0603
First-in-human: tackling the hypoxic challenge in breast cancer with advanced MRI1Department of Biomedical Imaging and Image-guided Therapy, Medical University of Vienna, Vienna, Austria, 2Department of Neurosurgery, University of Erlangen-Nürnberg, Erlangen, Germany, 3Department of Pathology, Medical University of Vienna, Vienna, Austria, 4Department of Surgery, Medical University of Vienna, Vienna, Austria, 5Department of Internal Medicine, Medical University of Vienna, Vienna, Austria
Synopsis
To develop a novel MRI approach for the non-invasive assessment of hypoxia and neovascularization in benign and malignant breast tumors and to provide insights into the intratumoral heterogeneity of breast cancer. 76 patients with a BI-RADS 4/5 lesion underwent 3T MRI of the breast with Vascular Architecture Mapping (and quantitative Blood Oxygenation Level Dependent (qBOLD) imaging. Our approach demonstrated that breast cancer consumes more oxygen and is more hypoxic and neovascularized than benign tumors. This non-invasive approach can be easily integrated in a diagnostic MRI protocol and has the potential to improve tumor characterization and facilitate tailored breast cancer treatment.
Introduction
In breast cancer tumor hypoxia is one of the key drivers of the development of an aggressive and treatment-resistant tumor phenotype and is a strong prognostic factor for disease progression, metastases, and survival (1-3). In addition, several studies have reported an association between neovascularity and poorer recurrence-free, cancer-specific, and overall survival (4-6)as well as an association with clinical response to chemotherapy (7). The distribution of hypoxia and induced neovascularization are not uniform within a tumor and therefore significantly contribute to BC heterogeneity (2). In breast cancer, a technique that not only depicts tumor hypoxia but also the induced neovascularization and BC heterogeneity is necessary yet currently does not exist. We hypothesized that the non-invasive assessment of hypoxia and neovascularization with MRI is feasible in benign and malignant breast tumors and provides insights into intratumoral heterogeneity. The aim of this study was to develop a novel MRI approach for the non-invasive synergistic assessment of hypoxia and neovascularization in benign and malignant breast tumors, which can be integrated in a diagnostic MRI protocol.Methods
In this IRB-approved prospective study 76 patients with a BI-RADS 4/5 lesion underwent 3T MRI of the breast with Vascular Architecture Mapping (VAM, TE GE/SE, 25/93 ms; TR 1360 ms; 60 measurements, TA 1.4 min, i.v Dotarem, 0.1 mmol/kg body weight) and quantitative Blood Oxygenation Level Dependent (qBOLD) imaging. For qBOLD, T2*- (8 echoes; TR 750 ms; TE 5–40 ms) and T2-mapping sequences (8 echoes; TR 2000 ms; TE 15–120 ms) were performed. Custom-made in-house MatLab software was used for VAM and qBOLD data postprocessing: 1) calculation of tumor blood volume and blood flow maps from GE-EPI DSC data; 2) calculation of T2* and T2 maps; 3) calculation of maps of the oxygen metabolism MRI biomarkers oxygen extraction fraction (OEF) and metabolic rate of oxygen (MRO2); mitochondrial oxygen tension (mitoPO2); and 4) calculation of maps of the vascular architecture MRI biomarkers including microvessel radius (VSI), density (MVD), and type (MTI). Histopathology was used as the goldstandard.Results
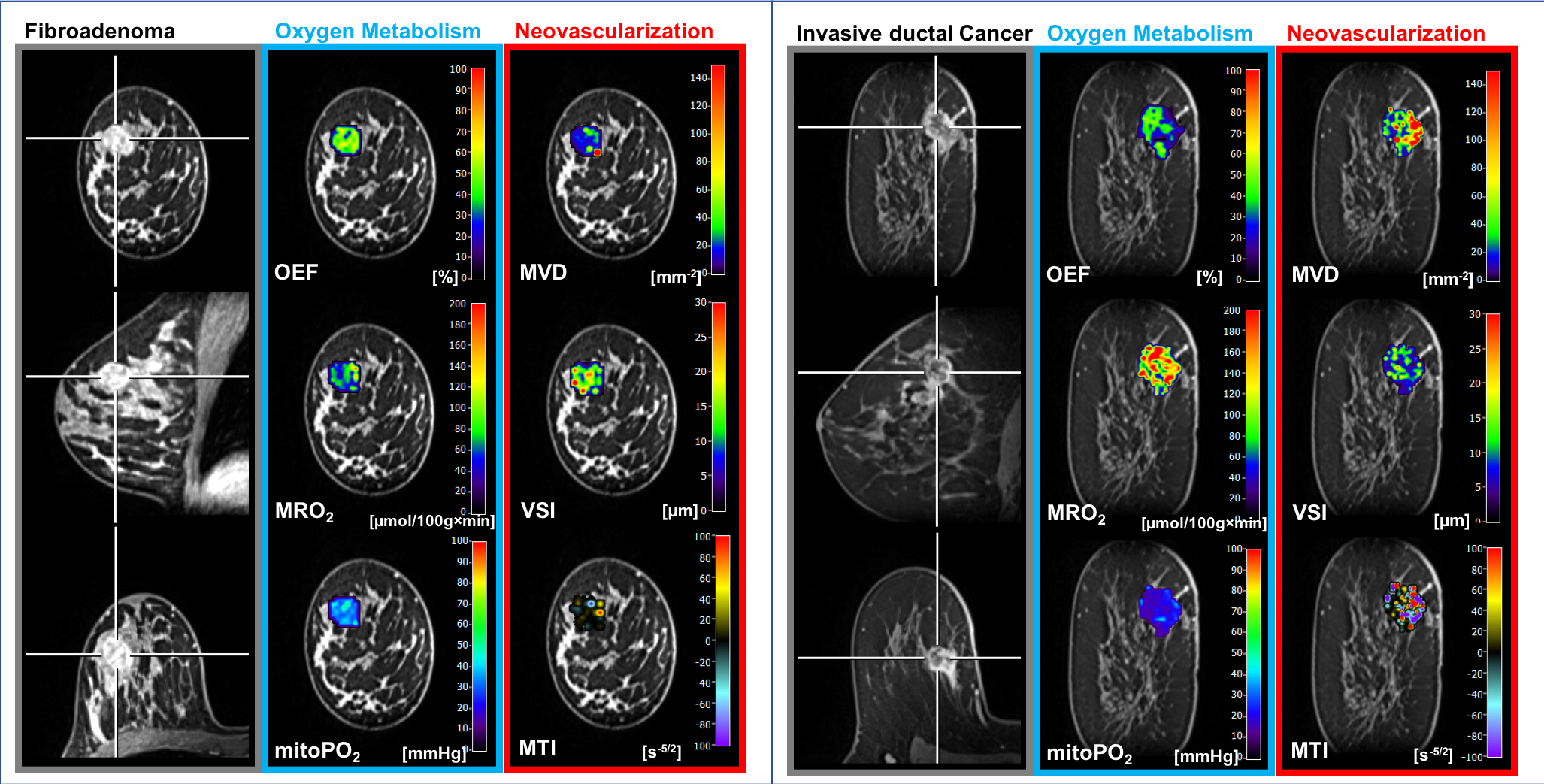
There were 53 malignant (mean tumor volume 6535mm3) and 23 benign (volume 4886 mm3) breast tumors. Non-invasive synergistic assessment of TME hypoxia and angiogenic activity with MRI was successfully performed in all tumors. MRO2 (p=0.013) was significantly higher whereas mitoPO2 (p=0.027) was significantly lower in malignant compared to benign tumors. Malignant tumors showed significantly greater microvessel density (p=0.002) and microvessel type were significantly more tortuous with slow flowing blood (capillary/venous; p=0.002) indicative of the presence angiogenic activity as a hallmark process of cancer development (Fig.1).Discussion
In this study, we developed a novel MRI approach for the non-invasive assessment of hypoxia and neovascularization in benign and malignant breast tumors. The MRI sequences can be easily integrated into a clinical routine MRI protocol, requiring less than 7 min of additional scan time and no additional injection of gadolinium based contrast agents. Our approach demonstrated that breast cancer showed significantly higher MRO2(P= 0.007), lower mitoPO2(P= 0.021), higher MVD (P= 0.005), and lower (i.e. more pathologic) MTI (P= 0.001) compared with benign breast tumors. This indicates that breast cancer consumes more oxygen and is more hypoxic and neovascularized than benign tumors. In the current study MRI biomarker maps of neovascularization, oxygen metabolism, and hypoxia, respectively, showed intratumoral spatial heterogeneity with a broad range of MRI biomarker values. These findings confirm the importance of tumor hypoxia and neovascularization as powerful physiological stimuli that can be exploited as a tumor-specific condition and can be used to design of hypoxia-based imaging biomarkers and hypoxia-activated anti-cancer drugs (8).Conclusion
In this first-in-human study we show that a non-invasive synergistic assessment of TME hypoxia and angiogenic activity with MRI is feasible and enables a differentiation of benign and malignant breast tumors. Synergistic metabolic for the assessment of tumor hypoxia and angiogenic activity provides a novel non-invasive imaging biomarker with the potential to guide therapeutic decisions in breast cancer patients.Acknowledgements
References
1. Ruan K, Song G, Ouyang G. Role of hypoxia in the hallmarks of human cancer. Journal of cellular biochemistry. 2009;107(6):1053-62.
2. Vaupel P. Hypoxia and aggressive tumor phenotype: implications for therapy and prognosis. Oncologist. 2008;13 Suppl 3:21-6.
3. Hockel M, Schlenger K, Mitze M, Schaffer U, Vaupel P. Hypoxia and Radiation Response in Human Tumors. Semin Radiat Oncol. 1996;6(1):3-9.
4. Tsutsui S, Kume M, Era S. Prognostic value of microvessel density in invasive ductal carcinoma of the breast. Breast cancer (Tokyo, Japan). 2003;10(4):312-9.
5. Bevilacqua P, Barbareschi M, Verderio P, Boracchi P, Caffo O, Dalla Palma P, et al. Prognostic value of intratumoral microvessel density, a measure of tumor angiogenesis, in node-negative breast carcinoma--results of a multiparametric study. Breast cancer research and treatment. 1995;36(2):205-17.
6. Al Murri AM, Wilson C, Lannigan A, Doughty JC, Angerson WJ, McArdle CS, et al. Evaluation of the relationship between the systemic inflammatory response and cancer-specific survival in patients with primary operable breast cancer. British journal of cancer. 2007;96(6):891-5.
7. Foekens JA, Peters HA, Grebenchtchikov N, Look MP, Meijer-van Gelder ME, Geurts-Moespot A, et al. High tumor levels of vascular endothelial growth factor predict poor response to systemic therapy in advanced breast cancer. Cancer research. 2001;61(14):5407-14.
8. Vaupel P, Mayer A. The clinical importance of assessing tumor hypoxia: relationship of tumor hypoxia to prognosis and therapeutic opportunities. Antioxid Redox Signal. 2015;22(10):878-80.
Figures