0604
Multi-shot DWI with multiplexed sensitivity encoding (MUSE) versus single-shot DWI in the breast1Department of Electrical Engineering, Stanford University, Stanford, CA, United States, 2Global MR Application and Workflow, GE Healthcare, Boston, MA, United States, 3Global MR Application and Workflow, GE Healthcare, Menlo Park, CA, United States, 4Department of Radiology, Stanford University, Stanford, CA, United States, 5Department of Bioengineering, Stanford University, Stanford, CA, United States
Synopsis
Diffusion-weighted imaging (DWI) has shown strong potential for clinical impact in breast MRI but is limited by low resolution and image distortion. Multi-shot acquisitions can help to address these limitations. Here we assess a multi-shot diffusion acquisition utilizing two different reconstructions in comparison to single-shot DWI in breast cancer patients. The assessment includes quantified perceived resolution and ratings of qualitative image characteristics with respect to the DCE-MRI acquisition.
Introduction
Diffusion-weighted Imaging (DWI) has been widely investigated in breast MRI and has shown promise for a number of indications including assessing response to treatment[1]. DWI also offers tremendous potential for non-contrast enhanced breast cancer screening protocol[1]. Conventional EPI-based DWI is limited by low resolution and image distortion. Both of these effects are the results of the single-shot trajectory utilized to avoid bulk motion artifacts. Multi-shot acquisitions circumvent the limitations of conventional single-shot EPI and can increase spatial resolution and reduce image distortion at the expense of greater vulnerability to motion-induced phase errors and bulk motion artifacts. In this work, we investigate multi-shot DWI by MUSE reconstruction[2] and a recently proposed method shot-LLR[3] in comparison to conventional single-shot DWI in breast cancer patients.
Methods
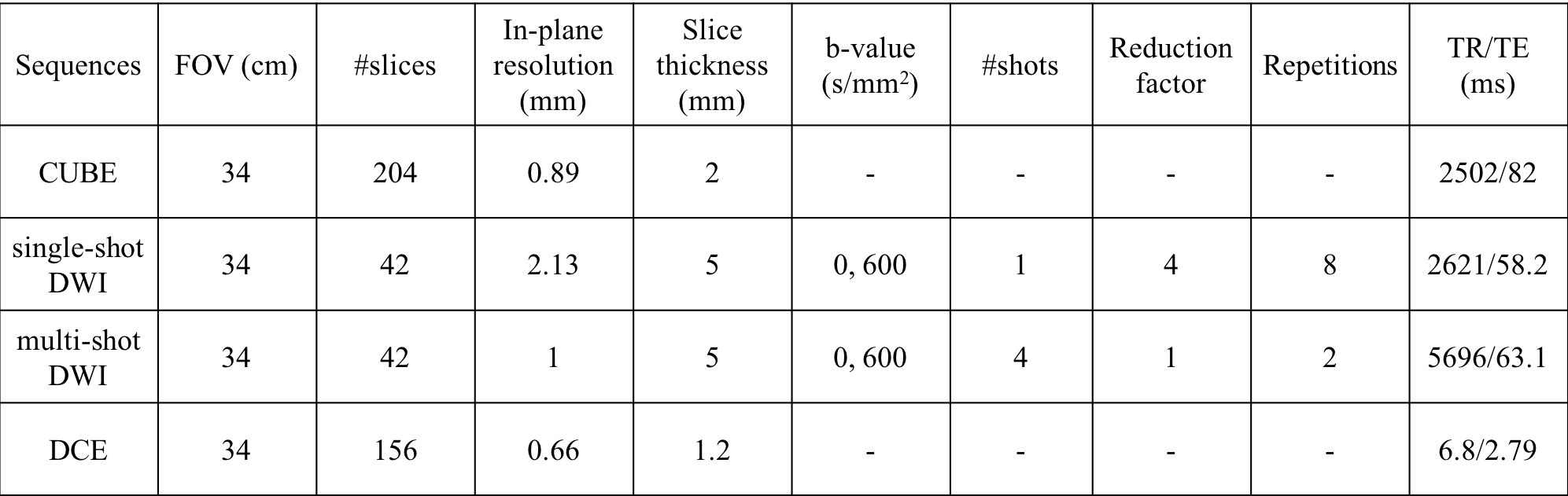
Patient Scans: Following IRB policies and procedures, nine breast patients were recruited and consented to have the multi-shot DWI acquisition added to their clinically ordered breast MRI. All data were acquired on 3T GE MR750 scanners with a 16-channel breast coil. Four sequences were included in the protocol: 1) the routine clinical Dynamic-Contrast Enhanced (DCE) acquisition utilizing the DISCO method, 2) T2 CUBE, 3) single-shot DWI, 4) multi-shot DWI. The acquisition parameters are shown in Table 1. Lesions in each case were identified and characterized by a breast imaging radiologist with extensive breast MRI experience and confirmed through biopsy.
Image reconstruction: GE’s ASSET reconstruction was used to reconstruct single-shot DWI with a reduction factor of 4. Multi-shot images were reconstructed by MUSE and shot-LLR independently. MUSE forms a phase estimation from the results of a SENSE reconstruction on data from each shot. Shot-LLR uses a relaxed model to bypass the phase estimation step and instead uses a locally low-rank (LLR) regularization to exploit shot-to-shot correlations.
For MUSE, calibration data from prescan were used to estimate sensitivity maps. For shot-LLR, non-diffusion-weighted images were used and the sensitivity map was calculated using ESPIRiT[4]. The regularization parameter was 0.008 and number of iterations was 200[3].
Method Comparison
Perceived resolution
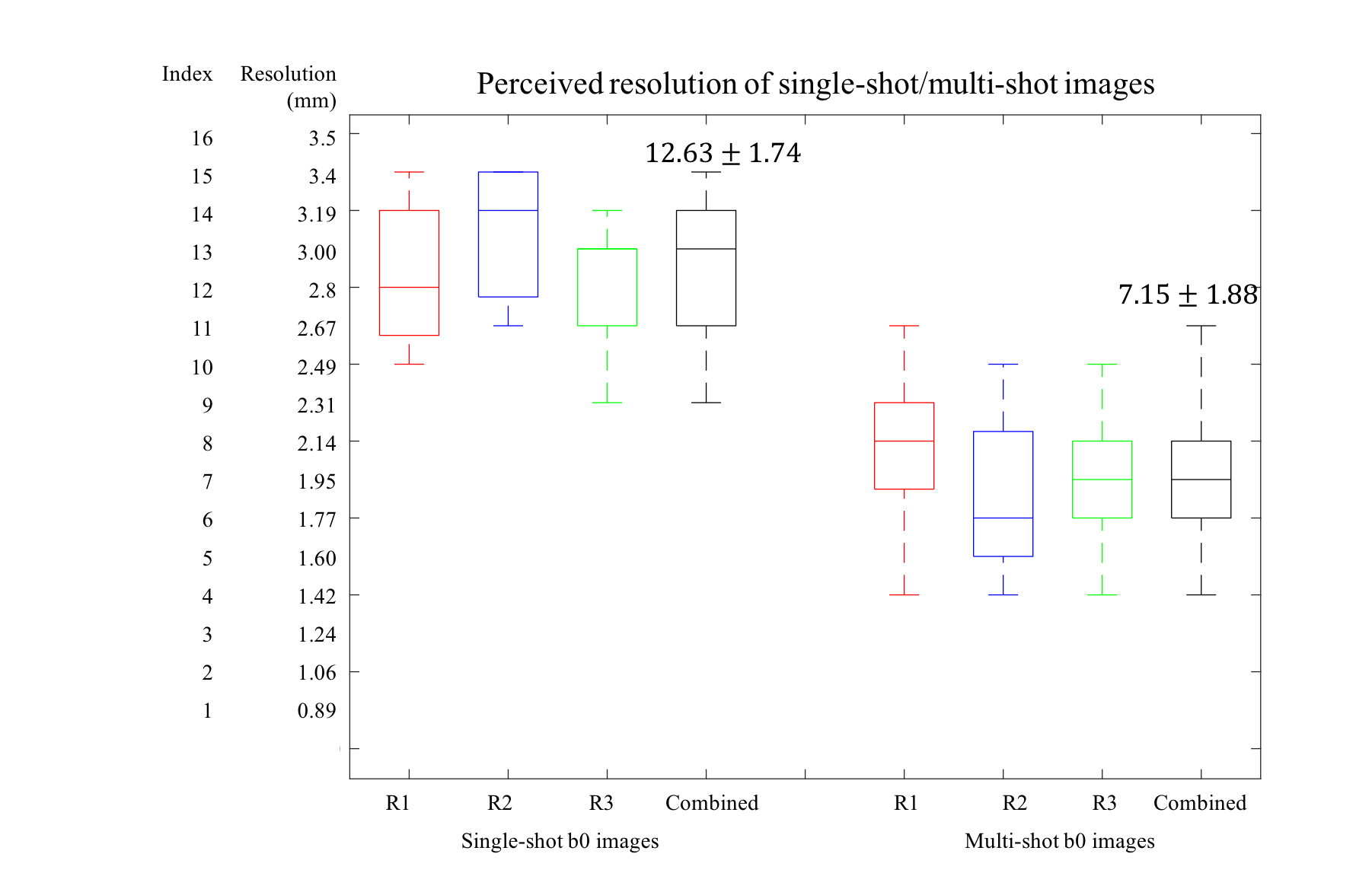
Corresponding T2 CUBE acquisitions originally acquired at 0.89mm⨉0.89mm⨉2mm resolution were first down-sampled along slice encoding direction to 0.89mm⨉0.89mm⨉5mm, then at 16 levels to represent different in-plane image resolutions ranging from 0.89mm to 3.5mm. Three breast imaging radiologists were then presented b0 images from single-shot and multi-shot DWI acquisitions through the lesion as determined by the DCE (peak enhancement), and chose the CUBE image with the closest degree of perceived resolution.
Image quality and lesion characterization
Each observer was then presented with the same slice through the lesion from 5 patients with tumors and rated the following image characteristics:
Lesion conspicuity: (breast lesion conspicuity to uninvolved fibroglandular tissue) 5-point rating scale (1=invisible, 2=barely perceptible, 3=visible but less bright than contrast-enhanced MRI, 4=equivalent to contrast-enhanced MRI, and 5=more conspicuous than on contrast-enhanced MRI).
Depiction of lesion detail: (margins/internal heterogeneity) 5-point rating scale (1=invisible, 2=barely perceptible, 3=visible but less well-defined than on contrast-enhanced MRI, 4=equivalent depiction of lesion morphology to contrast-enhanced MRI, and 5=more detail in lesion morphology than on contrast-enhanced MRI).
Perceived signal to noise ratio (SNR), distortion, aliasing/ghosting artifact: (5 point scale) 1 indicated no or minor things interfering image quality, and 4 or 5 indicated non-diagnostic image.
Results and Discussion
Figure 1 shows the plot of the matching results between b=0 images from single-shot/multi-shot acquisitions and interpolated CUBE T2 images. The multi-shot scans were perceived to achieve significantly (p < 0.05) higher resolution (2mm) than single-shot (3mm).
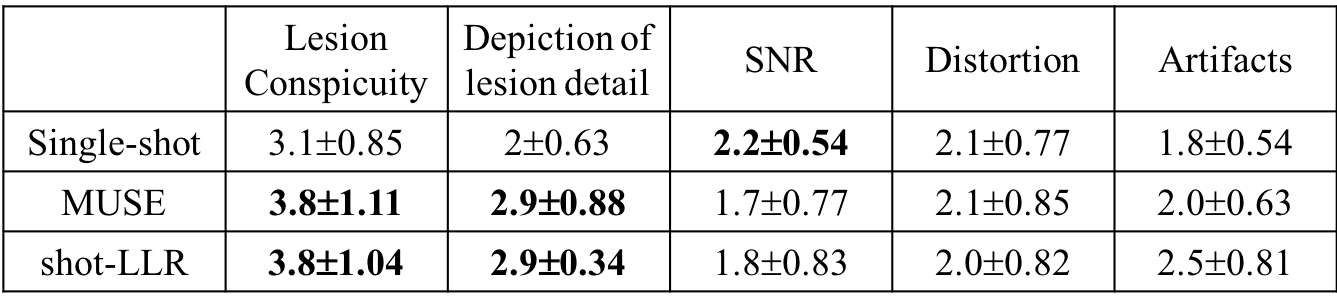
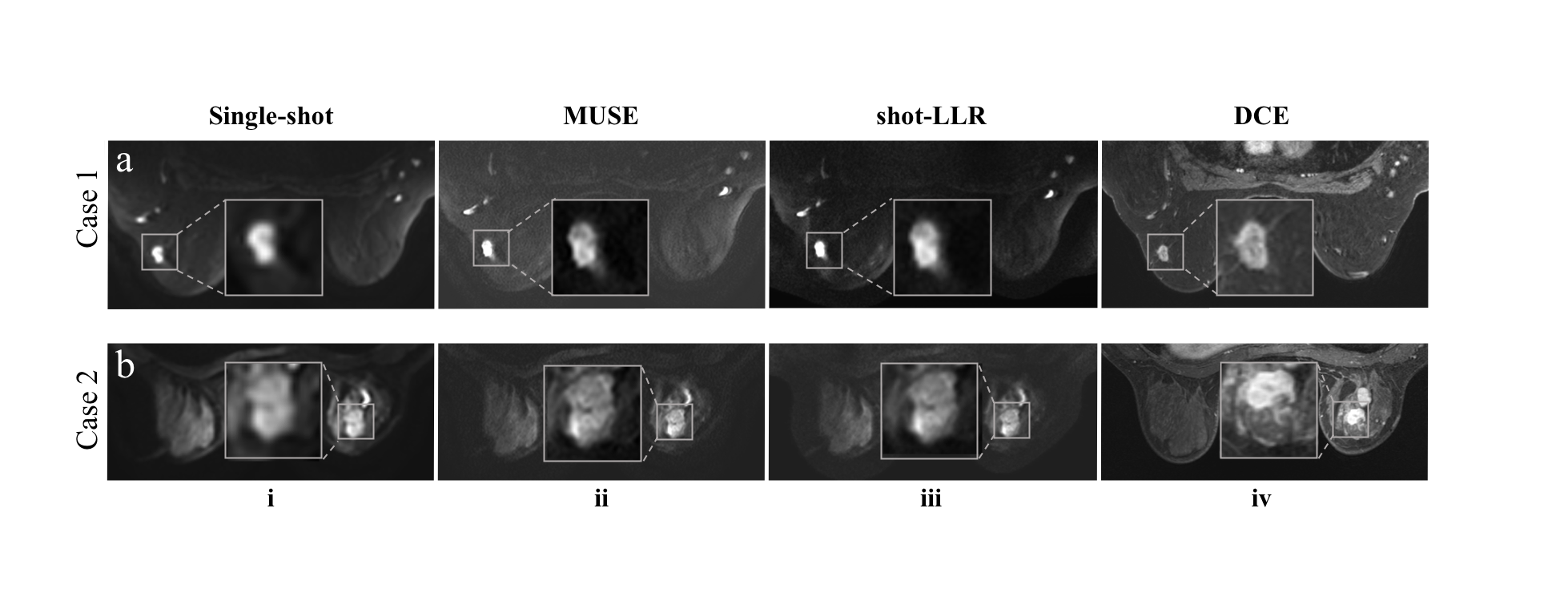
In Table 2, reconstruction results of both MUSE and shot-LLR showed significantly increased lesion conspicuity and depiction of detail compared with single-shot images (p < 0.05). Figure 2 shows two representative cases. The average conspicuity (3.8) indicates multi-shot images achieve almost equivalent performance compared with DCE. Both MUSE and shot-LLR show equal capability to depict the lesion detail, not as well as DCE, but much better than single-shot DWI (p<0.05). Shot-LLR is shown to have more aliasing artifacts, perhaps because the sensitivity map is from non-diffusion-weighted images, which may also have aliasing artifacts. There were no obvious improvements in terms of distortion, since the number of shots was 4. Further increasing this would help decrease distortion and may also show benefits of shot-LLR versus MUSE. The small number of patients limits the statistical analysis, but more cases will be acquired for further studies.
Conclusion
This study demonstrates a substantial improvement in acquired and perceived image sharpness in multi-shot DWI reconstructed by both MUSE and shot-LLR, compared with single-shot DWI.Acknowledgements
Research support from R01-EB009055, P41-EB015891 and GE Healthcare.References
1. Partridge, Savannah C., et al. "Diffusion‐weighted breast MRI: Clinical applications and emerging techniques." Journal of magnetic resonance imaging 45.2 (2017): 337-355.
2. Chen, Nan-kuei, et al. "A robust multi-shot scan strategy for high-resolution diffusion weighted MRI enabled by multiplexed sensitivity-encoding (MUSE)." Neuroimage 72 (2013): 41-47.
3. Hu, Yuxin, et al. "Motion‐robust reconstruction of multishot diffusion‐weighted images without phase estimation through locally low‐rank regularization." Magnetic resonance in medicine (2018).
4. Uecker, Martin, et al. "ESPIRiT—an eigenvalue approach to autocalibrating parallel MRI: where SENSE meets GRAPPA." Magnetic resonance in medicine 71.3 (2014): 990-1001.
Figures