0628
The feasibility and clinical value of single-direction diffusion-weighted imaging in the fetal corpus callosum1MRI, Shandong Medical Imaging Research Institute, Shandong University, Jinan, China, 2MR Collaboration AP, Siemens Healthcare, MR Collaboration AP, Beijing, China, 3Obstetrics, Jinan Maternity and Child Care Hospital, Jinan, China
Synopsis
We investigated the value and feasibility of single-direction diffusion-weighted imaging for the assessment of the fetal corpus callosum in 67 healthy fetuses and 26 fetuses with corpus callosum dysplasia. The results showed that single-direction DWI is significantly superior in optimal visibility and contrast ratio (CR) compared to the conventional HASTE and TrueFISP sequences. This study demonstrated that the application of single-direction DWI is promising in fetal corpus callosum lesions and can be used in routine clinical examination.
Introduction
MRI is a crucial method for the non-invasive diagnosis of fetal corpus callosum lesions[1]. However, commonly used half-Fourier acquisition single-shot turbo spin-echo (HASTE) and true fast imaging with steady-state precession (TrueFISP) methods sometimes cause the diagnosis of corpus callosum lesions, particularly partial dysplasia, to be missed. Previous studies have described single-direction diffusion-weighted imaging (DWI) with background suppression, which is now widely used in clinical practice. It uses the characteristics of neurophysiological diffusion limitation, and can provide clear visualization of nerve roots and brachial plexus [2]. However, the single-direction DWI has yet to be applied to the examination of the fetal corpus callosum[3]. This study aimed to explore the feasibility and advantages of single-direction DWI for the depiction of normal fetal corpus callosum and to compare the capability of detecting corpus callosum lesions with conventional sequences.Methods
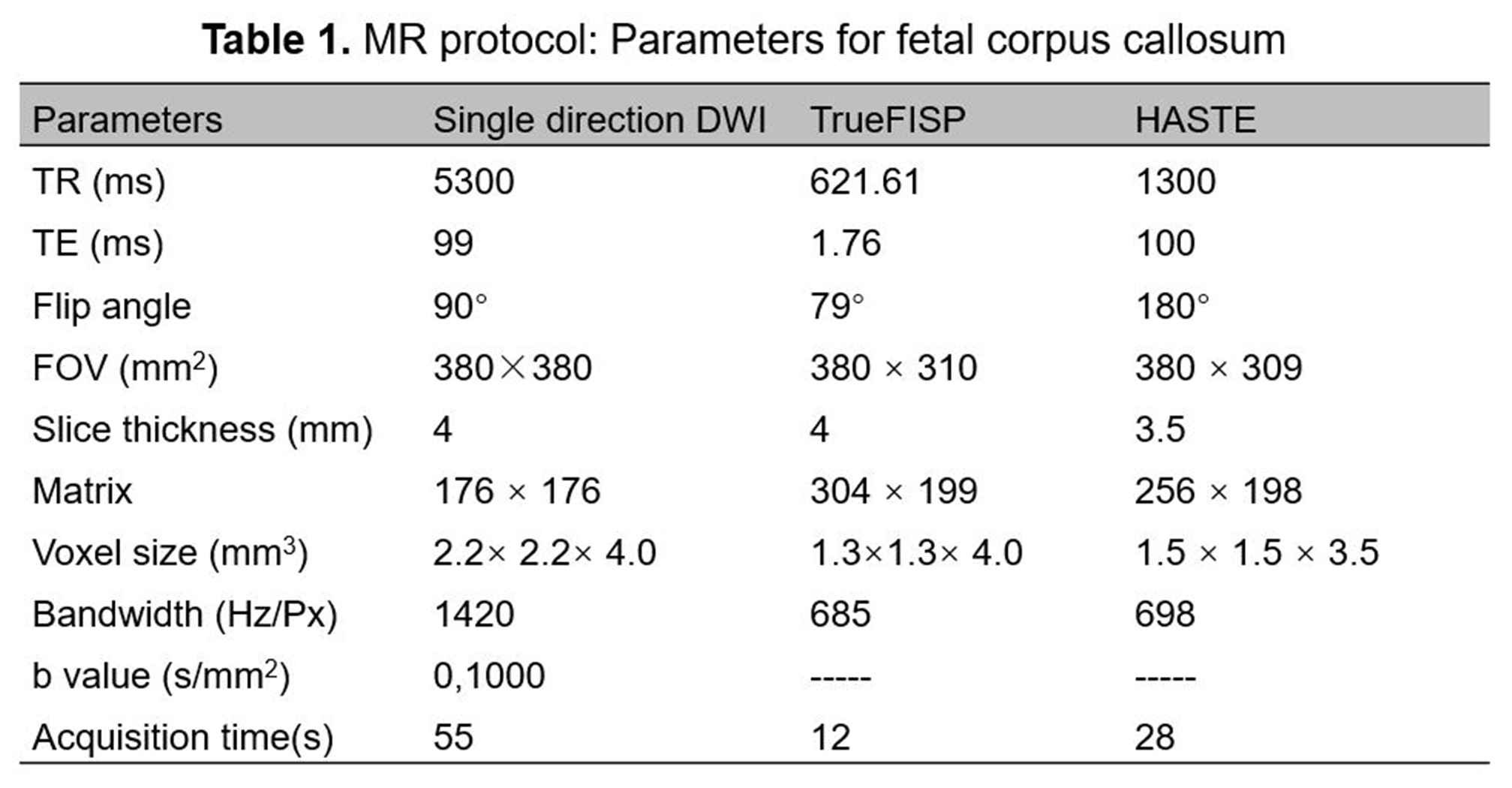
A total of 67 fetuses (gestational age (GA) 22 – 39 weeks) with normal corpus callosum development and 26 fetuses (GA 24 – 36 weeks) with confirmed corpus callosum dysplasia were enrolled. All the subjects underwent MRIs of the brain pre- and postnatally. The MRI data were acquired on a 1.5 T MAGNETOM Amira (Siemens Shenzhen Magnetic Resonance, Ltd., China) with a 13-channel body coil. The MR protocols included HASTE, TrueFISP, and single-direction DWI. The single-direction DWI was performed using a single-shot EPI sequence and only applied the gradient in a single direction, perpendicular to the corpus callosum. The detailed parameters are listed in Table 1.
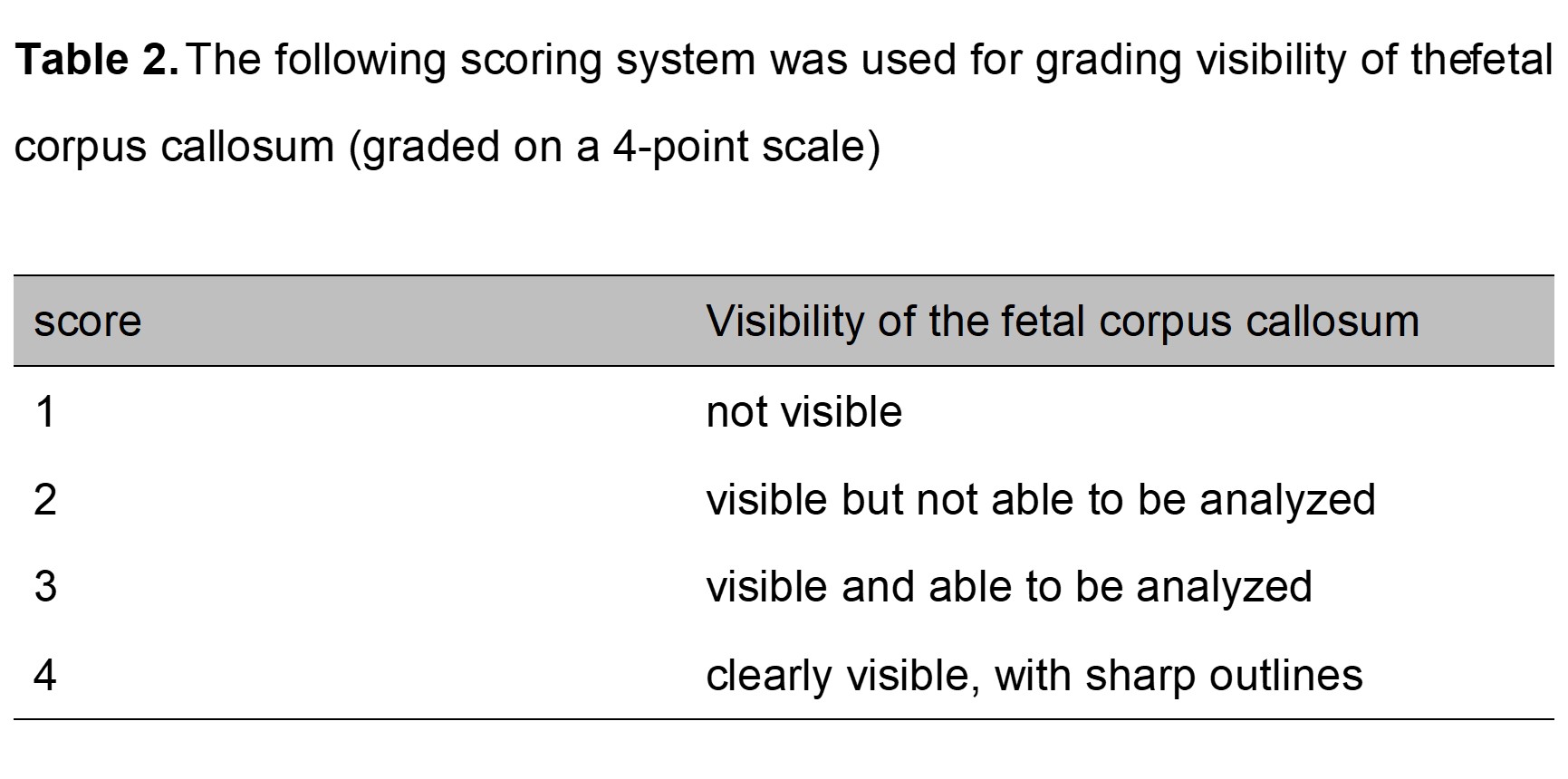
Two radiologists independently evaluated multiple parameters of image quality both qualitatively and quantitatively: the optimal visibility of the corpus callosum (graded on a 4-point scale [4], Table 2) and the contrast ratio (CR) were calculated and analyzed statistically. The CR between the corpus callosum and its surrounding normal brain tissue was calculated as follows: CR=(SIcorpus callosum - SInormal brain tissue) / (SIcorpus callosum + SInormal brain tissue) [5] , where SIcorpus callosum is the signal intensity of the corpus callosum, and SInormal brain tissue is the signal intensity of the normal brain tissue. For the ROIs of the corpus callosum, a circular-shaped ROI with a diameter of 5 mm was manually placed in the corporis callosi splenium on the axial view images of HASTE, TrueFISP, and single-direction DWI sequence datasets. The signal intensities of the corpus callosum and its surrounding normal brain tissue on the same plane were measured continuously by the same operator. Each layer was measured three times before the average value was recorded.
The Intraclass correlation coefficient (ICC) was used to assess interobserver variability. The image scores and CR in the HASTE, TrueFISP, and single-direction DWI protocols were compared using one-way ANOVA analysis (normal distributed data) and the Kruskal-Wallis and Mann-Whitney U tests (skew distributed data). The diagnostic accuracy of the three sequences among the 26 cases for corpus callosum lesions with follow-up results was calculated and compared using Fisher's exact test.
Results
Interobserver agreement for the optimal visibility of the corpus callosum for the three sequences showed favorable consistency: HASTE (ICC = 0.80), TrueFISP (ICC = 0.84), and single-direction DWI (ICC = 0.90). Single-direction DWI (3.7 ± 0.1, 3.8 ± 0.1) scored significantly higher compared with HASTE (2.9 ± 0.2, 3.0 ± 0.2) and TrueFISP (2.9 ± 0.1, 2.9 ± 0.2) (both p < 0.05).
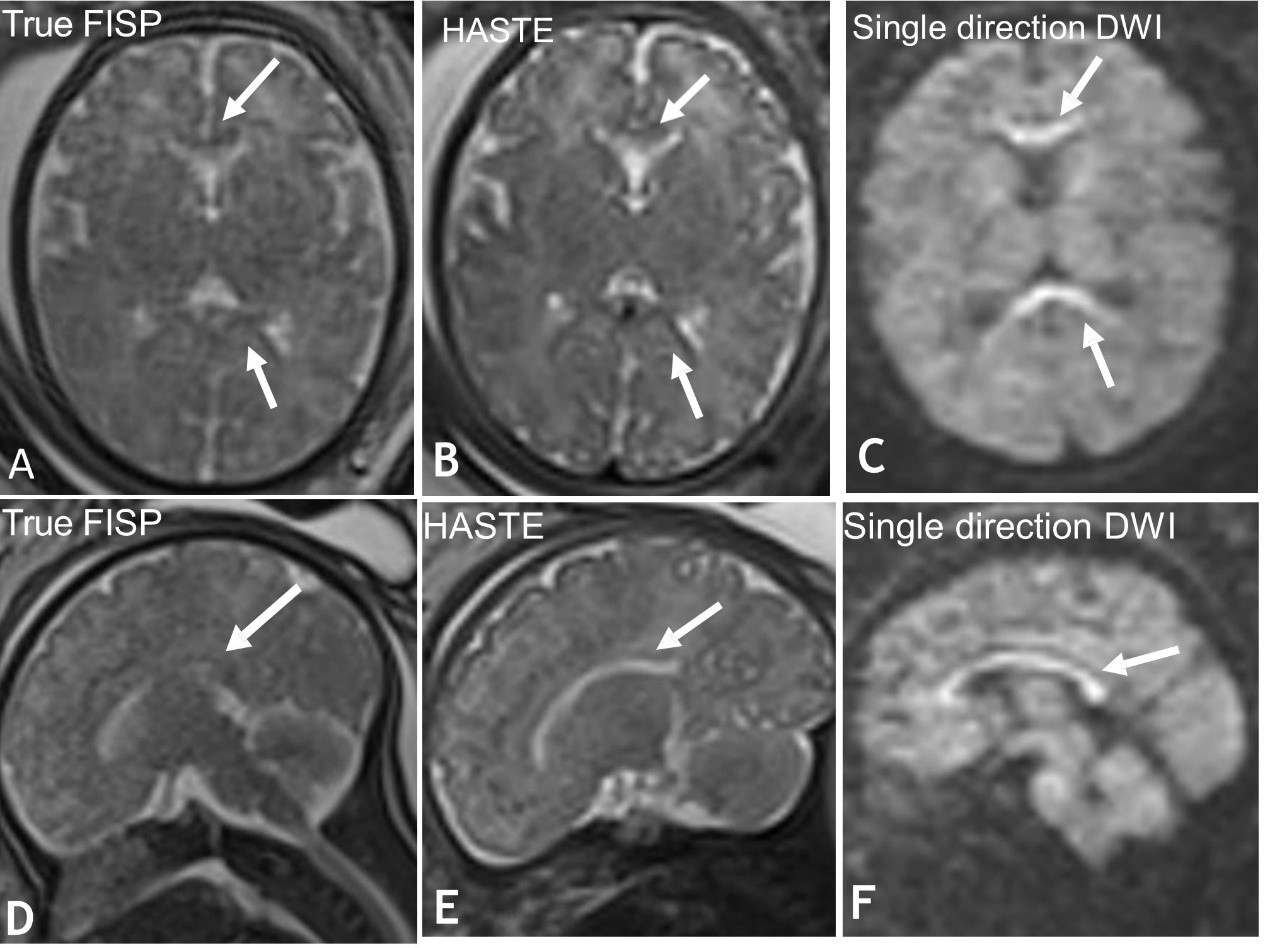
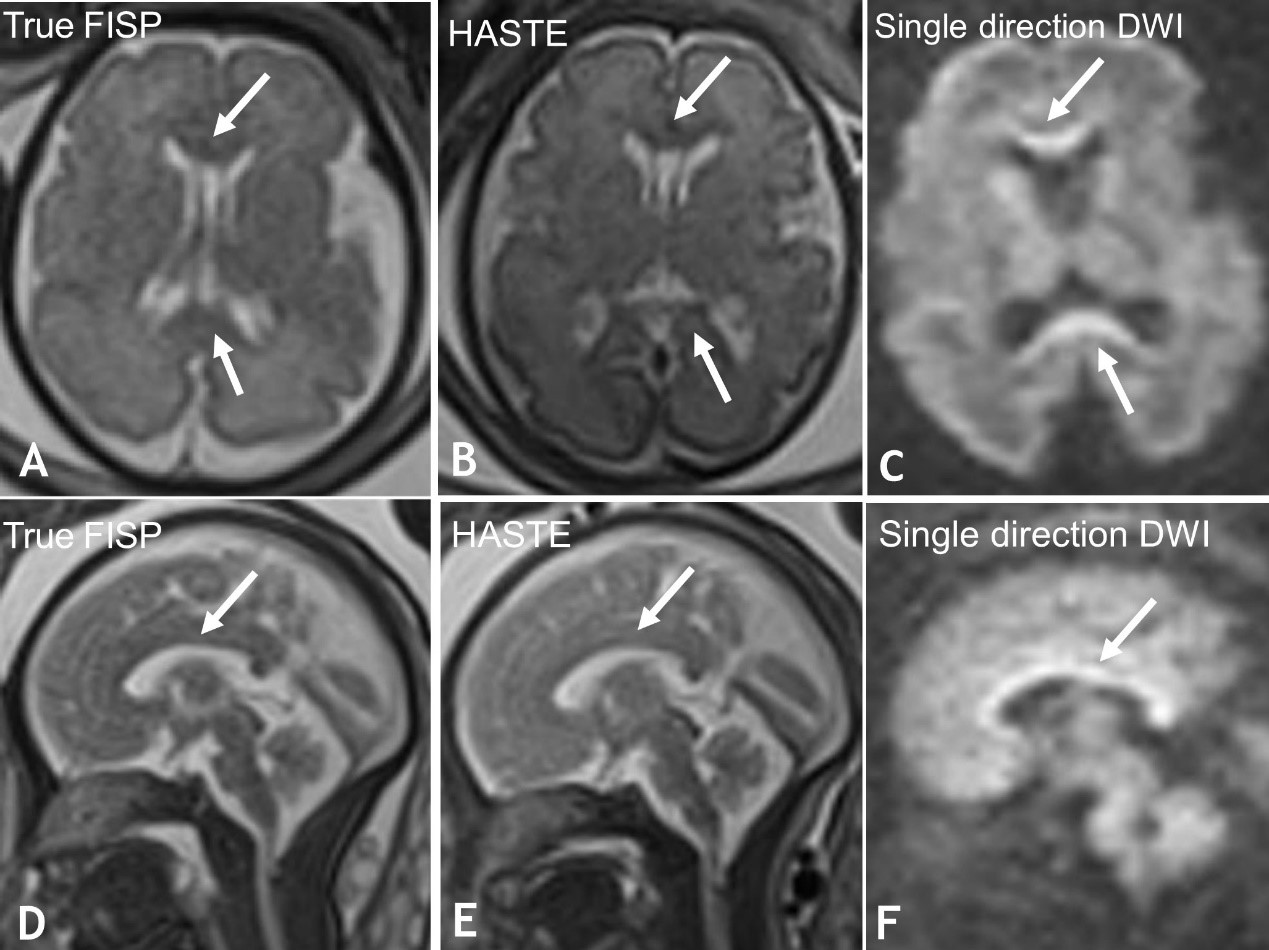
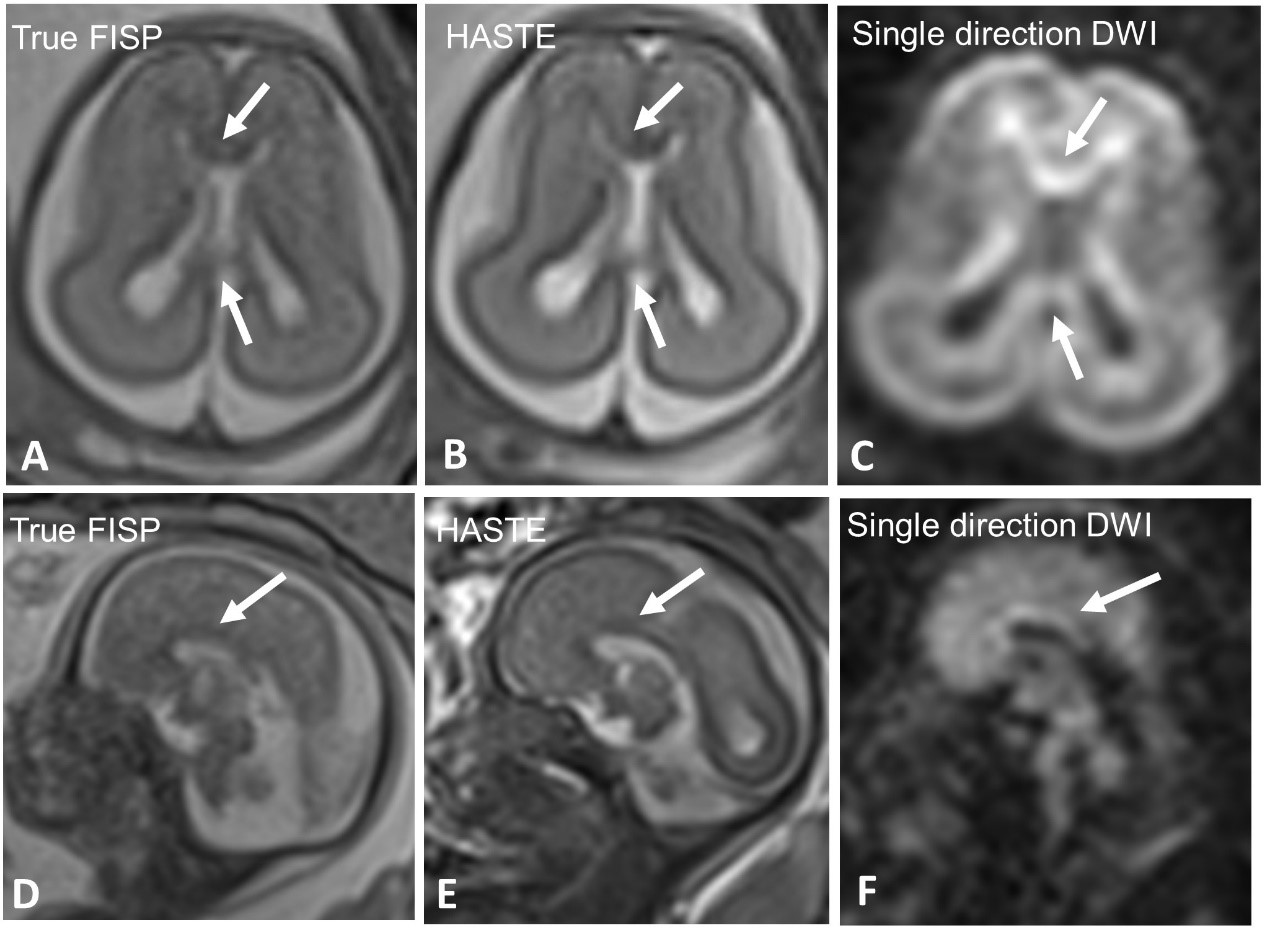
Single-direction DWI presented with the highest CR (p < 0.05) (Fig. 1-2). The CR of HASTE, TrueFISP, and single-direction DWI were 0.146 ± 0.038,0.134 ± 0.032, and 0.307 ± 0.031, respectively .
Among the 26 fetuses with suspected corpus callosum dysplasia identified by follow-up MRI postnatally (Fig. 3), the diagnostic accuracy of single-direction DWI, TrueFISP, and HASTE was 96.15% (25/26), 73.07% (19/26), and 69.23% (18/26), respectively. The diagnostic accuracy of single direction DWI was higher compared to TrueFISP and HASTE (p = 0.038, 0.009).
Discussion and Conclusion
The qualitative and quantitative evaluation of the fetal corpus callosum using optimal visibility scores and the CR proves that the single-direction DWI technique may serve as a useful tool for the diagnosis of fetal agenesis of the corpus callosum. Our results indicated that single-direction DWI provides superior image quality to conventional HASTE and TrueFISP for the fetal corpus callosum.Furthermore, its ability to find corpus callosum dysplasia is also superior to the traditional sequences. In conclusion, this study indicated that single-direction DWI is useful for imaging the fetal corpus callosum and can be used for routine clinical examination.Acknowledgements
No acknowledgement found.References
[1] Manevich-Mazor M,Weissmann-Brenner A,Bar Yosef O, et al. Added Value of Fetal MRI in the Evaluation of Fetal Anomalies of the Corpus Callosum: A Retrospective Analysis of 78 Cases[J]. Ultraschall Med.2018 39(5):513-525
[2] Mürtz P, Krautmacher C, Träber F, et al. Diffusion-weighted whole-body MR imaging with background body signal suppression: a feasibility study at 3.0 Tesla[J]. European Radiology,2007,17(12):3031-3037.
[3] Bydder GM 1, Rutherford MA, Hajnal JV. How to perform diffusion-weighted imaging[J]. Childs Nerv Syst. 2001 Apr;17(4-5):195-201.
[4] Tagliafico A, Succio G, Neumaier CE, et al. Brachial plexus assessment with three-dimensional isotropic resolution fast spin echo MRI: comparison with conventional MRI at 3.0 T[J]. Br J Radiol,2012,85(1014):e110-e116.
[5] Yoneyama M, Takahara T, Kwee T C, et al. Rapid High Resolution MR Neurography with a Diffusion-weighted Pre-pulse[J]. Magnetic Resonance in Medical Sciences,2013,12(2):111-119.
Figures