0619
Predicting Progression from Mild Cognitive Impairment to Alzheimer’s Disease1The Mind Research Network, Albuquerque, NM, United States
Synopsis
This exploratory analysis tests the suitability of deep residual networks to learn neuroanatomical abnormalities from the structural MRI (sMRI) modality, and utility of dynamic (i.e. time-varying) functional connectivity approaches in delineating discriminative functional MRI (fMRI) features to predict progression of individuals with mild cognitive impairment to Alzheimer’s disease. Results demonstrate better than state-of-the-art prediction performance using the structural MRI modality alone. Multimodal prediction performed significantly better than unimodal sMRI or fMRI predictions, thus corroborating the benefits of predicting in the augmented space. Results also corroborate the diagnostic utility of the sMRI and fMRI features used to make the predictions.
Introduction
Alzheimer’s disease (AD) is an irreversible, progressive dementia that demands early diagnosis and therapeutic intervention, while mild cognitive impairment (MCI) is an intermediate condition between typical age-related cognitive deterioration and dementia. MCI individuals can progress to some form of dementia (not necessarily AD); however, in absence of a narrower prodrome for AD, MCI is often used as a prodromal stage of AD to predict and characterize progression to AD. This work focuses on predicting progression of MCI to AD by evaluating the structural MRI (sMRI) and functional MRI (fMRI) data of the cognitively normal (CN), MCI and AD elderly populations. More specifically, the aim of this work is to predict the subset of MCI individuals who would progress to AD within a period of three years (progressive MCI or pMCI) and the other subset of MCI individuals that do not progress to AD within this period (stable MCI or sMCI).Methods
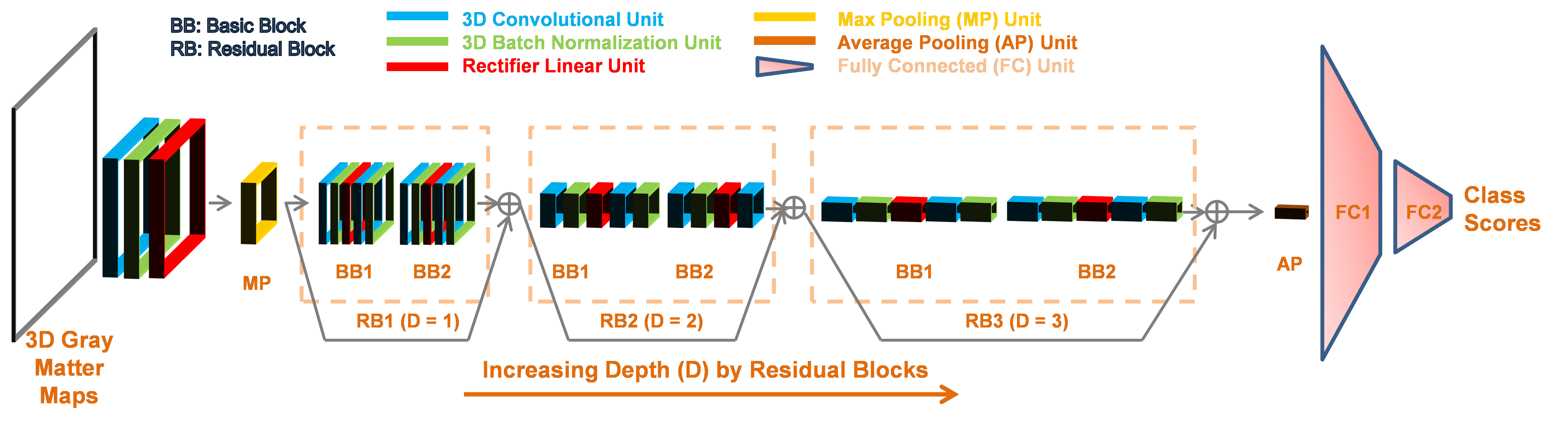
The first part of this work tests the suitability of a deep residual
network1 (Figure 1) to learn
neuroanatomical abnormalities in the gray matter volume (GMV) estimated from
ADNI sMRI data (n = 828; CN: 237, sMCI: 245, pMCI: 189 and AD: 157). We test this network using a rigorous, repeated (n =
10) k-fold (k = 5) cross-validation procedure, where we first estimate the predictive
(diagnostic/prognostic classification) power by training and testing on the
MCI population only, followed by use of domain transfer learning (DTL) approach
to perform network training additionally on the CN and AD groups. The second part of this work proposes a novel,
multimodal (sMRI-fMRI) data fusion framework to predict progression of MCI to
AD. This part featured unimodal (separate sMRI and fMRI) as well as
multimodal prediction analyses on a smaller subset of subjects of the earlier
used dataset for which both modalities were available (n = 132; CN: 34, sMCI: 36, pMCI:
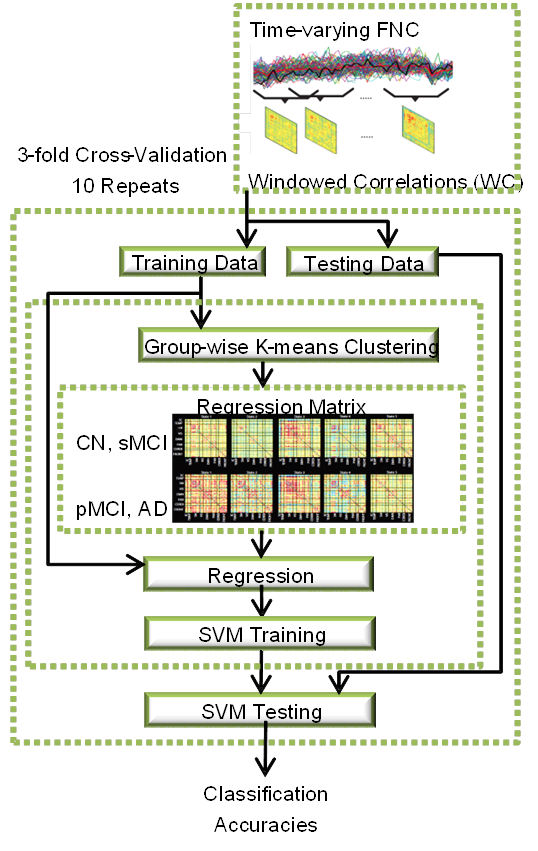
24 and AD: 38). For the fMRI modality, features based on dynamic (i.e.
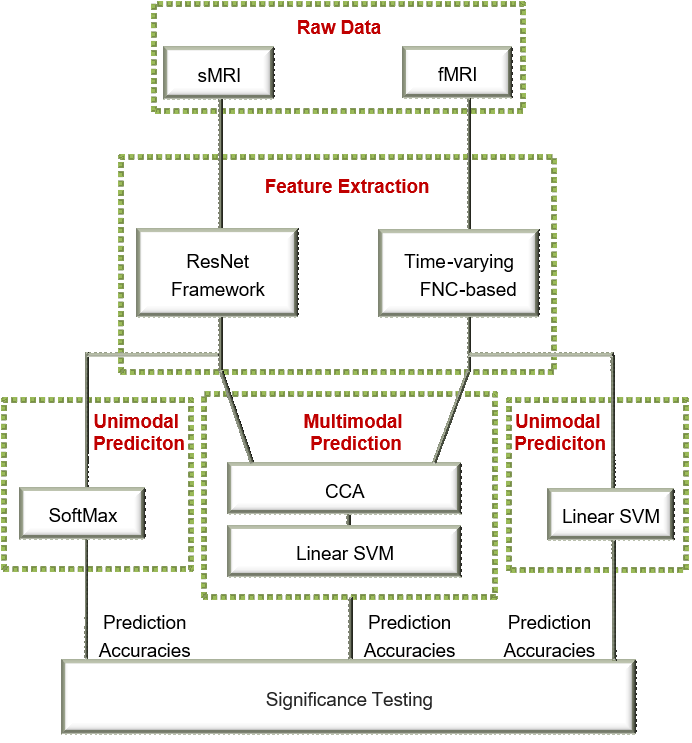
time-varying) functional network connectivity (dFNC) were estimated (Figure 2) using a previously proposed method 2. The estimated sMRI and fMRI features were fused
using canonical correlation analysis (CCA) in the multimodal prediction analysis
(Figure 3). All three prediction analyses were performed using
a rigorous stratified, repeated (n = 10) k-fold (k = 3) cross-validation
procedure on the same training and test folds, following which a three-way
performance comparison was conducted.
Results
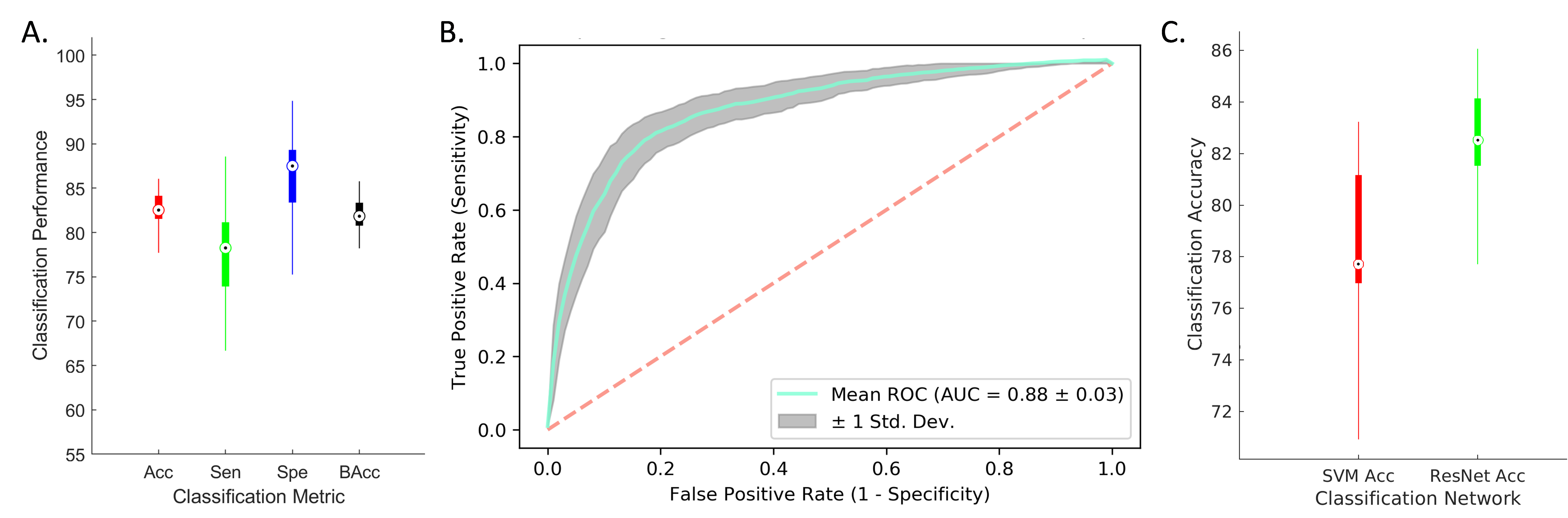
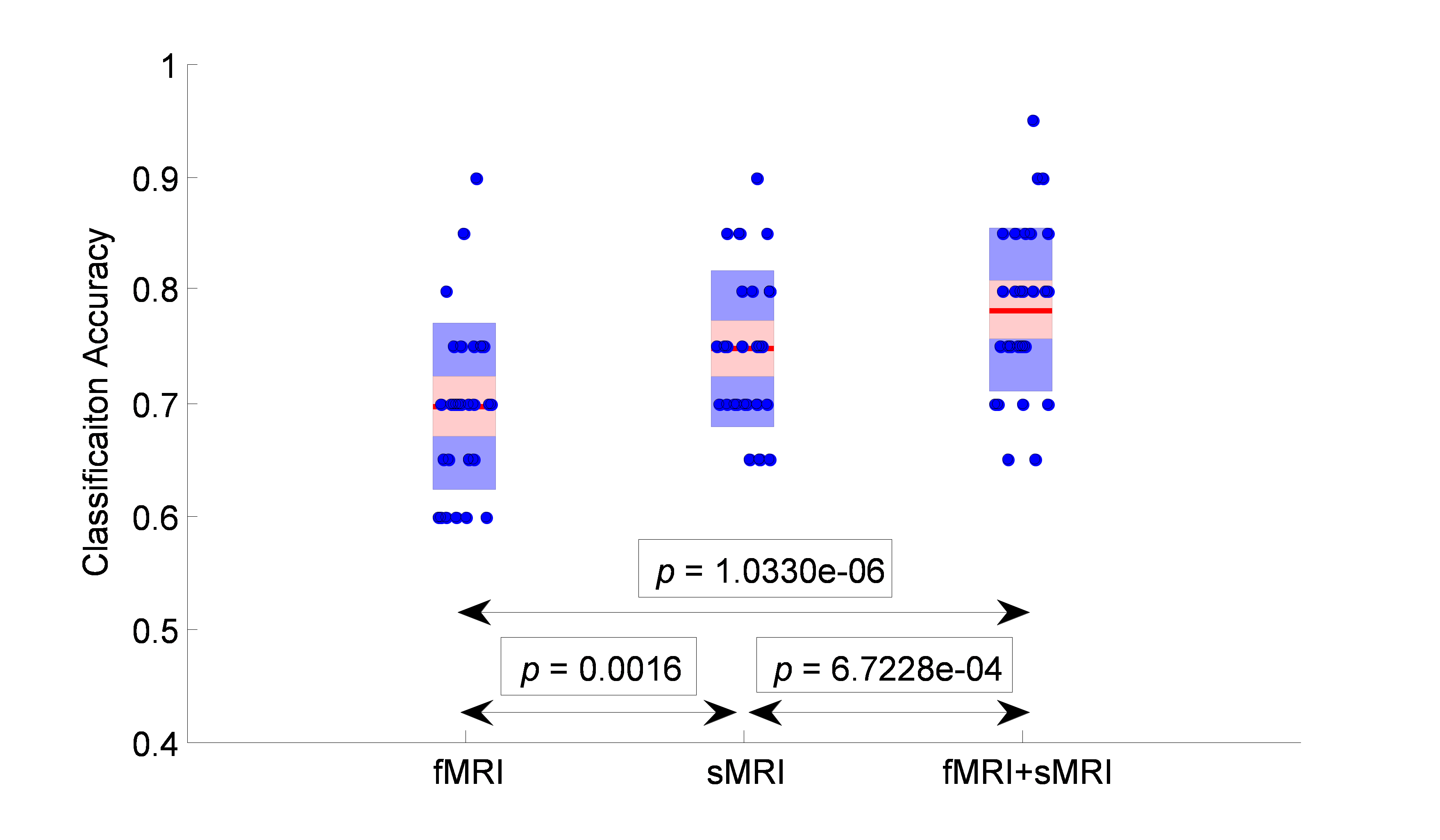
In the first part of this work, our initial sMRI (n = 828) prediction analysis on the MCI group alone achieved a prediction accuracy of 77.2%, which was further enhanced in the DTL case to 82.7% (Figure 4). The DTL case performed significantly better than a classical SVM classifier (p = 2.57e-8). Additionally, both of these reported accuracies are a significant improvement over the state-of-the-art performance (75.44% as reported in 3) in making similar predictions using the sMRI modality alone. Next, in the second part of this work on the smaller multimodal data (n=132), the fMRI, sMRI and the multimodal prediction analyses resulted in cross-validated prediction accuracies of 70%, 75% and 78% respectively (Figure 5). Significant improvement was observed with multimodal prediction as compared to the unimodal fMRI (p = 1.0330e-6) and sMRI prediction analyses (p = 6.72e-4). Additionally, the prediction with sMRI features was found to be significantly better than that from the fMRI features (p = 0.0016).Discussion
A significant improvement in the cross-validated prediction accuracy from the augmented (i.e. fused) feature space over those from the separate sMRI and fMRI feature spaces corroborates the presence of complimentary diagnostic information available in both modalities and validates the benefits of making such predictions in the augmented space. Results also evince that deep learning networks can be considered well-suited and further explored to evaluate neuroanatomical aberrations from the sMRI data, whereas dFNC approaches could be undertaken to capture diagnostic biomarkers from the fMRI data.Conclusion and Future Work
Our results highlight the possibility of early identification of modifiable risk factors for understanding progression to AD using similar advanced deep learning and dFNC based frameworks. Such delineation is significant for early identification of individuals with high disease risk, who could also be reliably recruited for testing preventive treatments of AD. While, in this work, we train the two modalities separately and fuse their resultant feature spaces, future work would target development of a deep learning network that enables end-to-end training in both modalities in a parallel fashion for better optimization of the network’s weights, a feature that is highly likely to enhance the prediction performance.Acknowledgements
This work was supported by NIH grant numbers 2R01EB005846, P20GM103472, P30GM122734, and R01REB020407 as well as NSF grant 1539067 to Dr. Vince D. Calhoun.References
1. He, K., Zhang, X., Ren, S. & Sun, J. in 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR) 770-778 (2016).
2. Rashid, B. et al. Classification of schizophrenia and bipolar patients using static and dynamic resting-state fMRI brain connectivity. NeuroImage 134, 645-657, doi:10.1016/j.neuroimage.2016.04.051 (2016).
3. Lu, D., Popuri, K., Ding, G. W., Balachandar, R. & Beg, M. F. Multimodal and Multiscale Deep Neural Networks for the Early Diagnosis of Alzheimer’s Disease using structural MR and FDG-PET images. Scientific Reports 8, 5697, doi:10.1038/s41598-018-22871-z (2018).
Figures