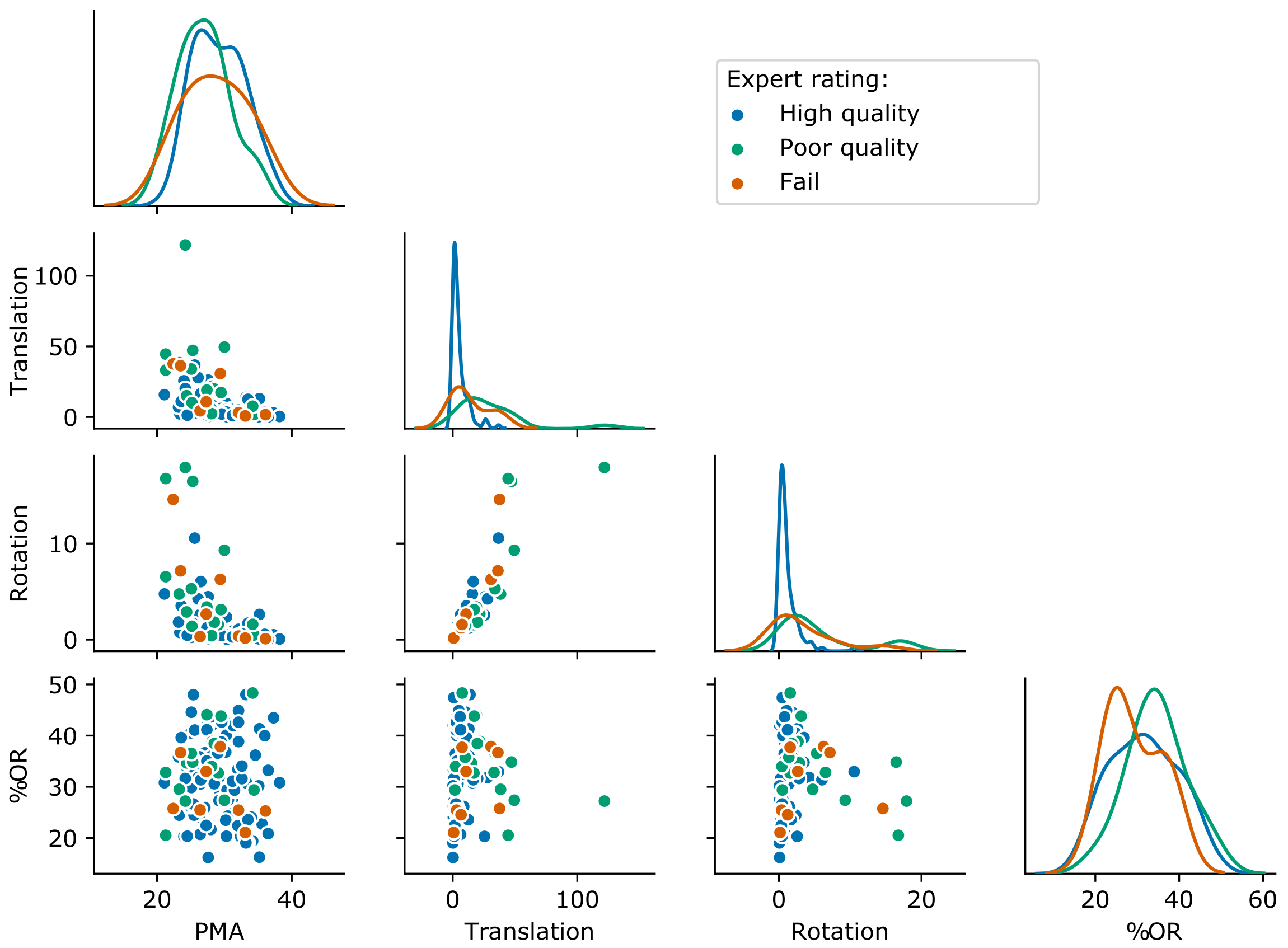
- Quality assessment using metrics of the motion traces and slice outlier weights, as well as expert rating of the reconstructions. The motion metrics are defined as the root-mean-squared forward difference of translation and rotation traces (a.u.).
Results
Out of 140 subjects (postmenstrual age range 21-38 weeks (wPMA)) scanned to date, 125 have complete dMRI acquisition data and these were processed in a fully automated manner. Expert rating identified 10 processing failures due to an incomplete field-of-view, unresolved distortion or severe misalignment; 17 poor quality cases; and 98 high quality reconstructions. Figure 2 shows that the distribution of quantitative quality metrics in the population is generally uncorrelated to the fetal gestational age, and that high quality reconstructions are obtained across a broad range of motion and outlier metrics.
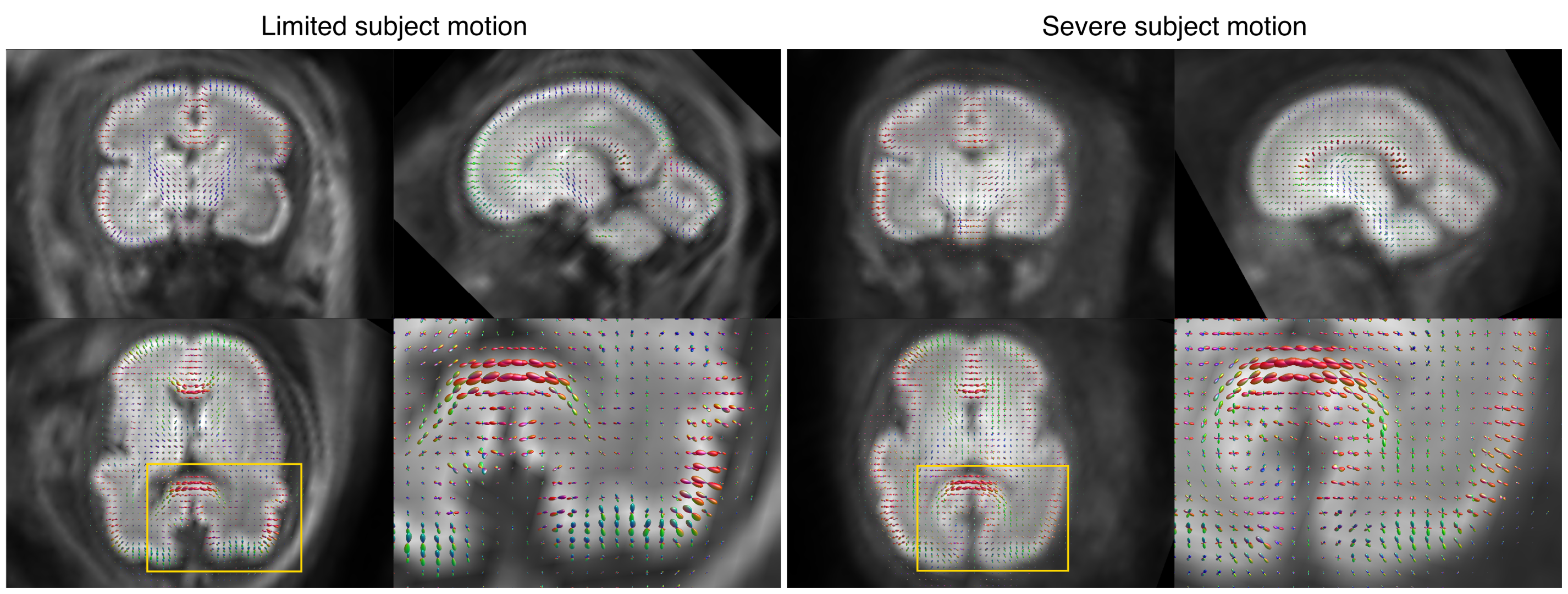
In Figure 3, we compare reconstructions in two subjects of approximately the same gestational age, chosen at the 10% and 90% percentiles for the group as a whole in the rotation metric. We observe similar image quality irrespective of the amount of subject motion, although with slightly less sharpness in the motion-corrupted subject.
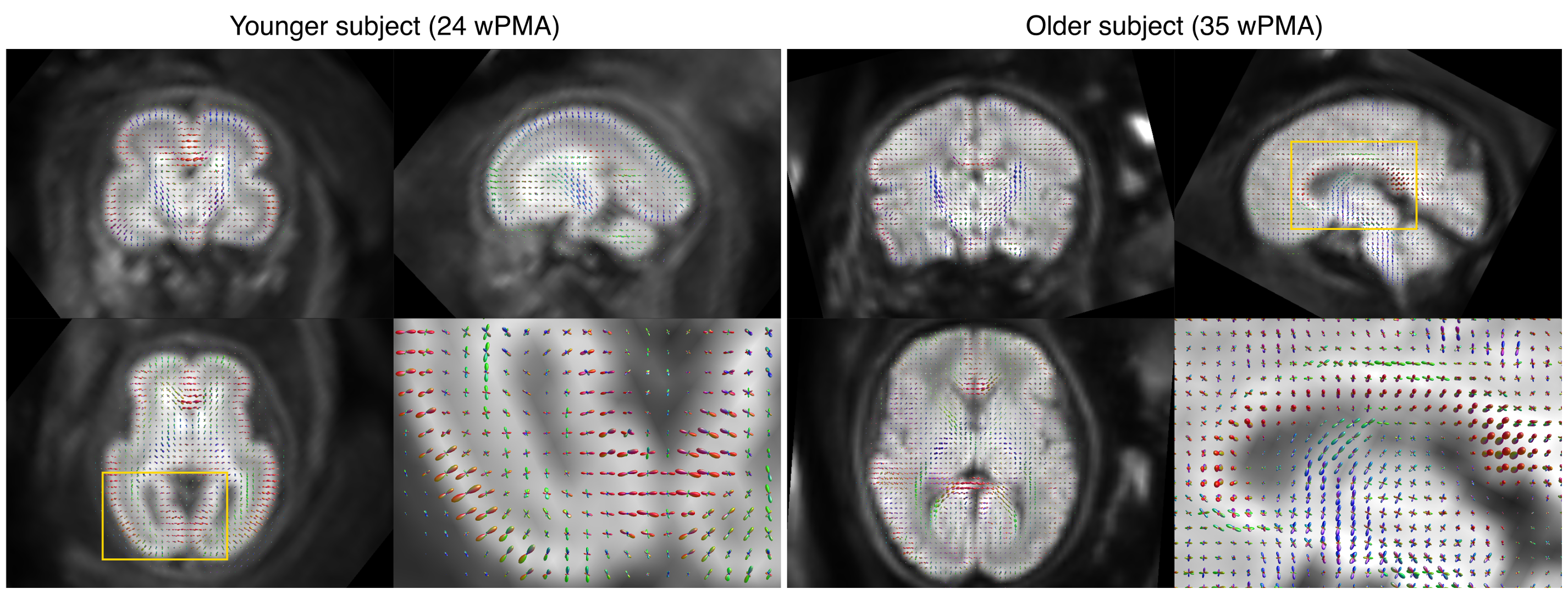
Figure 4 shows reconstructions in a young subject (24 wPMA) and in an older subject (35 wPMA), illustrating the change in brain microstructure during this period of rapid brain growth. In the younger subject, the radial fibre orientation in the bright cortical rim stands out. In the older subject, core white matter fibre bundles such as the corpus callosum and fornix become more developed.
Conclusion
The integrated acquisition and analysis pipeline for fetal diffusion MRI in the dHCP produces high quality motion and distortion corrected output data in the large majority of subjects and across a broad age range. Future work will aim to recover the damaged cases and automate pose correction; extend the analysis with more advanced local modelling and tractography; and construct age-resolved dMRI population atlases.Acknowledgements
This work was supported by ERC grant agreement no. 319456 (dHCP project), the Wellcome EPSRC Centre for Medical Engineering at King's College London [WT 203148/Z/16/Z] and by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.References
- Jiang S, Xue H, Counsell S. Diffusion tensor imaging (DTI) of the brain in moving subjects: application to in-utero fetal and ex-utero studies. Magn Reson Med 2009; 62(3):645-655.
- Oubel E, Koob M, Studholme C, Dietemann J-L, Rousseau F. Reconstruction of scattered data in fetal diffusion MRI. Med Image Anal 2012; 16(1):28-37.
- Fogtmann M, Seshamani S, Kroenke C, Cheng X, Chapman T, Wilm J, Rousseau F, Studholme C. A unified approach to diffusion direction sensitive slice registration and 3-D DTI reconstruction from moving fetal brain anatomy. IEEE Trans Med Imaging 2014; 33(2):272-289.
- Kuklisova-Murgasova M, Daducci A, Lockwood-Estrin G, Christiaens D, Rutherford M, Tournier J-D, Bach M, Hajnal JV. Reconstruction of fetal diffusion MRI using a spherical harmonic model. ISMRM 2017; 25:1747.
- Hutter J, Christiaens D, Schneider T, Cordero-Grande L, Slator PJ, Deprez M, Price AN, Tournier J-D, Rutherford M, Hajnal JV. Slice-level diffusion encoding for motion and distortion correction. Med Image Anal 2018; 48:214-229.
- Cordero-Grande L, Price AN, Ferrazzi G, Hutter J, Christiaens D, Hughes E, Hajnal JV. Spin And Field Echo (SAFE) dynamic field correction in 3T fetal EPI. ISMRM 2018; 26:O208.
- Tournier J-D, Hughes E, Tusor N, Sotiropoulos SN, Jbabdi S, Andersson J, Rueckert D, Edwards AD, Hajnal JV. Data-driven optimisation of multi-shell HARDI. ISMRM 2015; 23:2897.
- Veraart J, Novikov DS, Christiaens D, Ades-Aron B, Sijbers J, Fieremans E. Denoising of diffusion MRI using random matrix theory. NeuroImage 2016;142:394-406.
- Nadakuditi RR. Optshrink: An algorithm for improved low-rank signal matrix denoising by optimal, data-driven singular value shrinkage. IEEE Trans Inf Theory 2014; 60(5):3002–3018.
- Tustison NJ, Avants BB, Cook PA, Zheng Y, Egan A, Yushkevich PA, Gee JC. N4ITK: improved N3 bias correction. IEEE Trans Med Imaging 2010; 29(6):1310-20.
- Christiaens D, Cordero-Grande L, Hutter J, Price AN, Deprez M, Hajnal JV, Tournier J-D. Learning compact q-space representations for multi-shell diffusion-weighted MRI. IEEE Trans Med Imaging 2018; in press.
- Christiaens D, Cordero-Grande L, Pietsch M, Hutter J, Edwards AD, Deprez M, Hajnal JV, Tournier J-D. Multi-shell SHARD reconstruction from scattered slice diffusion MRI data in the neonatal brain. ISMRM 2018; 26:O464.
- Leemans A, Jones DK. The B-matrix must be rotated when correcting for subject motion in DTI data. Magn Reson Med 2009; 61(6):1336-49.
- Basser PJ, Mattiello J, Le Bihan D. MR Diffusion Tensor Spectroscopy and Imaging. Biophysics Journal 1994; 66:259-267.
- Tournier J-D, Calamante F, Connelly A. Robust determination of the fibre orientation distribution in diffusion MRI: non-negativity constrained super-resolved spherical deconvolution. NeuroImage 2007; 5(4):1459-72.
Figures