0606
3D Multitasking for Non-ECG, Free-Breathing, Simultaneous Cardiac Motion-Resolved T1 Mapping and Function Evaluation1Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 2Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 3Siemens Healthineers, Los Angeles, CA, United States, 4Department of Bioengineering, UCLA, Los Angeles, CA, United States
Synopsis
Myocardial T1 mapping characterizes focal and diffuse fibrosis. We have recently shown cardiac motion-resolved 2D T1 maps with free breathing and without ECG, greatly simplifying workflow. In this study, we extend this approach to 3D and redesign the acquisition to improve spatial resolution and sampling efficiency compared to 2D. We also show the feasibility of assessing function from the same cardiac-resolved 3D Multitasking scan used for T1 mapping. T1 maps were compared to 2D MOLLI and function was compared to a breath-hold cine sequence.
Introduction
Myocardial T1 mapping can characterize both focal and diffuse myocardial fibrosis, important factors often linked with adverse events.[1] Whole-heart coverage is necessary to fully characterize the myocardial tissue[2]; however, since typical T1 mapping methods require a breath-hold per slice, this can be exhausting or unreliable for patients. Recently, interest has increased in T1 mapping during systole in addition to diastole [3,4] to potentially ease analysis due to the thicker myocardium and provide more information; but it typically requires an additional breath-hold per slice. Cine images, used to assess function, are included in a cardiac MRI scan at the cost of another breath-hold per slice. An alternative approach, Multitasking, can produce accurate and repeatable cardiac motion-resolved 2D T1 maps with free breathing and without ECG, greatly simplifying workflow with an easy setup.[5,6] In this study we extend this approach to 3D and redesign the acquisition to improve spatial resolution and sampling efficiency compared to 2D. We will also show the feasibility of assessing function from the same cardiac-resolved 3D Multitasking scan used for T1 mapping.Methods
The proposed sequence uses a prototype 3D stack-of-stars trajectory modified to collect image data readouts incremented by the golden-angle with Gaussian random partition encoding, while every 8th readout is auxiliary data (0° trajectories at the center partition). The continuous acquisition sequence applies inversion recovery pulses at set intervals to achieve T1 recovery and collects small-angle FLASH readouts to sample the entire T1 recovery period. Sequence parameters were: fixed scan time of 9:19 min, 2.5s between IRs, TE/TR = 1.6/3.5ms, flip angle = 5°, 16 slices, slice thickness = 8 mm, in-plane resolution = 1.4x1.4 mm2.
Note that the original 2D multitasking implementation acquired auxiliary data every other readout; by switching to every 8 readouts here, we can measure 7 imaging lines where 2D multitasking measured only 4. This change improves the efficiency of image data collection by 75%, which we have used to tradeoff higher in-plane spatial resolution (1.4x1.4 mm2 compared to 1.7x1.7 mm2).
Similar to 2D Multitasking, real-time low-rank matrix images were reconstructed from the image data and auxiliary data for use in cardiac and respiratory motion binning.[5] Next, low-rank tensor reconstruction was performed using an explicit tensor subspace constraint estimated from the auxiliary data and a dictionary of Bloch equation T1 curves to produce 700 inversion time (TI) images (range: 3.5-2,450 ms, 3.5 ms temporal resolution) with 20 cardiac and 6 respiratory phases for a total of 84,000 3D images. T1 values were estimated by pixel-wise fitting to a FLASH-IR model at an end-expiration respiratory and both diastolic and systolic cardiac phases.
Eight asymptomatic subjects (3 female, age 39±16) were scanned at 3T (Siemens Biograph mMR) with 3D Multitasking T1 mapping and a resolution-matched, breath-hold, ECG-gated, 2D MOLLI. For both methods, T1 was measured with an ROI in the septum. Diastolic T1 values from both methods were compared using a paired t-test.
Multitasking T1 mapping can also assess cardiac function because of the cardiac phase information it images. In one subject, we compared end-diastolic volume, end-systolic volume, stroke volume, and ejection fraction to a breath-hold, ECG-gated, multi-slice cine sequence. Cine sequence parameters were: scan time = 14 heartbeats for each slice, flip angle = 35°, slice thickness = 8 mm, in-plane resolution 1.4 x 1.4 mm2. For function measurements with Multitasking, 1 out of 700 TIs was chosen that provided good contrast between the myocardium and blood pool. For both methods, the endocardium was segmented in end-diastole and end-systole to calculate stroke volume and ejection fraction.
Results and Discussion
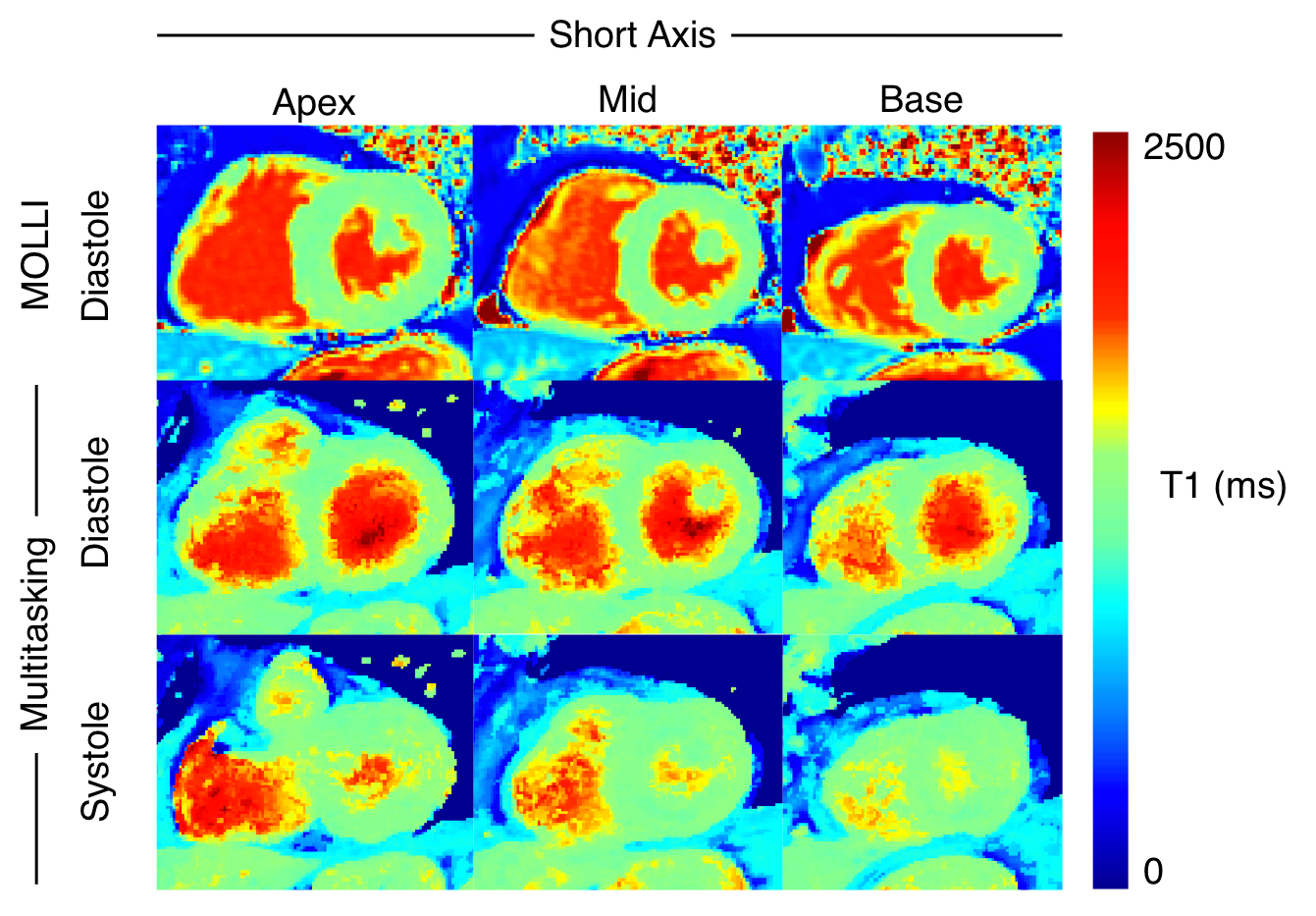
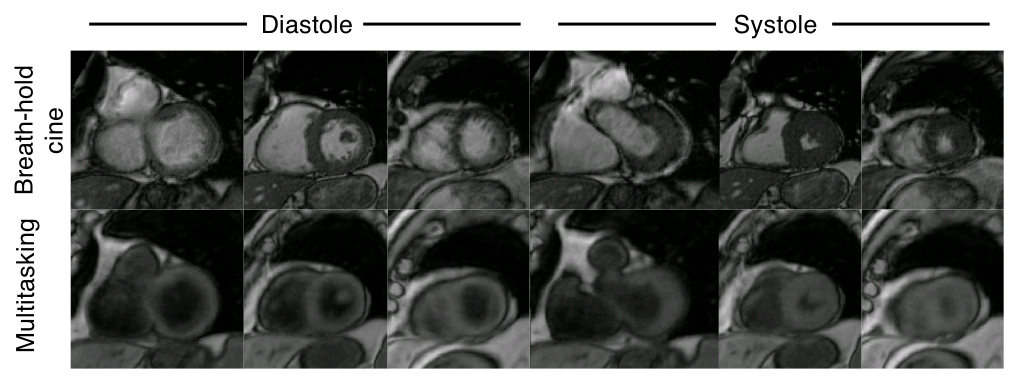
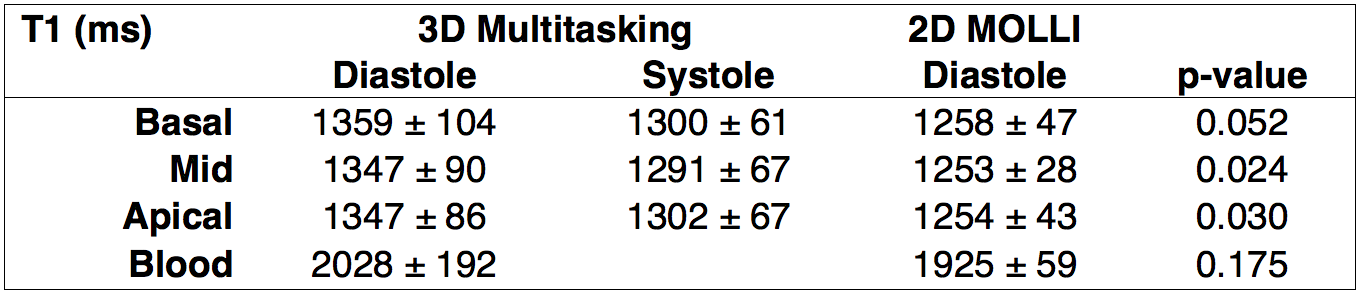
Systolic and diastolic T1 maps from one subject are shown in Figure 1 for 3D Multitasking T1 mapping and 2D MOLLI. Basal, mid, and apical T1 values in 3 out of 16 slices averaged for all subjects for Multitasking 3D T1 mapping and MOLLI are shown in Table 1. Systolic T1 values measured with 3D Multitasking T1 mapping are lower than diastolic T1 values, consistent with recent studies.[3,4,7] Diastolic T1 values measured with Multitasking are higher compared to MOLLI diastolic T1 values. The bias between methods may be due to sequence differences (FLASH vs SSFP) and myocardial blood inflow differences stemming from the excitation (continuous 3D excitation versus less-frequent slice-selective 2D excitation); MOLLI has also been shown to underestimate T1 values. Diastolic and systolic cine images from breath-hold cine scans and 3D Multitasking are shown in Figure 2. Function measurements from one subject are shown in Table 2, demonstrating similar volume measurements.Conclusion
We demonstrate simultaneous T1 mapping and function evaluation using a whole-heart 3D free-breathing, non-ECG, Multitasking technique. Our redesign of the sampling pattern allowed imaging data to be acquired 75% more efficiently than previous Multitasking techniques.Acknowledgements
This work was supported by NIH 1R01HL124649 and NIH T32HL116273.References
1. Puntmann et al. Circ Res. 2016;119(2). 2. Messroghli et al. JCMR 2017;19:75. 3. Messner et al. Sci Reports 2018;8(5251). 4. Zhao et al. JCMR 2016;18(13). 5. Christodoulou et al. Nature BME 6. Shaw et al. ISMRM 2016:0039. 7. Kawel et al JCMR 2012;14(27).Figures