0605
Imaging Fetal Congenital Heart Disease Using Motion Compensated Cardiovascular Magnetic Resonance Imaging1Radiology, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 2Translational Medicine, The Hospital for Sick Children, Toronto, ON, Canada, 3Medical Biophysics, University of Toronto, Toronto, ON, Canada, 4Pediatric Cardiology, The Hospital for Sick Children, Toronto, ON, Canada, 5Imaging Sciences and Biomedical Engineering, King's College London, London, United Kingdom, 6Paediatric and Fetal Cardiology, Evelina Children's Hospital, London, United Kingdom, 7Pediatrics and Diagnostic Imaging, University of Toronto, Toronto, ON, Canada
Synopsis
In pregnancies where fetal congenital heart disease is suspected during routine obstetric ultrasound, a thorough echocardiographic workup is required to assess the fetal cardiac anatomy and function. MRI has been increasingly proposed as an adjunct diagnostic tool to evaluate the fetus. In this work, we present a newly developed method for reconstructing high-resolution dynamic MR images of the fetal heart, evaluate this modality in the context of visualizing cardiac abnormalities, and compare to echocardiography. We show that MRI of the fetal heart has the potential to compliment echocardiography in the assessment of congenital heart disease.
Introduction
Congenital heart disease (CHD) is the most common congenital abnormality, affecting nearly 1% of live births each year [1]. If CHD is suspected during routine obstetric ultrasound, a thorough echocardiographic workup is required to assess the fetal cardiac anatomy and function. Recent developments in cardiovascular magnetic resonance imaging (CMR) allow for high resolution imaging of the fetal heart by compensating for the effects of motion and fetal heart rate [2–7]. Here we present our experience applying a novel framework for fetal MRI to subjects with a range of cardiac abnormalities and compare our CMR images to fetal echocardiography [4]. We show that CMR has the potential to compliment echocardiography in the assessment of fetal congenital heart disease.Methods
Twenty-five pregnant volunteers underwent fetal CMR and echocardiography examinations due to suspected CHD. A multi-slice 2D balanced steady state free precession sequence with golden angle radial sampling was prescribed in short-axis and long-axis planes covering the whole fetal heart on a 1.5T clinical MRI system (Avanto Fit, Siemens Healthineers – Germany). All scans were acquired free-breathing with the following parameters: flip angle: 70°, spokes: 3000, TR/TE: 4.95/2.48 ms, samples per spoke: 256, field-of-view: 256 × 256 mm2, spatial resolution: 1 × 1 × 4 mm3, CINE temporal resolution: 12-15 ms, scan time per slice: 15s. Reconstruction of fetal CMR images was performed using a previously published method for retrospective motion correction [4]. A real-time reconstruction was used to assess and reject noticeable through-plane motion, estimate and correct for translational motion, and extract the fetal heart rate. Using these motion parameters, high-resolution CINE images were reconstructed wherein the effects of maternal respiration and fetal movement were suppressed. To provide the closest comparison to CINE CMR, continuous echocardiography 2D sweeps of the fetal cardiac anatomy were acquired in axial and sagittal views covering the fetal heart and great vessels using a Philips iU22 system with a C5-1 abdominal transducer and frequency range of 1-5 MHz (Philips Healthcare − Netherlands). Quantitative comparison between CMR and echocardiography was performed by two independent blinded reviewers using a binary scoring system (1 - identifiable structure, 0 - non-identifiable structure) of nine fetal cardiac features.Results
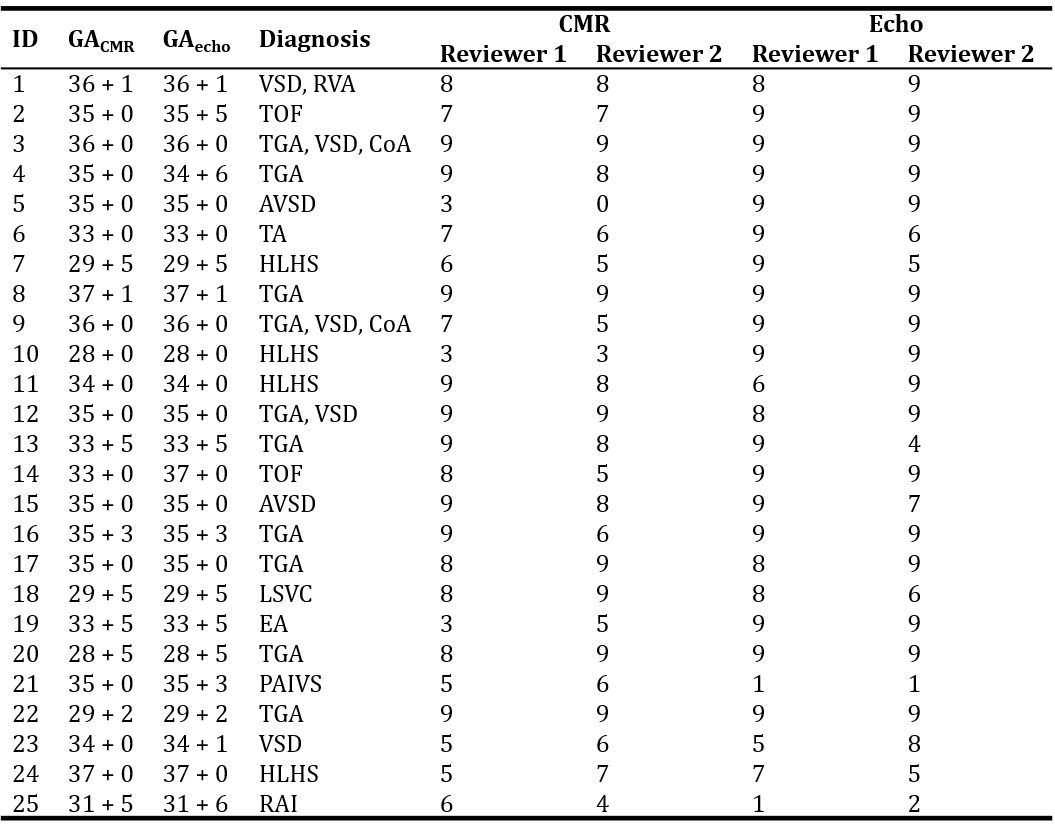
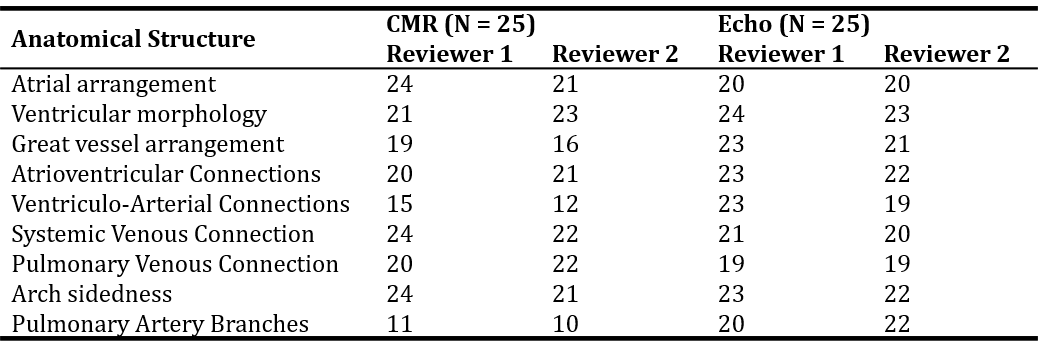
Representative axial and short-axis multi-slice CMR images covering the heart are shown in Figs. 1 and 2 respectively, providing a detailed overview of the segmental analysis performed by two reviewers for each subject and modality. The abnormal arrangement of the great vessels and discordant ventriculo-arterial connections indicate transposition of the great arteries, which was confirmed by postnatal echo and cardiac surgery. Segmental analysis of the fetal cardiac anatomy using CMR and echo is summarized for all twenty-five subjects in Figs. 3 and 4. The average number of anatomical features identified (out of 9) across all subjects was higher for echo (R1: 7.8 ± 2.3, R2: 7.5 ± 2.4) than CMR (R1: 7.1 ± 2.1, R2: 6.7 ± 2.3), while a Wilcoxon sign rank test indicated a statistically significant difference between modalities for both reviewers (R1 p=0.01, R2 p=0.01). Interobserver agreement measured by Cohen’s kappa coefficient was 0.58 for CMR and 0.47 for echo. If we exclude subjects with observed gross fetal movement (N=4), the number of anatomical features observed by CMR (R1: 7.5 ± 1.8, R2: 7.3 ± 1.7) or echo (R1: 7.6 ± 2.5 R2: 7.4 ± 2.5) is no longer statistically different (R1: p=0.72, R2: p=0.88). Furthermore, the number of anatomical features identified by at least one of CMR or echo (R1: 8.4 ± 1.3, R2: 8.4 ± 1.2) was higher than either modality alone. In general, both the CMR and echo images were able to clearly identify the cardiac abnormalities present within the cohort of subjects. Fig. 5 shows an example reconstruction from both modalities wherein the relatively small left ventricle and ascending aorta are in keeping with the postnatal diagnosis of hypoplastic left heart syndrome.Discussion
This work presents the first segmental-analysis-based comparison between motion compensated fetal MRI and echo across a range of congenital heart defects. We show that fetal MRI provides complimentary diagnostic information to echo during late gestation suggesting its utility in cases with poor acoustic windows such as oligohydramnios, maternal obesity and diaphragmatic hernia.Conclusion
CMR is a promising tool for evaluating fetal cardiac anatomy and function. Given adequate coverage of the heart without major fetal movement, fetal CMR provides diagnostic information comparable to echo in late gestation, providing new opportunities to study pregnancies in which the fetal cardiovascular system is abnormal.Acknowledgements
No acknowledgement found.References
1. Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics-2016 update a report from the American Heart Association. Circulation. 2016.
2. Roy CW, Seed M, van Amerom JFP, Al Nafisi B, Grosse-Wortmann L, Yoo S-JJ, et al. Dynamic imaging of the fetal heart using metric optimized gating. Magn Reson Med . 2013;70:1598–607.
3. Roy CW, Seed M, Macgowan CK. Accelerated MRI of the fetal heart using compressed sensing and metric optimized gating. Magn Reson Med . 2016;00:1–11.
4. Roy CW, Seed M, Kingdom JC, Macgowan CK. Motion compensated cine CMR of the fetal heart using radial undersampling and compressed sensing. J Cardiovasc Magn Reson . 2017;19:29. Available from: http://jcmr-online.biomedcentral.com/articles/10.1186/s12968-017-0346-6
5. Chaptinel J, Yerly J, Mivelaz Y, Prsa M, Alamo L, Vial Y, et al. Fetal cardiac cine magnetic resonance imaging in utero. Sci Rep . 2017;7:15540.
6. van Amerom JFP, Lloyd DFA, Price AN, Kuklisova Murgasova M, Aljabar P, Malik SJ, et al. Fetal cardiac cine imaging using highly accelerated dynamic MRI with retrospective motion correction and outlier rejection. Magn Reson Med . 2018;79:327–38.
7. Kording F, Yamamura J, de Sousa MT, Ruprecht C, Hedström E, Aletras AH, et al. Dynamic fetal cardiovascular magnetic resonance imaging using Doppler ultrasound gating. J Cardiovasc Magn Reson. 2018;20:17.
Figures