0620
Cerebrovascular reactivity (CVR) as a potential biomarker in vascular cognitive impairment: relationship with cognition, clinical diagnosis, amyloid and tau proteins.1Department of Radiology, Johns Hopkins University, Baltimore, MD, United States, 2Department of Medicine, Johns Hopkins University, Baltimore, MD, United States, 3Department of Psychiatry, Johns Hopkins University, Baltimore, MD, United States, 4Department of Neurology, Johns Hopkins University, Baltimore, MD, United States, 5Department of Oncology, Johns Hopkins University, Baltimore, MD, United States, 6F.M. Kirby Research Center for Functional Brain Imaging, Kennedy Krieger Institute, Baltimore, MD, United States, 7Department of Neurosurgery, Johns Hopkins University, Baltimore, MD, United States
Synopsis
Is whole brain cerebrovascular reactivity (CVR) associated with cognitive function in subjects with cognitive impairment and normal cognition? In a cross-sectional study of 72 subjects, whole brain CVR as assessed with the BOLD response to a CO2 breathing challenge, was significantly associated with measures of cognitive function. These relationships remained after adjusting for cerebrospinal fluid biomarkers of Alzheimer’s disease pathology and measures of vascular risk. These findings suggest that whole brain CVR may be useful as a biomarker for assessing altered cognition resulting from vascular dysfunction separate from Alzheimer’s disease.
INTRODUCTION
Vascular dementia is the second leading cause of cognitive impairment1,2. However, compared to Alzheimers-type dementia for which a number of biomarkers, e.g. amyloid, tau, glucose hypometabolism, and hippocampal volume, have been established, few biomarkers are available for the diagnosis, stratification, and treatment monitoring of vascular-related dementia3,4. White matter hyperintensities (WMH) in FLAIR MRI are thought to be an indicator of vascular pathology5,6. However, WMH load only correlates modestly with cognitive performance and revealed limited value in clinical diagnosis7. This study sought to investigate the potential of a novel physiological imaging technique, cerebrovascular reactivity (CVR) MRI, as a biomarker in vascular cognitive impairment and dementia by examining its relationship with cognition, clinical diagnosis, amyloid and tau proteins.METHODS
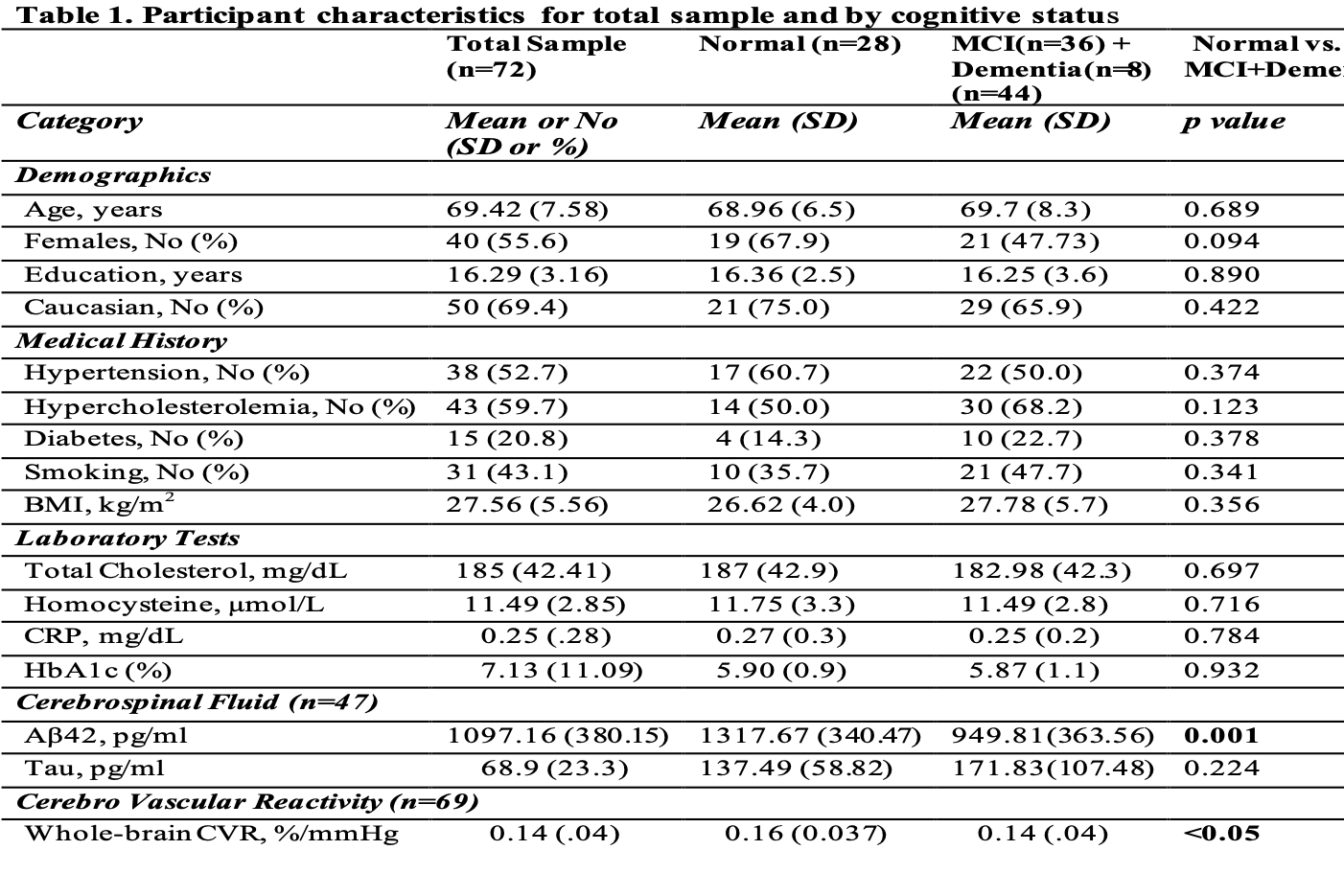
Participants: 72 participants (age 69±8yrs, 56% women) enriched in vascular risk factors (diabetes, hypertension, hypercholesterolemia) were recruited. Among them, 25 were cognitively normal, 36 were mild cognitive impairment (MCI) patients, and 8 were dementia patients. Table 1 summarizes demographic information of the participants.
MRI Procedures: CVR MRI measures the brain blood vessel’s vasodilatory capacity. It is assessed by interleaved inhalation of room-air and CO2-enriched air (5% CO2, 21% O2, 74% N2) while continuously acquiring BOLD MRI images for 7 minutes8. End-tidal (ET) CO2 and breathing rate were recorded using capnography. CVR maps were calculated using a general linear model with BOLD images as the dependent variable and EtCO2 time course as a regressor. The present study primarily focused on whole-brain-averaged CVR (in %ΔBOLD/mmHg of EtCO2), since vascular dementia is a whole-brain disease.
T2 Fluid-Attenuated-Inversion-Recovery (FLAIR) images were collected and they were reviewed by a board-certified neuroradiologist to obtain a Fazekas score as an assessment of WMH burden.
Cognitive and Physical performance: Global cognition was determined using the Montreal Cognitive Assessment, MOCA9. Four cognitive domains were generated by averaging z scores for relevant neuropsychological tests: (1) Verbal episodic memory, (2) Executive function, (3) Processing speed, and (4) Language.
Gait speed(m/s) was measured for a self-paced 4-meter walk10,11.
Labs and CSF measurements: Cerebrospinal fluid (CSF) was collected via lumbar puncture in a subset of participants (n=47), and analyzed for AD-biomarkers, Abeta42 and Tau. Four blood tests were performed to assess vascular risk: hemoglobin A1c(HbA1c), homocysteine, C-reactive protein(CRP), and total cholesterol.
Vascular Risk Score: A composite vascular risk score was calculated as a sum of five medical history elements: hypertension (1=recent,0=remote/absent), hypercholesterolemia (1=recent,0=remote/absent), diabetes (1=recent, 0=remote/absent), smoking (1≥100 cigarettes-smoked,0=if not), and body mass index (1≥ 30,0<30).
Statistical Analysis: Group differences in continuous variables were assessed by t-tests. Linear regression models were performed to test the associations between whole-brain CVR and measures of cognition, physical performance, amyloid and tau.
RESULTS AND DISCUSSION
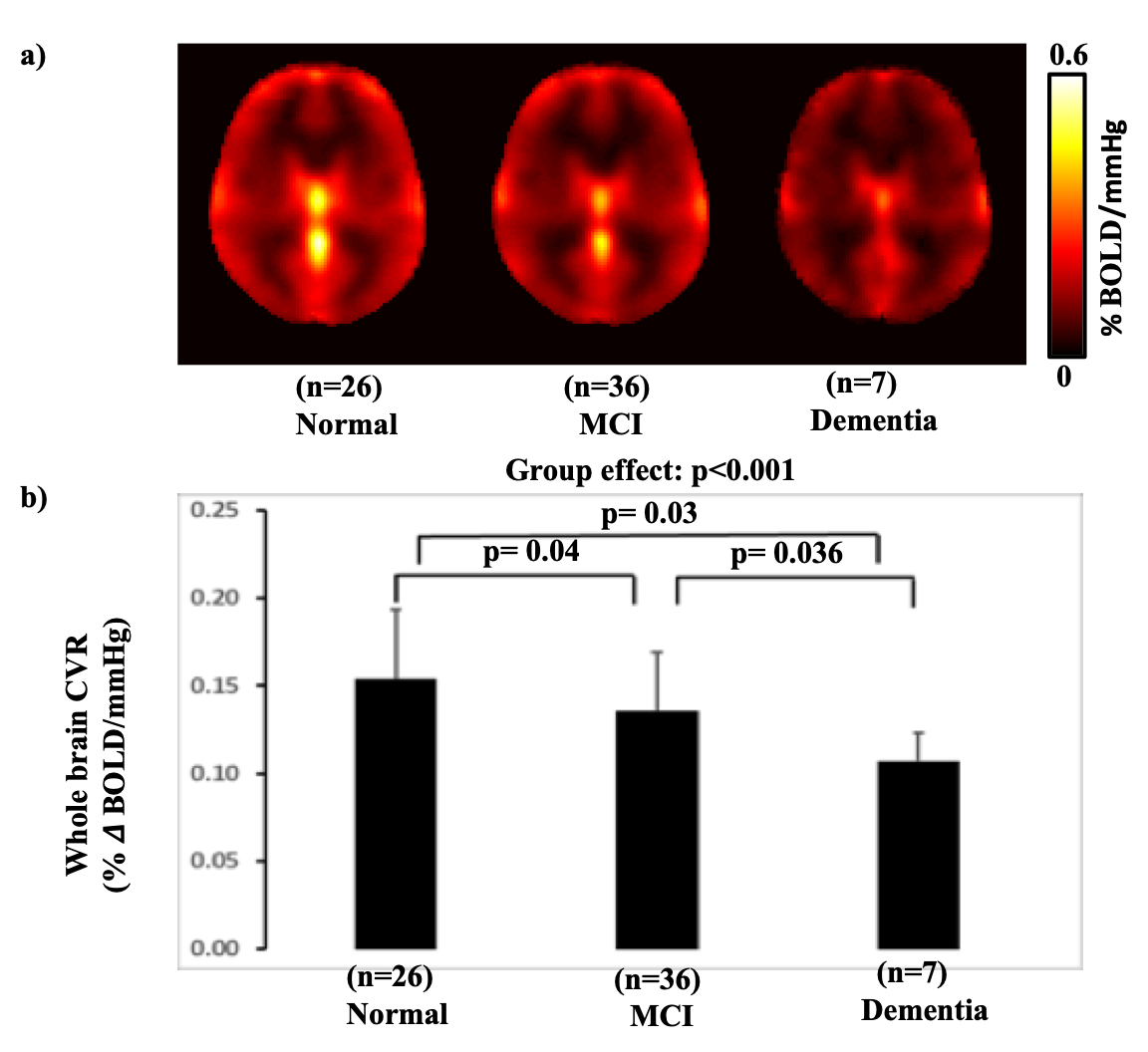
Figure 1a shows averaged CVR maps in normal, MCI, and dementia participants. Figure 1b shows whole-brain CVR values across these diagnosis groups. A significant decline (p<0.001) in CVR can be seen. There was also a significant difference (p<0.05) between each pair of the groups.
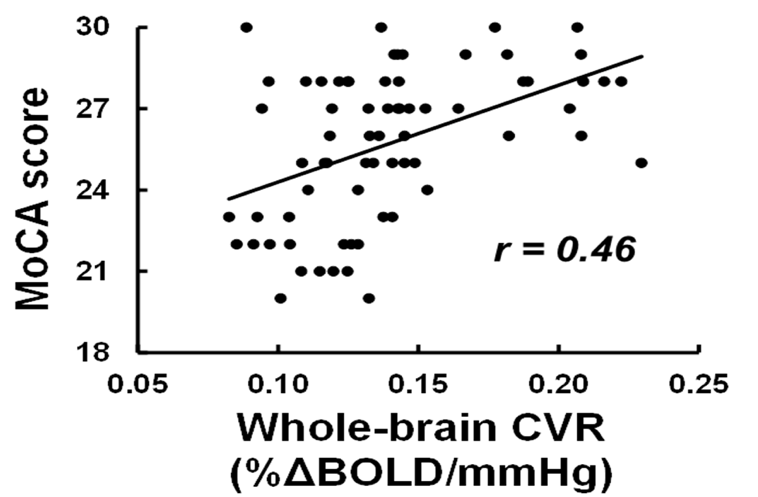
Next, we examined associations between CVR and cognition, after adjusting for age, gender and education. As shown in Figure 2, higher whole brain CVR was significantly associated with better performance on general cognitive function as determined by MOCA (p<0.001). We further examined the associations between CVR and specific cognitive domains. Higher CVR was significantly associated with better performance on executive function(p<0.05) and language(p<0.05), but not with episodic memory(p=.16) and processing speed(p=.45).
To examine whether CVR can explain variations in cognition above and beyond AD pathology, we added AD pathological biomarkers, CSFAβ42 and tau. CVR remained associated with MOCA scores after controlling for Aβ42 and Tau (p<0.005).
The analysis was repeated in participants with cognitive impairments (MCI+dementia). CVR remained significantly associated with MOCA (p<.01), however, the associations between CVR and specific cognitive domains were no longer significant.
Next, we examined the association between CVR and physical performance (Gait speed). Higher CVR was significantly associated with faster gait (p< 0.05), after adjusting for age and gender.
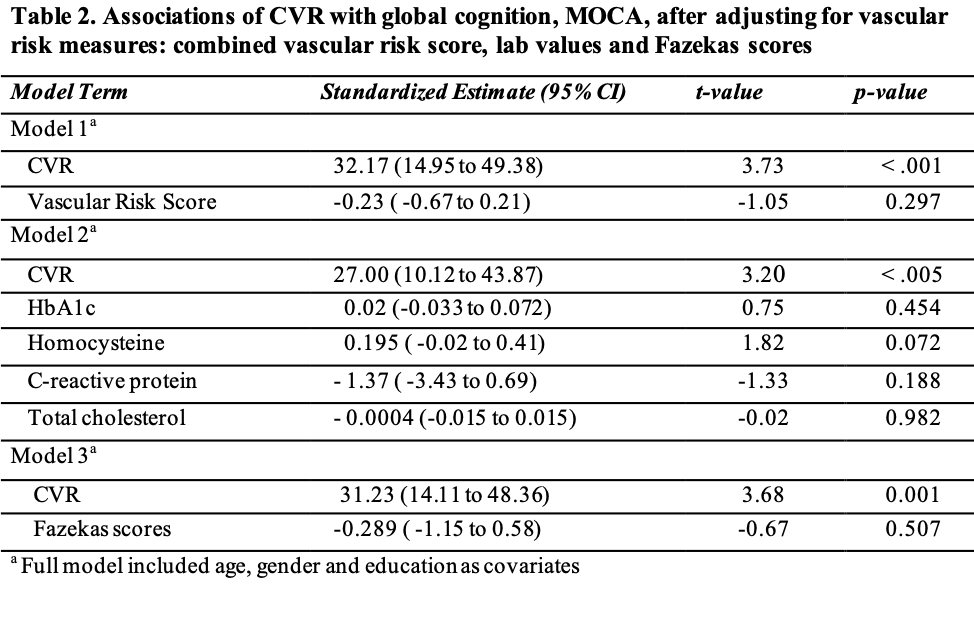
We also examined the association between CVR and vascular risks. CVR was not significantly associated with vascular risk scores or Fazekas scores. However, the association between CVR and MOCA score remained significant after controlling for vascular risk scores and Fazekas scores (p<0.005) (Table 2).
CONCLUSION
CVR was able to differentiate cognitively normal subjects, MCI patients, and dementia patients in a group of individuals with mixed AD and vascular pathology. CVR can independently predict cognitive function above and beyond traditional AD pathological biomarkers (i.e. after controlling for Aβ42 and Tau), suggesting that CVR may be a useful biomarker for evaluating cognitive impairment related to vascular pathology in older individuals.Acknowledgements
No acknowledgement found.References
1. Schneider JA, Arvanitakis Z, Bang W, Bennett DA. Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Neurology. 2007;69(24):2197-2204.
2. Schneider JA, Arvanitakis Z, Leurgans SE, Bennett DA. The neuropathology of probable Alzheimer disease and mild cognitive impairment. Ann Neurol. 2009;66(2):200-208.
3. Weiner MW, Veitch DP, Aisen PS, et al. Impact of the Alzheimer’s Disease Neuroimaging Initiative, 2004 to 2014. Alzheimer’s Dement. 2015;11(7):865-884.
4. Montagne A, Nation DA, Pa J, Sweeney MD, Toga AW, Zlokovic B V. Brain imaging of neurovascular dysfunction in Alzheimer’s disease. Acta Neuropathol. 2016;131(5):687-707.
5. Duering M, Zieren N, Hervé D, et al. Strategic role of frontal white matter tracts in vascular cognitive impairment: A voxel-based lesion-symptom mapping study in CADASIL. Brain. 2011;134(8):2366-2375.
6. Wardlaw JM, Smith C, Dichgans M. Mechanisms of sporadic cerebral small vessel disease: Insights from neuroimaging. Lancet Neurol. 2013;12(5):483-497.
7. Knopman DS, Griswold ME, Lirette ST, et al. Vascular Imaging abnormalities and cognition: Mediation by cortical volume in nondemented individuals: Atherosclerosis risk in communities-neurocognitive study. Stroke. 2015;46(2):433-440.
8. Lu H, Xu F, Rodrigue KM, et al. Alterations in cerebral metabolic rate and blood supply across the adult lifespan. Cereb Cortex. 2011;21(6):1426-1434.
9. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695-699.
10. Guralnik JM, Simonsick EM, Ferrucci L, et al. A Short Physical Performance Battery Assessing Lower Extremity Function: Association with Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J Gerontol. 1994;49(2):M85-M94.
11. Bohannon RW. Comfortable and maximum walking speed of adults aged 20-79 years: Reference values and determinants. Age Ageing. 1997;26(1):15-19.
Figures